Download as pdf or txt
You might also like
- DIVA-5 Diva 5 Id English FormDocument20 pagesDIVA-5 Diva 5 Id English FormEspíritu Ciudadano93% (28)
- Case 55 BPHDocument4 pagesCase 55 BPHGetachew Addis75% (12)
- Serrapeptase: Studies and Technical InformationDocument6 pagesSerrapeptase: Studies and Technical InformationestiwijayantiNo ratings yet
- 11 Myths of Dentoalveolar SurgeryDocument9 pages11 Myths of Dentoalveolar SurgerydrendodontistNo ratings yet
- El Milagro de La EnzimaDocument172 pagesEl Milagro de La Enzimavictoriacharcas100% (3)
- An Aspirin a Day: The Wonder Drug That Could Save YOUR LifeFrom EverandAn Aspirin a Day: The Wonder Drug That Could Save YOUR LifeNo ratings yet
- The Catch Is That There Really Is No Safe Dose of AspirinDocument4 pagesThe Catch Is That There Really Is No Safe Dose of AspirinSanto ChloNo ratings yet
- A Research On The Physiologic EffectsDocument4 pagesA Research On The Physiologic EffectsmajamorenaNo ratings yet
- 1.STRUKTUR KRISTAL (Kuliah)Document14 pages1.STRUKTUR KRISTAL (Kuliah)RatnaWulannNo ratings yet
- Ibuprofen - Pharmacology, Therapeutics and Side Effects. 2012Document260 pagesIbuprofen - Pharmacology, Therapeutics and Side Effects. 2012VuqarNo ratings yet
- Textbook Essentials of Menopause Management A Case Based Approach Lubna Pal Editor Ebook All Chapter PDFDocument53 pagesTextbook Essentials of Menopause Management A Case Based Approach Lubna Pal Editor Ebook All Chapter PDFjames.gillis956100% (14)
- Drug Prescribing in Oral SurgeryDocument27 pagesDrug Prescribing in Oral SurgeryAsma'a AlmawasNo ratings yet
- Se SN AspirinDocument5 pagesSe SN Aspirinnguyen thu trangNo ratings yet
- Essentials of Menopause Management 2017Document328 pagesEssentials of Menopause Management 2017ErickNo ratings yet
- Tumor Strengths and Frailties - Aspiring To Prevent Colon CancerDocument2 pagesTumor Strengths and Frailties - Aspiring To Prevent Colon CancerJeff ChenNo ratings yet
- Nonsteroidal Antiinflammatorydrugsfor Acuteandchronicpain: Timothy J. Atkinson,, Jeffrey FudinDocument13 pagesNonsteroidal Antiinflammatorydrugsfor Acuteandchronicpain: Timothy J. Atkinson,, Jeffrey FudinMaBe MejíaNo ratings yet
- What You Should Know: D.1 Pharmaceutical Products and Drug Action Drug DevelopmentDocument53 pagesWhat You Should Know: D.1 Pharmaceutical Products and Drug Action Drug DevelopmentRania Samir Shaaban MohamedNo ratings yet
- Aspirin & CancerDocument2 pagesAspirin & CancerEdgardo WerbinNo ratings yet
- Aspirin: Salicylic AcidDocument4 pagesAspirin: Salicylic AcidTius LenaNo ratings yet
- Things You Might Not Know About Aspirin: Three Studies Published TuesdayDocument3 pagesThings You Might Not Know About Aspirin: Three Studies Published TuesdayMohanasundari MuniandyNo ratings yet
- Australian PrescriberDocument3 pagesAustralian PrescriberMohamed OmerNo ratings yet
- Sble2103 Process WritingDocument31 pagesSble2103 Process WritingNuruul HidayahNo ratings yet
- 3 Dangerous DrugsDocument7 pages3 Dangerous DrugsCat CouNo ratings yet
- 16 General PharmacologyDocument19 pages16 General PharmacologyStudy SmarterNo ratings yet
- Ejercicios Clase 6Document3 pagesEjercicios Clase 6roberthtaipevNo ratings yet
- How Do I Know If Aspirin Is Right For Me?: Coronary-Bypass Surgery AngioplastyDocument4 pagesHow Do I Know If Aspirin Is Right For Me?: Coronary-Bypass Surgery Angioplastymaje_leonardoNo ratings yet
- Asian MS Newsletter Spring Issue, 2012Document13 pagesAsian MS Newsletter Spring Issue, 2012AsianMS_SupportGroupNo ratings yet
- Ibuprofen BookDocument259 pagesIbuprofen BookbabithyNo ratings yet
- Journal of International Medical Research 1986 Busson 53 62Document10 pagesJournal of International Medical Research 1986 Busson 53 62Eureka HimitsuNo ratings yet
- Critique of Effects of N 3 Fatty Acid SuDocument12 pagesCritique of Effects of N 3 Fatty Acid SuEde GedeonNo ratings yet
- Archive CourseprintPDF Antiplatelet Medication Response Testing 39435 Fd1744e5 E2ab 490a 9d79 5ef80e99d97aDocument17 pagesArchive CourseprintPDF Antiplatelet Medication Response Testing 39435 Fd1744e5 E2ab 490a 9d79 5ef80e99d97aOmar AlmasriNo ratings yet
- 34 Page Intro The Miracle EnzymeDocument34 pages34 Page Intro The Miracle EnzymeVs GoswamiNo ratings yet
- Ornithogalum Pyrenaicum: Case No. 1Document4 pagesOrnithogalum Pyrenaicum: Case No. 1Barbara Blackburn-PersaudNo ratings yet
- Ibuprofen Safety at The Golden Anniversary 2019Document22 pagesIbuprofen Safety at The Golden Anniversary 2019AMIT JAINNo ratings yet
- PDF 20221116 110548 0000Document19 pagesPDF 20221116 110548 0000rohith jaganNo ratings yet
- Medical Myths Busters: How To Save Billions of Dollars Annually in Health Care CostsDocument67 pagesMedical Myths Busters: How To Save Billions of Dollars Annually in Health Care CostswvornbergerNo ratings yet
- Pharma Chronicle JUly 2011Document55 pagesPharma Chronicle JUly 2011Elmer RicoNo ratings yet
- Aspirina Riesgos y Beneficios - Clev Clin J Med 2013Document9 pagesAspirina Riesgos y Beneficios - Clev Clin J Med 2013Ari JimenezNo ratings yet
- Invitro Dissolution and Assay of "Ibuprofen"Tablet.Document59 pagesInvitro Dissolution and Assay of "Ibuprofen"Tablet.Md.Moniruzzaman100% (3)
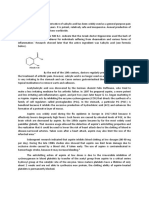
- Revisiting Aspirin, Paracetamol and Ibuprofen: Discovery of Synthetic Procedures and Mode of ActionsDocument4 pagesRevisiting Aspirin, Paracetamol and Ibuprofen: Discovery of Synthetic Procedures and Mode of ActionsbabithyNo ratings yet
- The Pharmaceutical Industry and The Future of Drug Development (RSC Publishing)Document36 pagesThe Pharmaceutical Industry and The Future of Drug Development (RSC Publishing)Ahmed AzzamNo ratings yet
- Cancer Cachexia: Subtitles and TranscriptionsDocument9 pagesCancer Cachexia: Subtitles and TranscriptionsJuan Carlos Carbajal SilvaNo ratings yet
- Cleaning BloodDocument29 pagesCleaning Bloodpjsworld100% (1)
- Sample Press Release - PRDocument3 pagesSample Press Release - PRmyrt88No ratings yet
- TCRM 7 459 PDFDocument13 pagesTCRM 7 459 PDFMikhael JHNo ratings yet
- The History of Aspirin: Reading SkillDocument3 pagesThe History of Aspirin: Reading SkillNabilah PutiNo ratings yet
- Global Initiative For Asthma (GINA), What's New in GINA 2019Document7 pagesGlobal Initiative For Asthma (GINA), What's New in GINA 2019srhmdNo ratings yet
- B1 Assessment 3-The Use and Abuse of DrugsDocument9 pagesB1 Assessment 3-The Use and Abuse of Drugsliam_s143No ratings yet
- Insider Cures Jan2014Document8 pagesInsider Cures Jan2014WalterNo ratings yet
- A History of AspirinDocument3 pagesA History of AspirinMulyaniNo ratings yet
- Chapter 11 Ex. 5: AspirinDocument2 pagesChapter 11 Ex. 5: AspirinLink Worx SeoNo ratings yet
- Ibuprofen - A Journey From Prescription To Over-The-counterDocument5 pagesIbuprofen - A Journey From Prescription To Over-The-counterPharmazellNo ratings yet
- Aspirin, Cyclooxygenase Inhibition and Colorectal Cancer: Carlos Sostres, Carla Jerusalen Gargallo, Angel LanasDocument11 pagesAspirin, Cyclooxygenase Inhibition and Colorectal Cancer: Carlos Sostres, Carla Jerusalen Gargallo, Angel LanasJNHRNo ratings yet
- How To Live Longer and Feel Better - Even With CancerDocument21 pagesHow To Live Longer and Feel Better - Even With CancerMaurizio Pieroni0% (1)
- Daily Aspirin 1Document2 pagesDaily Aspirin 1Anne Marianna FriedrichNo ratings yet
- Daily AspirinDocument2 pagesDaily AspirinUSMP FN ARCHIVOSNo ratings yet
- Daily AspirinDocument2 pagesDaily AspirinGeraldine Quesquen MincholaNo ratings yet
- Omega 3-1Document4 pagesOmega 3-1SyamsulNo ratings yet
- The Effect of Lisinopril On The Desiccation Resistance of Drosophila Melanogaster Anagha Rama Varma 9/22/16Document4 pagesThe Effect of Lisinopril On The Desiccation Resistance of Drosophila Melanogaster Anagha Rama Varma 9/22/16api-308560676No ratings yet
- Final Asthma EssayDocument12 pagesFinal Asthma Essayapi-609379126No ratings yet
- The Best Practice Is The Lowest Effective Dose Your Third Psychiatric Consultation: Diet, Exercise, and Sleep Trump Medications Medication is the Last Option Your Fourth Psychiatric ConsultationFrom EverandThe Best Practice Is The Lowest Effective Dose Your Third Psychiatric Consultation: Diet, Exercise, and Sleep Trump Medications Medication is the Last Option Your Fourth Psychiatric ConsultationNo ratings yet
- Why Stomach Acid Is Good for You: Natural Relief from Heartburn, Indigestion, Reflux and GERDFrom EverandWhy Stomach Acid Is Good for You: Natural Relief from Heartburn, Indigestion, Reflux and GERDRating: 5 out of 5 stars5/5 (1)
- The Journal of Physiology - 2023 - Watkins - Myo Inositol Alters The Effects of Glucose Leptin and Insulin On PlacentalDocument19 pagesThe Journal of Physiology - 2023 - Watkins - Myo Inositol Alters The Effects of Glucose Leptin and Insulin On PlacentalMario CoelhoNo ratings yet
- Evaluation of Anti-Aging Effects of Gemfibrozil OnDocument6 pagesEvaluation of Anti-Aging Effects of Gemfibrozil OnMario CoelhoNo ratings yet
- J American Geriatrics Society - 2014 - Atkins - Sarcopenic Obesity and Risk of Cardiovascular Disease and Mortality ADocument8 pagesJ American Geriatrics Society - 2014 - Atkins - Sarcopenic Obesity and Risk of Cardiovascular Disease and Mortality AMario CoelhoNo ratings yet
- Lvac 001Document9 pagesLvac 001Mario CoelhoNo ratings yet
- Antioxidants 13 00385Document19 pagesAntioxidants 13 00385Mario CoelhoNo ratings yet
- Fnut 09 929891Document11 pagesFnut 09 929891Mario CoelhoNo ratings yet
- A Pilot Study Assessing The Effect of Prolonged Administration of High Daily Doses of Vitamin D On The Clinical Course of Vitiligo and PsoriasisDocument14 pagesA Pilot Study Assessing The Effect of Prolonged Administration of High Daily Doses of Vitamin D On The Clinical Course of Vitiligo and PsoriasisMario CoelhoNo ratings yet
- Vitd th17Document10 pagesVitd th17Mario CoelhoNo ratings yet
- Vit d3Document5 pagesVit d3Mario CoelhoNo ratings yet
- Safety of 5000 International Units Daily Oral Dosing of Vitamin d3 For Four Years in Various Diseases 5f28c908f2e62Document8 pagesSafety of 5000 International Units Daily Oral Dosing of Vitamin d3 For Four Years in Various Diseases 5f28c908f2e62Mario CoelhoNo ratings yet
- Missed Ischemic Stroke Diagnosis in The Emergency Department by Emergency Medicine and Neurology ServicesDocument7 pagesMissed Ischemic Stroke Diagnosis in The Emergency Department by Emergency Medicine and Neurology ServicesReyhansyah RachmadhyanNo ratings yet
- AdhdDocument2 pagesAdhdapi-671375887No ratings yet
- Case # 3Document2 pagesCase # 3Best of pinoyNo ratings yet
- 6 Public Health Issues To Know in 2023 + Jobs Tackling Them - CourseraDocument6 pages6 Public Health Issues To Know in 2023 + Jobs Tackling Them - CourseraUdaai NairNo ratings yet
- Stroke PDFDocument67 pagesStroke PDFBadrul MunirNo ratings yet
- Protocol Needlestick InjuriesDocument1 pageProtocol Needlestick InjuriesMrLarry Dolor100% (1)
- Research Presentation Script I. Background of The Study & Introduction of Research TitleDocument3 pagesResearch Presentation Script I. Background of The Study & Introduction of Research TitleSophia Adel RodriguezNo ratings yet
- Updated Kamin How To Do TheDocument82 pagesUpdated Kamin How To Do TheMarianaMouraNo ratings yet
- Bronchopneumonia JurnalDocument8 pagesBronchopneumonia JurnalMuhd AfizyNo ratings yet
- Virus Hepatitis RevDocument83 pagesVirus Hepatitis RevSukma WinahyuNo ratings yet
- Intestinal Obstruction, Colorectal CancerDocument49 pagesIntestinal Obstruction, Colorectal CancermeghanaNo ratings yet
- Renal - MedbulletsDocument74 pagesRenal - Medbulletssmian08No ratings yet
- Training Manual For Counselors PDFDocument197 pagesTraining Manual For Counselors PDFمخلص منيب اللهNo ratings yet
- 2022 - European Guideline Dermite AtopiqueDocument23 pages2022 - European Guideline Dermite AtopiqueLydia LydiaNo ratings yet
- Practical Research (Qualitative Research: Name: Mackale Jann P. Prado Grade and Section: 11-AristotleDocument4 pagesPractical Research (Qualitative Research: Name: Mackale Jann P. Prado Grade and Section: 11-Aristotlemariane alexa buma-aNo ratings yet
- Brochure Cell DIVE-EN - MC-0002135Document13 pagesBrochure Cell DIVE-EN - MC-0002135histo.haritNo ratings yet
- Community-Acquired Pneumonia in Children - Clinical Features and Diagnosis - UpToDateDocument48 pagesCommunity-Acquired Pneumonia in Children - Clinical Features and Diagnosis - UpToDateAlejandra AubadNo ratings yet
- FinalDocument101 pagesFinalVimal ChauhanNo ratings yet
- 1000 MCQ Bank QuestionsDocument150 pages1000 MCQ Bank Questionsريماالعلي0% (1)
- Breast Cancer Stage IV SampleDocument66 pagesBreast Cancer Stage IV SampleShaira SariaNo ratings yet
- 2021 Nurs3154 Co 2021.01.15Document18 pages2021 Nurs3154 Co 2021.01.15nolifeNo ratings yet
- MUDRASDocument5 pagesMUDRASscsubbaraoNo ratings yet
- PPD PICO Venezia Az'ZahraDocument2 pagesPPD PICO Venezia Az'ZahraMusiani Andi SudiNo ratings yet
- Definition of Antifungal DrugsDocument11 pagesDefinition of Antifungal DrugsShah ZebNo ratings yet
- Paracetamol and CodeineDocument4 pagesParacetamol and CodeineAdhika RahmanNo ratings yet
- Webinar On Osteoarthritis - With Answers To Questions: Barbara MellenDocument6 pagesWebinar On Osteoarthritis - With Answers To Questions: Barbara Mellengeta_dan_846701717No ratings yet
- Coronary Artery Bypass Graft Surgery in Patients With Ischemic Heart FailureDocument31 pagesCoronary Artery Bypass Graft Surgery in Patients With Ischemic Heart Failuresree vidhyaNo ratings yet
- Retina As Window To CNS Disorders - Eye Based Diagnosis of CNS - MS & ALZHEIMER DISEASE - ARDY GISNAWAN (ARD)Document8 pagesRetina As Window To CNS Disorders - Eye Based Diagnosis of CNS - MS & ALZHEIMER DISEASE - ARDY GISNAWAN (ARD)UNHAS OphthalmologyNo ratings yet