Download as pdf or txt
You might also like
- UKOAA - Medical QuestionnaireDocument6 pagesUKOAA - Medical Questionnairemashangh50% (2)
- The Candidate Must Complete Section A of The Form and Submit It To The Med Al Fficer at T e Time of ExaminationDocument4 pagesThe Candidate Must Complete Section A of The Form and Submit It To The Med Al Fficer at T e Time of ExaminationJabdi LobahNo ratings yet
- MLC Medical FormDocument5 pagesMLC Medical FormSoekhaidir SuripnoNo ratings yet
- Introduction of Case StudyDocument6 pagesIntroduction of Case StudyZhengrongShouNo ratings yet
- טפסים לביטוח רפואיDocument3 pagesטפסים לביטוח רפואיmaricelangob3No ratings yet
- FormatDocument3 pagesFormatchiragNo ratings yet
- Lnformation I. (RR+R: Medical QuestionnaireDocument1 pageLnformation I. (RR+R: Medical QuestionnaireMoori G BlackNo ratings yet
- Medical Screening Questionnaire and Examination Record: Social / Occupational History Yes No CommentsDocument4 pagesMedical Screening Questionnaire and Examination Record: Social / Occupational History Yes No CommentsAnnisa DiendaNo ratings yet
- Medical Questionnaire Sept 06Document2 pagesMedical Questionnaire Sept 06Rein Potential Applicant100% (1)
- History Taking FormDocument9 pagesHistory Taking FormEren ErkılınçNo ratings yet
- Medical Certificate For Service at Sea: ConfidentialDocument4 pagesMedical Certificate For Service at Sea: ConfidentialADMIN MCU RSU SAHID SAHIRMAN100% (1)
- MedFest Health History and Physical Exam Form NON US Programs FillableDocument4 pagesMedFest Health History and Physical Exam Form NON US Programs Fillableshariff gutierrezNo ratings yet
- OGUK Medical FormDocument7 pagesOGUK Medical Formum erNo ratings yet
- 5, Ngaporf Seafarer Reebieael Eerfifieate: Marmme and Port Author!Ty of SlngaporeDocument5 pages5, Ngaporf Seafarer Reebieael Eerfifieate: Marmme and Port Author!Ty of SlngaporeinstalasiNo ratings yet
- Sample Form - New Pre-Employment - MEDEX 001Document3 pagesSample Form - New Pre-Employment - MEDEX 001Helmi C MahadyNo ratings yet
- Adult NP PaperworkDocument5 pagesAdult NP Paperworksomethingelse913No ratings yet
- Reflexology New Patient FormDocument7 pagesReflexology New Patient FormOana Iftimie100% (2)
- C105a-Pre-Sea-And-Periodic-Medical-Fitness-Examinations-For-Seafarers - by AstroDocument5 pagesC105a-Pre-Sea-And-Periodic-Medical-Fitness-Examinations-For-Seafarers - by Astroklinik utama Bali Puri MedikaNo ratings yet
- Medical History FormDocument2 pagesMedical History Formapi-279870303No ratings yet
- Health ScreeningDocument3 pagesHealth Screeningpixelkum1No ratings yet
- Hematology CasesDocument10 pagesHematology Casesuyes100% (1)
- Pre AdmissionDocument5 pagesPre AdmissionLaura Margaretha BatlayarNo ratings yet
- Latihan MTK Un SMP BahasDocument2 pagesLatihan MTK Un SMP Bahasdinas pertanianNo ratings yet
- Health History QuestionDocument9 pagesHealth History QuestionSunil Murkikar (GM - PMI Quality Operations)No ratings yet
- 63925fbf4677a6ba79885506 - Medical History FormDocument3 pages63925fbf4677a6ba79885506 - Medical History FormAyunda PutriNo ratings yet
- Medical Second Opinion Request FormDocument5 pagesMedical Second Opinion Request Formapi-380809599No ratings yet
- 2013 MedicalsDocument5 pages2013 MedicalsSebastia Felipe SolisNo ratings yet
- Patient Registration FormDocument5 pagesPatient Registration FormCari WithrowNo ratings yet
- Health Certificate To Work in Confined SpaceDocument6 pagesHealth Certificate To Work in Confined SpacenmmarhelNo ratings yet
- Physical Examination 6Document95 pagesPhysical Examination 6Си Йи ФуNo ratings yet
- Health DeclarationDocument5 pagesHealth Declarationust dol100% (1)
- Medical ReportDocument3 pagesMedical ReportSachitra Nirman MalwatteNo ratings yet
- HM Medical Checkups at Project Sites Medical CampsDocument2 pagesHM Medical Checkups at Project Sites Medical Campsraj kumariNo ratings yet
- Annexure 1Document8 pagesAnnexure 1Abhas GahlotNo ratings yet
- Anglais Médical1Document23 pagesAnglais Médical1Nettah MarouaNo ratings yet
- Health Questionnaire CandidateDocument5 pagesHealth Questionnaire CandidateSaudia Arabia JobsNo ratings yet
- Pre Medical Form PDFDocument11 pagesPre Medical Form PDFNitin KumarNo ratings yet
- Health Declaration For Care 4 U Policy / Medical InsuranceDocument2 pagesHealth Declaration For Care 4 U Policy / Medical InsuranceMarco AglibotNo ratings yet
- Jayla Wright Chart Materials Sim 3Document9 pagesJayla Wright Chart Materials Sim 3tNo ratings yet
- Medical Examination: Subang Polyclinic SDN BHDDocument5 pagesMedical Examination: Subang Polyclinic SDN BHDSubang polylinicNo ratings yet
- New Inpatient Evaluation (History and Physical)Document3 pagesNew Inpatient Evaluation (History and Physical)e-MedTools100% (16)
- Medical Form For Pre-Medical EnrollmentDocument1 pageMedical Form For Pre-Medical EnrollmentFrancine Joyce AguilaNo ratings yet
- Vsim - Edited Clinical WorksheetsDocument8 pagesVsim - Edited Clinical WorksheetsTedra FloydNo ratings yet
- Pe Form (Cosare, Alessandra Maxinne E.-Dmd-1-Canine)Document6 pagesPe Form (Cosare, Alessandra Maxinne E.-Dmd-1-Canine)MoyeonieNo ratings yet
- Your Health PlanDocument9 pagesYour Health PlanMaggie FornaroNo ratings yet
- SA04 Medical Examination Report PDFDocument4 pagesSA04 Medical Examination Report PDFSOU FEI Ang0% (1)
- Adult in TakeDocument9 pagesAdult in TakeNaura CorporationNo ratings yet
- Rellance: Laikshmlovaa PDST, Dasanaputa Holl Tanna LnreDocument16 pagesRellance: Laikshmlovaa PDST, Dasanaputa Holl Tanna LnreSanthosh RNo ratings yet
- Patient History Edited 2019Document3 pagesPatient History Edited 2019api-468186696No ratings yet
- Final Clinical SurgeryDocument107 pagesFinal Clinical SurgeryMahmoud Farag100% (1)
- Neuro PT AssessmentDocument26 pagesNeuro PT AssessmentGetahun TsegayeNo ratings yet
- Part IIDocument64 pagesPart IIhussainNo ratings yet
- Form 86Document8 pagesForm 86Hanna Jane BayarcalNo ratings yet
- Fit To Work Certificate DocxDocument3 pagesFit To Work Certificate DocxBlood ViernesNo ratings yet
- Comprehensive Case Study I AbortionDocument27 pagesComprehensive Case Study I AbortionAmna Sidi MohammadNo ratings yet
- Trip Application FormDocument7 pagesTrip Application Formj_morgan_allen1528No ratings yet
- Progresivve New FormDocument8 pagesProgresivve New FormZahir MalavéNo ratings yet
- Form 86 Medical CertificateDocument4 pagesForm 86 Medical CertificateNARCISO GALAGALANo ratings yet
- 031 Pre Admission ScreeningDocument1 page031 Pre Admission Screeningdohtrc pototanNo ratings yet
- Design of This Case Record Form (CRF) : General GuidanceDocument5 pagesDesign of This Case Record Form (CRF) : General GuidanceCecilia PinedaNo ratings yet
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicFrom EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicRating: 5 out of 5 stars5/5 (1)
- Airway AdjunctsDocument17 pagesAirway AdjunctsChannelGNo ratings yet
- UDAAN2 0UITSscheduleDocument1 pageUDAAN2 0UITSscheduleÀhmèd Kãīf ShãìkhNo ratings yet
- PRP ResearchDocument16 pagesPRP ResearchMaheshNo ratings yet
- THYROIDDocument100 pagesTHYROIDFrance PalNo ratings yet
- Adaptive Architecture and The Prevention of InfectDocument8 pagesAdaptive Architecture and The Prevention of InfectsummiNo ratings yet
- Pathophysiology, Diagnosis and Treatment of Neonatal Sepsis: Review ArticleDocument7 pagesPathophysiology, Diagnosis and Treatment of Neonatal Sepsis: Review ArticleZakia DrajatNo ratings yet
- Microvascular Decompression Treatment For Trigeminal NeuralgiaDocument5 pagesMicrovascular Decompression Treatment For Trigeminal NeuralgiaAkmal Niam FirdausiNo ratings yet
- Manajemen Fisioterapi Pada Cerebral PalsyDocument82 pagesManajemen Fisioterapi Pada Cerebral PalsyBimo AnggoroNo ratings yet
- How To Interpret An Echocardiography Report (For The Non-Imager) ?Document12 pagesHow To Interpret An Echocardiography Report (For The Non-Imager) ?VandeosNo ratings yet
- Classification of Gastrointestinal Cancer Through Explainable AI and Ensemble LearningDocument6 pagesClassification of Gastrointestinal Cancer Through Explainable AI and Ensemble LearningAdhiraj SaxenaNo ratings yet
- Down Syndrome What Is Down Syndrome?Document4 pagesDown Syndrome What Is Down Syndrome?Vanessa Rose NoelNo ratings yet
- Chicken Pox Research PaperDocument5 pagesChicken Pox Research Paperc9rvz6mm100% (1)
- Case ANALYSISDocument2 pagesCase ANALYSISAliyah Kaye Lacdaying RomeroNo ratings yet
- Medical Surgical Nursing - Cardiovascular System DisordersDocument11 pagesMedical Surgical Nursing - Cardiovascular System DisordersSofia LiNo ratings yet
- Zeolita EstudiosDocument5 pagesZeolita EstudiosVulcano JerezNo ratings yet
- Limb Length DiscrepancyDocument8 pagesLimb Length DiscrepancyManish Prasad100% (1)
- Botanicals For Chronic Venous Insufficiency: Alternative and Complementary Therapies December 2007Document9 pagesBotanicals For Chronic Venous Insufficiency: Alternative and Complementary Therapies December 2007Анђела КостићNo ratings yet
- Science, Technology and SocietyDocument14 pagesScience, Technology and SocietyAdrienne CabanigNo ratings yet
- Identify Parts of A News ArticleDocument4 pagesIdentify Parts of A News Articleapi-545873065No ratings yet
- Large As MedicineDocument427 pagesLarge As MedicineFira'ol BogalaNo ratings yet
- Analysis of Volatile Organic Compounds in Exhaled Breath For Detection of Diabetes Mellitus and CholesterolDocument3 pagesAnalysis of Volatile Organic Compounds in Exhaled Breath For Detection of Diabetes Mellitus and CholesterolInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- NCPDocument6 pagesNCPLevyanne GsanchezNo ratings yet
- Nutrilite FiberDocument8 pagesNutrilite FiberJignesh Dhomse100% (1)
- Executive Health Check Up Package - RSPI - Pondok Indah - 2023Document20 pagesExecutive Health Check Up Package - RSPI - Pondok Indah - 2023stephanymelody123No ratings yet
- The Effectiveness of Yoga For Depression A Critical Literature ReviewDocument12 pagesThe Effectiveness of Yoga For Depression A Critical Literature ReviewRahul KhuranaNo ratings yet
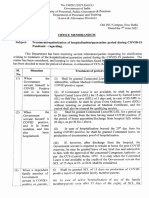
- DoPT Guidelines On Treatment - Regularization of Hospitalization - Quarantine Period During COVID 19 PandemicDocument2 pagesDoPT Guidelines On Treatment - Regularization of Hospitalization - Quarantine Period During COVID 19 PandemictapansNo ratings yet
- Ibbs 2011 IndonesiaDocument80 pagesIbbs 2011 Indonesiarifka yoesoefNo ratings yet
- A Narrative Review of Influenza: A Seasonal and Pandemic DiseaseDocument12 pagesA Narrative Review of Influenza: A Seasonal and Pandemic DiseaseFreddy SueroNo ratings yet
- Occupational Hazards in Textile IndustryDocument20 pagesOccupational Hazards in Textile IndustryShilpa ChaubeyNo ratings yet