Download as pdf or txt
You might also like
- Microbiology The Human Experience 1st Edition Foster Test BankDocument16 pagesMicrobiology The Human Experience 1st Edition Foster Test Bankdavidnelsonseyjdmpoaz100% (13)
- Project 1: Protinex: Market Opportunity Analysis Segmenting, Positioning and BrandingDocument7 pagesProject 1: Protinex: Market Opportunity Analysis Segmenting, Positioning and BrandingEr Piyush Kapoor100% (1)
- UTI Case StudyDocument11 pagesUTI Case StudyEileen Aquino Macapagal100% (3)
- ATS-2023-ePoster D4 16may23 FINALDocument1 pageATS-2023-ePoster D4 16may23 FINAL김현수No ratings yet
- Hybrid Compounds As Direct Multitarget Ligands: A ReviewDocument36 pagesHybrid Compounds As Direct Multitarget Ligands: A ReviewJames TerryNo ratings yet
- Dermatology Handbook 2021 - 2022Document196 pagesDermatology Handbook 2021 - 2022AlexNo ratings yet
- Rec Jan-Des 2020Document16 pagesRec Jan-Des 2020Astri SyadiahNo ratings yet
- Daily Sheetto Be Filled by The UCMO: Area Incharge CodesDocument87 pagesDaily Sheetto Be Filled by The UCMO: Area Incharge CodesdawoodNo ratings yet
- Revised Template of SL and ML For The 12th Cycle ImplementationDocument2 pagesRevised Template of SL and ML For The 12th Cycle Implementationronnie zurbitoNo ratings yet
- Revised Template of SL and ML For The 12th Cycle Implementation 4Document2 pagesRevised Template of SL and ML For The 12th Cycle Implementation 4Emma DionedaNo ratings yet
- 20 New PortalsDocument4 pages20 New PortalssivanayakNo ratings yet
- COVID-19 Treatment and Vaccine Tracker: TreatmentsDocument4 pagesCOVID-19 Treatment and Vaccine Tracker: TreatmentsCeramic TilesNo ratings yet
- Food With Influence in The Sexual and ReDocument9 pagesFood With Influence in The Sexual and ReLeandro VieiraNo ratings yet
- Annex "C" Sars-Cov-2 Claims Summary Form: Patient Information Member InformationDocument3 pagesAnnex "C" Sars-Cov-2 Claims Summary Form: Patient Information Member Informationstewie marsNo ratings yet
- 1 Azad Nagar, Kanpur 2 Kidwai Nagar, Kanpur: Dr. Ajay Kumar Verma (Ms-Pipri - Up@esic - Nic.in)Document1 page1 Azad Nagar, Kanpur 2 Kidwai Nagar, Kanpur: Dr. Ajay Kumar Verma (Ms-Pipri - Up@esic - Nic.in)Ajay Kumar VermaNo ratings yet
- Cancer Nanotechnology A New Revolution For Cancer Diagnosis and TherapyDocument14 pagesCancer Nanotechnology A New Revolution For Cancer Diagnosis and TherapyBrunaNo ratings yet
- Fri 394 Ilc2022Document1 pageFri 394 Ilc2022rtthrtfhNo ratings yet
- Indian EconomyDocument4 pagesIndian Economyvengurlekarsiddhi08No ratings yet
- Norway Gha2009Document1 pageNorway Gha2009Development InitiativesNo ratings yet
- Annex B.2 and B.3 LIPH 2023-2025 Forms 19oct2021Document3 pagesAnnex B.2 and B.3 LIPH 2023-2025 Forms 19oct2021MishelleBainoLadaoNo ratings yet
- PharmasAlmanac Q4 2020Document92 pagesPharmasAlmanac Q4 2020Debjani DuttaNo ratings yet
- Current Prospects of Nutraceuticals - A ReviewDocument13 pagesCurrent Prospects of Nutraceuticals - A ReviewMaria Fernanda Costa Cabral RibeiroNo ratings yet
- Adan, Kiraz, Baran, 2016 - Cell Proliferation and Cytotoxic AssaysDocument9 pagesAdan, Kiraz, Baran, 2016 - Cell Proliferation and Cytotoxic AssaysLu JunqueiraNo ratings yet
- Asian - Basic Statistics 2024Document6 pagesAsian - Basic Statistics 2024ArpitNo ratings yet
- PKM Tanah Abang-BalprasDocument16 pagesPKM Tanah Abang-BalprasDwi rizki KesumaNo ratings yet
- CPhI Russia 2013 Brochure PDFDocument2 pagesCPhI Russia 2013 Brochure PDFctyvteNo ratings yet
- Adweek - October 10, 2022Document46 pagesAdweek - October 10, 2022ganis supriadiNo ratings yet
- 2019 Revised DOST-GIA Form D Semi Annual Progress ReportDocument1 page2019 Revised DOST-GIA Form D Semi Annual Progress ReportApolinar TabañeraNo ratings yet
- 498 Prado et al. - Urochloa and Maize rotationDocument1 page498 Prado et al. - Urochloa and Maize rotationJyonNo ratings yet
- TOC - Project SuperwomanDocument1 pageTOC - Project SuperwomanSulekha BhattacherjeeNo ratings yet
- Doh Peme-Laboratory Dep't December 2020Document1 pageDoh Peme-Laboratory Dep't December 2020MSL LaboratoryNo ratings yet
- Canon Toshiba Ultrasound I-Series FDA 510K SummaryDocument59 pagesCanon Toshiba Ultrasound I-Series FDA 510K SummaryXing LuNo ratings yet
- Health Policy in Portugal July 2016Document2 pagesHealth Policy in Portugal July 2016carlosvalxNo ratings yet
- Annex B.2 and B.3 LIPH 2023-2025 Forms 19oct2021Document3 pagesAnnex B.2 and B.3 LIPH 2023-2025 Forms 19oct2021Rhu Pugo, La UnionNo ratings yet
- Differences Between Adult and Pediatric Septic ShockDocument7 pagesDifferences Between Adult and Pediatric Septic ShockYanna RizkiaNo ratings yet
- Baldeweg 2007Document10 pagesBaldeweg 2007joey lommerseNo ratings yet
- MaxCyte A Versatile Tool For SARS CoV 2 ResponseDocument1 pageMaxCyte A Versatile Tool For SARS CoV 2 ResponsesmileherowarsNo ratings yet
- Company Profile SDocument5 pagesCompany Profile SWitchbladeNo ratings yet
- HC IiDocument32 pagesHC IikakaismaelNo ratings yet
- Possible Side-Effects What The Medicine Is For: Medicated Relief For Mouth & Throat InfectionsDocument2 pagesPossible Side-Effects What The Medicine Is For: Medicated Relief For Mouth & Throat InfectionsLawrence A. DyNo ratings yet
- Towards Universal Coverage in The Majority WorldDocument15 pagesTowards Universal Coverage in The Majority WorldJose Cabrejos PitaNo ratings yet
- Pap ADocument9 pagesPap AlandabureNo ratings yet
- WFP2023Document36 pagesWFP2023Fallucky SantiagoNo ratings yet
- Binder1 4Document11 pagesBinder1 4Cristina-Felicia DeacNo ratings yet
- Department of Education Division of Nueva Ecija Ricardo Dizon Canlas Agricultural SchoolDocument6 pagesDepartment of Education Division of Nueva Ecija Ricardo Dizon Canlas Agricultural SchoolLady In BlackNo ratings yet
- 1 s2.0 S1877050922022414 MainDocument7 pages1 s2.0 S1877050922022414 MainkhusnulNo ratings yet
- Teleperformance-Presentation ProjectDocument44 pagesTeleperformance-Presentation Projectarjunshrivastav6No ratings yet
- InfluenzaDocument1 pageInfluenzaninzah wanzahNo ratings yet
- Flourishing Sustainable Business Canvas 1613959100Document1 pageFlourishing Sustainable Business Canvas 1613959100Vanessa CampitelliNo ratings yet
- Usaid An Icn List DQQ 2022Document1 pageUsaid An Icn List DQQ 2022Samson DesieNo ratings yet
- Unlocking T Cell Potential Multiparameter Characterization of CAR T Cells 1711606816Document1 pageUnlocking T Cell Potential Multiparameter Characterization of CAR T Cells 1711606816pramod226No ratings yet
- Thu 348 Ilc2022Document1 pageThu 348 Ilc2022rtthrtfhNo ratings yet
- Appendix 5 Hazmat Inventory SheetDocument1 pageAppendix 5 Hazmat Inventory Sheetaldrb hospitalNo ratings yet
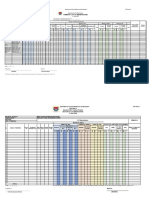
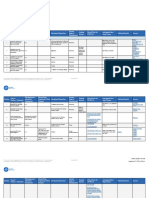
- Monitoring and Surveillance: Immunization in Practice: A Practical Guide For Health Staff-2015 Update (WHO)Document29 pagesMonitoring and Surveillance: Immunization in Practice: A Practical Guide For Health Staff-2015 Update (WHO)Elvin Ryan PlantillaNo ratings yet
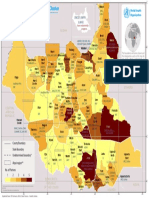
- Total Number of Partners: Ongoing Activities - Health Cluster South Sudan - January 2016Document1 pageTotal Number of Partners: Ongoing Activities - Health Cluster South Sudan - January 2016YenThiLeNo ratings yet
- Webinar 1 Slide Deck With Approved Slides SMRP - For APAC - Handouts - PDFDocument20 pagesWebinar 1 Slide Deck With Approved Slides SMRP - For APAC - Handouts - PDFZekai BingolNo ratings yet
- San Antonio Es Gad Accomplishment Report 2023Document8 pagesSan Antonio Es Gad Accomplishment Report 2023Janeth LayaNo ratings yet
- Usaid An Icn Hemocue Population 2022Document1 pageUsaid An Icn Hemocue Population 2022Samson DesieNo ratings yet
- The Tendency of Stunting Among Children Under Five in The North - 2023 - JornalDocument8 pagesThe Tendency of Stunting Among Children Under Five in The North - 2023 - JornalJuan ZilkyNo ratings yet
- Mitocondrias 2023 PortugalDocument31 pagesMitocondrias 2023 PortugalPriscila FloresNo ratings yet
- COVID19 Weekly Report 30 September 2020 PDFDocument1 pageCOVID19 Weekly Report 30 September 2020 PDFzomikulaNo ratings yet
- Global Hepatitis Report 101-110Document10 pagesGlobal Hepatitis Report 101-110Ştefaniuc IulianNo ratings yet
- Global Hepatitis Report 2024 31-40Document10 pagesGlobal Hepatitis Report 2024 31-40Ştefaniuc IulianNo ratings yet
- Global Hepatitis Report 121-130Document10 pagesGlobal Hepatitis Report 121-130Ştefaniuc IulianNo ratings yet
- Global Hepatitis Report 141-150Document10 pagesGlobal Hepatitis Report 141-150Ştefaniuc IulianNo ratings yet
- Eng 81 90Document10 pagesEng 81 90Ştefaniuc IulianNo ratings yet
- Global Hepatitis Report 2024 11-20Document10 pagesGlobal Hepatitis Report 2024 11-20Ştefaniuc IulianNo ratings yet
- Achilles TendonDocument155 pagesAchilles TendonŞtefaniuc IulianNo ratings yet
- Eng 1 40Document40 pagesEng 1 40Ştefaniuc IulianNo ratings yet
- CV Risc in SLE 5pdfDocument18 pagesCV Risc in SLE 5pdfŞtefaniuc IulianNo ratings yet
- BoneCement PDFDocument9 pagesBoneCement PDFŞtefaniuc IulianNo ratings yet
- From: Case-Fatality Rate and Characteristics of Patients Dying in Relation To COVID-19 in ItalyDocument1 pageFrom: Case-Fatality Rate and Characteristics of Patients Dying in Relation To COVID-19 in ItalyŞtefaniuc IulianNo ratings yet
- Bone Cement and The Implications For Anaesthesia: July 2012Document5 pagesBone Cement and The Implications For Anaesthesia: July 2012Ştefaniuc IulianNo ratings yet
- Harris Hip Score: Please Answer The Following QuestionsDocument2 pagesHarris Hip Score: Please Answer The Following QuestionsŞtefaniuc IulianNo ratings yet
- Juvenile Hallux Valgus PDFDocument14 pagesJuvenile Hallux Valgus PDFŞtefaniuc IulianNo ratings yet
- Dermatological DiagnosisDocument27 pagesDermatological DiagnosisŞtefaniuc IulianNo ratings yet
- Pneumonia in The Intensive Care Unit: Jordi Rello Emili DiazDocument8 pagesPneumonia in The Intensive Care Unit: Jordi Rello Emili DiazMario A. Humeres RNo ratings yet
- Echinostoma IlocanumDocument3 pagesEchinostoma IlocanumChristie Raye NapuliNo ratings yet
- The Pathogenesis of Optic Neuritis Caused by Angiostrongylus Cantonensis in BALB/c MiceDocument12 pagesThe Pathogenesis of Optic Neuritis Caused by Angiostrongylus Cantonensis in BALB/c Miceracut_khansatraNo ratings yet
- English WorkDocument11 pagesEnglish WorkJoyce Nelly Dixon CordobasNo ratings yet
- Cease and Desist Final 17oct2021 3Document85 pagesCease and Desist Final 17oct2021 3Mhinda Army100% (1)
- Gambar Malaria P.falciparumDocument5 pagesGambar Malaria P.falciparumRonalda BudyantaraNo ratings yet
- History - Appendix A - Isolation Precautions - Guidelines Library - Infection Control - CDCDocument2 pagesHistory - Appendix A - Isolation Precautions - Guidelines Library - Infection Control - CDCKomite PPI RSUDPCNo ratings yet
- T136 (Key)Document9 pagesT136 (Key)Uyên Nhi TrươngNo ratings yet
- National Consultation On HIV and HCV Treatment Access Issues REPORTDocument64 pagesNational Consultation On HIV and HCV Treatment Access Issues REPORTbobbyramakantNo ratings yet
- HIV & AIDS - The Prostitute ParadoxDocument2 pagesHIV & AIDS - The Prostitute Paradoxana_smiguelNo ratings yet
- Kamal 2009Document14 pagesKamal 2009seruniallisaaslimNo ratings yet
- Vaccine For AnimalsDocument177 pagesVaccine For AnimalsHeshamKotbNo ratings yet
- Para Lec 1Document23 pagesPara Lec 1stpaulafamilyNo ratings yet
- Article1380380118 - Alim Et AlDocument7 pagesArticle1380380118 - Alim Et AlrenshagullNo ratings yet
- Funding Vaccines For Emerging Infectious DiseasesDocument4 pagesFunding Vaccines For Emerging Infectious Diseasesfadfdafade uohdajufadNo ratings yet
- 2016 ACPL Expanded Content OutlineDocument9 pages2016 ACPL Expanded Content OutlineiisforintheskyNo ratings yet
- Cytomegalovirus Infection and Disease in The New Era of Immunosuppression Following Solid Organ TransplantationDocument9 pagesCytomegalovirus Infection and Disease in The New Era of Immunosuppression Following Solid Organ TransplantationReza Firmansyah IINo ratings yet
- National Guideline For Ipc in Hse Dental and Orthodontic ServicesDocument125 pagesNational Guideline For Ipc in Hse Dental and Orthodontic ServicesSimona BugaciuNo ratings yet
- Shuyun Li Dis-Mm-CurvaDocument14 pagesShuyun Li Dis-Mm-CurvaMARIA ALEJANDRA DE LOS SANTOS ACUNANo ratings yet
- Oropouche Virus As An Emerging Cause of Acute Febrile Illness in ColombiaDocument14 pagesOropouche Virus As An Emerging Cause of Acute Febrile Illness in Colombiajuliana22004No ratings yet
- BRAP PAMET Biosafety Guidance On COVID 19 Testing For Laboratorians EDocument179 pagesBRAP PAMET Biosafety Guidance On COVID 19 Testing For Laboratorians EMM ReyesNo ratings yet
- Chapter 2Document14 pagesChapter 2Um E AbdulSaboorNo ratings yet
- Safety Precautions For Attending Theocratic SchoolsDocument2 pagesSafety Precautions For Attending Theocratic SchoolsRitaNo ratings yet
- Final PresentationDocument43 pagesFinal Presentationapi-608681693No ratings yet
- MicrobiologyDocument17 pagesMicrobiologykimacol659No ratings yet
- Mycobacterium Tuberculosis:: 1. Pulmonary Disease 2. Extra-Pulmonary Disseminated DiseaseDocument3 pagesMycobacterium Tuberculosis:: 1. Pulmonary Disease 2. Extra-Pulmonary Disseminated Diseasesmart_dudeNo ratings yet
- Principles in Antimicrobial Therapy: The Abcs: Benjamin G. Co, MD, FPPS, FpsecpDocument46 pagesPrinciples in Antimicrobial Therapy: The Abcs: Benjamin G. Co, MD, FPPS, FpsecpAayushi AggarwalNo ratings yet