
Posterior Compartment of The Forearm
Posterior Compartment of The Forearm
You might also like
- (download pdf) Human Anatomy 9th Edition Martini Solutions Manual full chapterDocument28 pages(download pdf) Human Anatomy 9th Edition Martini Solutions Manual full chapterpiipiindreaj100% (9)
- Muscles of The Hand & WristDocument43 pagesMuscles of The Hand & WristWasemBhatNo ratings yet
- Elbow RehabilitatioinDocument64 pagesElbow Rehabilitatioinnanahossam12345No ratings yet
- ForearmDocument31 pagesForearmRahaf MajadlyNo ratings yet
- Anterior Compartment of The ForearmDocument55 pagesAnterior Compartment of The ForearmAuza Moses IbrahimNo ratings yet
- Posterior Compartment of ForearmDocument60 pagesPosterior Compartment of Forearmnickmirad2No ratings yet
- Forearm Muscles: DR - Lubna NazliDocument44 pagesForearm Muscles: DR - Lubna NazliPavel OnofreiNo ratings yet
- The HandDocument16 pagesThe HandChidera EmmanuelNo ratings yet
- Forearm PostengDocument20 pagesForearm Postengaliqazal26No ratings yet
- Muscles of The Hand PDocument27 pagesMuscles of The Hand Pmansoorbadshah7809No ratings yet
- Ant Forearm MusclesDocument16 pagesAnt Forearm Musclesrukhsanatariq299No ratings yet
- Anterior Compartment of ForearmDocument25 pagesAnterior Compartment of Forearmromaisa akhtarNo ratings yet
- Muscle - System ANATOMYDocument54 pagesMuscle - System ANATOMYfatimamuzammil406No ratings yet
- Arm, Forearm, Hand MuscleDocument18 pagesArm, Forearm, Hand MusclerabeyaNo ratings yet
- Gross Anatomy of The ForearmDocument52 pagesGross Anatomy of The ForearmADELAJA SAMUELNo ratings yet
- The ForearmDocument26 pagesThe Forearmapi-249972919No ratings yet
- Posterior Compartment of ForearmDocument23 pagesPosterior Compartment of Forearmtaimas sallauNo ratings yet
- 4-Anatomy of The ForearmDocument31 pages4-Anatomy of The ForearmMuostafa KamelNo ratings yet
- Forearm Muscles: Anterior CompartmentDocument9 pagesForearm Muscles: Anterior CompartmentLM KishimotoNo ratings yet
- Upper Limb MusclesDocument10 pagesUpper Limb MusclesfatimaNo ratings yet
- L11 Lower Limb MusclesDocument32 pagesL11 Lower Limb MusclesAbubakar DucaysaneNo ratings yet
- Muscles of Hand: Nimra FarazDocument25 pagesMuscles of Hand: Nimra FarazNimra FarazNo ratings yet
- Muscles of The Upper and Lower LimbsDocument67 pagesMuscles of The Upper and Lower LimbsAngel 冯晓君No ratings yet
- Back of Forearm and Hand-1Document34 pagesBack of Forearm and Hand-1emanNo ratings yet
- 10th Lec Muscles Posterior of ForearmDocument16 pages10th Lec Muscles Posterior of ForearmMudasir razaNo ratings yet
- Lecture 5 MDocument116 pagesLecture 5 MKendidde LucasNo ratings yet
- ElbowDocument35 pagesElbowSanmukhiya Darshit ChandraNo ratings yet
- 13 ShaziabDocument31 pages13 Shaziabtaimourm51No ratings yet
- 11-Extensor Mus ForearmDocument24 pages11-Extensor Mus ForearmIbrahim Adel zaidNo ratings yet
- Anatomy MS WristJointSGDDocument24 pagesAnatomy MS WristJointSGDSpencerNo ratings yet
- Front of Forearm-1Document44 pagesFront of Forearm-1emanNo ratings yet
- Lecct. 2 Muscle 2Document13 pagesLecct. 2 Muscle 2Zaid AbdulqadirNo ratings yet
- Compartment of ThighDocument48 pagesCompartment of Thighhalarajeh2004No ratings yet
- Radial NerveDocument31 pagesRadial Nervek kishlayaNo ratings yet
- Flexor Region of The ForearmDocument13 pagesFlexor Region of The ForearmNeil DolendoNo ratings yet
- Di̇z Eklemi̇ni̇n Anatomi̇si̇ Ve Bi̇yomekani̇ği̇ - Bau (1) - 2Document67 pagesDi̇z Eklemi̇ni̇n Anatomi̇si̇ Ve Bi̇yomekani̇ği̇ - Bau (1) - 2erfan mohammadiNo ratings yet
- ANA L4 - Bones, Joints Muscles of The Upper Limb IIIDocument24 pagesANA L4 - Bones, Joints Muscles of The Upper Limb IIIjexshimadaNo ratings yet
- Anatomy Ii Notes-1-2-1Document66 pagesAnatomy Ii Notes-1-2-1khelianderrick81No ratings yet
- Anatomy of The ArmDocument38 pagesAnatomy of The ArmAkomolede AbosedeNo ratings yet
- ForearmDocument63 pagesForearmolamidealapa2608No ratings yet
- Muscles, Vessels, Nerves of Upper Lower ExtremitiesDocument93 pagesMuscles, Vessels, Nerves of Upper Lower Extremitiescansinunlu1559No ratings yet
- Anaphy ReportDocument28 pagesAnaphy ReportJunaisah P. PangaponNo ratings yet
- 6 Muscles of Forearm FinDocument46 pages6 Muscles of Forearm FinAbdelrhman AbubakrNo ratings yet
- Anatomy (302) - 1Document82 pagesAnatomy (302) - 1Shehzad Noman SajidNo ratings yet
- Anterior ArmDocument6 pagesAnterior ArmandrahlynNo ratings yet
- SGD 8Document3 pagesSGD 8Steph SantosNo ratings yet
- Anatomy Ofthe Upper ArmDocument37 pagesAnatomy Ofthe Upper ArmBenjamin JonathanNo ratings yet
- Anatomy of Hand-2Document24 pagesAnatomy of Hand-2Junaid AhmadNo ratings yet
- Nerves Nerve of Lower LimbDocument33 pagesNerves Nerve of Lower LimbSalsabeel SalamahNo ratings yet
- Lumbo - Sacral PlexusDocument41 pagesLumbo - Sacral Plexushariniselvam95drNo ratings yet
- Anatomy of The ForearmDocument2 pagesAnatomy of The ForearmAmal LadNo ratings yet
- 210420PM PPT - Femoral NerveDocument23 pages210420PM PPT - Femoral NerveAananda Raaj V MNo ratings yet
- Muscles of HandDocument15 pagesMuscles of HandAhmed TarekNo ratings yet
- LG 8Document56 pagesLG 8Joo Se HyukNo ratings yet
- Musculosk UL6 Muscles 4Document45 pagesMusculosk UL6 Muscles 4Zaid HamdanNo ratings yet
- RadialnervepresentationDocument22 pagesRadialnervepresentationmelburnveronNo ratings yet
- Elbow and Antebrachium NotesDocument8 pagesElbow and Antebrachium NoteschadNo ratings yet
- Muscles in The Posterior Compartment of The ThighDocument11 pagesMuscles in The Posterior Compartment of The Thighnandasheeras08No ratings yet
- Gross Anatomy of The Forearm: A CAL Package Designed By-Pratik SinhaDocument24 pagesGross Anatomy of The Forearm: A CAL Package Designed By-Pratik SinhaManvi JogiNo ratings yet
- A Simple Guide to the Voice Box and Its Disorders, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to the Voice Box and Its Disorders, Diagnosis, Treatment and Related ConditionsNo ratings yet
- The HeartDocument56 pagesThe HeartAuza Moses Ibrahim100% (1)
- 8 MediastinumDocument30 pages8 MediastinumAuza Moses Ibrahim100% (2)
- 9 PericardiumDocument19 pages9 PericardiumAuza Moses Ibrahim100% (2)
- Birth DefectsDocument46 pagesBirth DefectsAuza Moses IbrahimNo ratings yet
- Development of CNS and Spinal CordDocument41 pagesDevelopment of CNS and Spinal CordAuza Moses IbrahimNo ratings yet
- Integumentary SystemDocument51 pagesIntegumentary SystemAuza Moses IbrahimNo ratings yet
- Organogenetic PeriodDocument32 pagesOrganogenetic PeriodAuza Moses IbrahimNo ratings yet
- Development of The EarDocument58 pagesDevelopment of The EarAuza Moses IbrahimNo ratings yet
- GASTRULATIONDocument78 pagesGASTRULATIONAuza Moses IbrahimNo ratings yet
- Intro Head and NeckDocument74 pagesIntro Head and NeckAuza Moses Ibrahim100% (2)
- CerebrumDocument38 pagesCerebrumAuza Moses IbrahimNo ratings yet
- Anterior Compartment of The ArmDocument46 pagesAnterior Compartment of The ArmAuza Moses IbrahimNo ratings yet
- Anterior Compartment of The ForearmDocument55 pagesAnterior Compartment of The ForearmAuza Moses IbrahimNo ratings yet
- Axilla and Brachial PlexusDocument67 pagesAxilla and Brachial PlexusAuza Moses IbrahimNo ratings yet
- Anatomy of The Shoulder JointDocument44 pagesAnatomy of The Shoulder JointAuza Moses Ibrahim100% (1)
- Bednar MS, James MA, Light TR. Congenital Longitudinal Deficiency. J Hand Surg Am. 2009Document9 pagesBednar MS, James MA, Light TR. Congenital Longitudinal Deficiency. J Hand Surg Am. 2009AsdfNo ratings yet
- Carpal Instability - 2Document71 pagesCarpal Instability - 2mohammad farhanNo ratings yet
- Neill - A To Z of Bones JT & LigamentDocument272 pagesNeill - A To Z of Bones JT & LigamentPaul Vk100% (1)
- Outcomesof Tendon Transferto Restore Wrist Fingersand Thumb ExtensionDocument7 pagesOutcomesof Tendon Transferto Restore Wrist Fingersand Thumb ExtensionBecky YuliagustinaNo ratings yet
- Anat 51 To 92qDocument48 pagesAnat 51 To 92qMuhieddin GhosnNo ratings yet
- FixinDocument44 pagesFixinJaime EscobarNo ratings yet
- Anatomy 1 - MSS (Upper Limb)Document127 pagesAnatomy 1 - MSS (Upper Limb)Abdullah As'adNo ratings yet
- Resume Miologi Kaki Depan BlakangDocument1 pageResume Miologi Kaki Depan BlakangMade BagiNo ratings yet
- Ulnar Nerve Entrapment Massage Mag Whitney LoweDocument3 pagesUlnar Nerve Entrapment Massage Mag Whitney Lowewolfgangl70No ratings yet
- Plexopathy and MononeuropathyDocument38 pagesPlexopathy and MononeuropathySOUMYADEEP BHUINYANo ratings yet
- Acumed Surgical Technique Modular Hand System HNW00 04 A PDFDocument28 pagesAcumed Surgical Technique Modular Hand System HNW00 04 A PDFBey TaNo ratings yet
- Linear Algebra and Its Applications 5th Edition Lay Test BankDocument26 pagesLinear Algebra and Its Applications 5th Edition Lay Test BankJonathanSwansonbwyi100% (52)
- 1-Muscle of Upper Extremeties-TableDocument4 pages1-Muscle of Upper Extremeties-TableJan JeminoNo ratings yet
- Anatomy of The Hand: Khalid AyoubDocument53 pagesAnatomy of The Hand: Khalid Ayoubvaikunthan100% (2)
- Frog MusclesDocument1 pageFrog MusclesFama VicencioNo ratings yet
- Looking Again at The Forelimb of Tyrannosaurus Rex: Christine Lipkin and Kenneth CarpenterDocument25 pagesLooking Again at The Forelimb of Tyrannosaurus Rex: Christine Lipkin and Kenneth CarpenternomadNo ratings yet
- OinaDocument19 pagesOinaPauline JaleaNo ratings yet
- Wrist and Hand Complex BiomechanicsDocument94 pagesWrist and Hand Complex BiomechanicsManu kafeelNo ratings yet
- Soft Tissue Disorders and Fibromyalgia: Jaya Ravindran Consultant RheumatologistDocument54 pagesSoft Tissue Disorders and Fibromyalgia: Jaya Ravindran Consultant RheumatologistarunupadhayaNo ratings yet
- Female Muscle DiagramDocument1 pageFemale Muscle DiagrammakukikiNo ratings yet
- Distal Radial and Ulnar Arteries: The Alternative Forearm AccessDocument12 pagesDistal Radial and Ulnar Arteries: The Alternative Forearm AccessAlejandro Vazquez ManniseNo ratings yet
- Bio Mechanics of The ElbowDocument56 pagesBio Mechanics of The ElbowOnwaree Ing100% (4)
- ANATOMY Multiple Choice Questions 2012Document39 pagesANATOMY Multiple Choice Questions 2012kishorechandra100% (5)
- Nerve InjuriesDocument3 pagesNerve InjuriesAmber MerrittNo ratings yet
- Evolve Proline Operative TechniqueDocument20 pagesEvolve Proline Operative TechniqueRadomir CzajkaNo ratings yet
- Oina MusclesDocument73 pagesOina MusclesShen AndradeNo ratings yet
- Uts AnatomiDocument18 pagesUts AnatomiSuratmi UnnesNo ratings yet
- STT Tecnica QuirúrgicaDocument5 pagesSTT Tecnica QuirúrgicaNathaly GuevaraNo ratings yet
- Medical Picture Mnemonics PDFDocument28 pagesMedical Picture Mnemonics PDFAntoine JusticeNo ratings yet


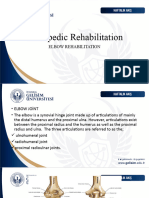



































































































UPPER AND LOWER LIMB
ANA 211
Posterior compartment of the
Forearm
Auza, M I (BSc, MSc)
Department of Human Anatomy
Faculty of Basic Medical Sciences
Bingham University, Karu
WISDOM QUOTE
"If you run after
knowledge,
goodness and mercy will
run after you.“
Proverbs 1:22,29-33
Introduction
• The muscles in the posterior compartment of the forearm are
commonly known as the extensor muscles.
• The general function of these muscles is to
• Produce extension at the wrist and fingers.
• They are all innervated by the
• Radial nerve.
• The muscles in this compartment are organised into two layers;
• Superficial layer
• Deep layer
• These two layers are separated by a layer of fascia.
Superficial Muscles
• The superficial layer of the posterior forearm contains
seven muscles they are:
• Extensor carpi radialis brevis,
• Extensor carpi radialis longus
• Extensor carpi ulnaris
• Extensor digiti minimi
• Extensor digitorum,
• Brachioradialis
• Anconeus
NB
• All the seven muscles cross the elbow joint
Superficial Muscles
• The superficial muscles of the back of the forearm are
further divided into two groups
• Lateral group
• Posterior group
S/N Posterior Group Lateral Group
1 Extensor digitorum Brachioradialis
2 Extensor digiti minimi Extensor carpi radialis longus
3 Extensor carpi ulnaris Extensor carpi radialis brevis
4 Anconeus
Superficial Muscles
• The superficial layer of the posterior forearm contains
seven muscles.
• Four out of seven of these superficial muscles share a
common tendinous origin at the lateral epicondyle of the
humerus called common extensor origin and they are:
• Extensor carpi radialis brevis,
• Extensor carpi ulnaris
• Extensor digiti minimi
• Extensor digitorum
Lateral aspect of the lower end of humerus showing origin of seven superficial muscles of the back of
forearm (ECRB = extensor carpi radialis brevis, ED = extensor digitorum, EDM = extensor digiti minimi,
ECU = extensor carpi ulnaris).
Brachioradialis
• The brachioradialis is a paradoxical muscle.
• Its origin and innervation are characteristic of
an extensor muscle, but it is actually a flexor
at the elbow.
Attachments:
• Originates from the proximal aspect of the
lateral supracondylar ridge of humerus
• Attaches to the distal end of the radius, just
before the radial styloid process.
Actions:
• Flexes at the elbow.
Innervation: Radial nerve
Extensor Carpi Radialis Longus (ECRL)
and Brevis (ECRB)
• The extensor carpi radialis muscles are
situated on the lateral aspect of the
posterior forearm.
• Due to their position, they are able to
produce abduction as well as extension
at the wrist.
Attachments:
• ECRL originates from the lateral
supracondylar ridge of the humerus
• ECRB originates from the lateral
epicondyle.
• Their tendons attach to metacarpal
bones II and III.
Actions:
• Extends and abducts the wrist.
Insertion of the extensor carpi ulnaris, extensor carpi
Innervation: Radial nerve. radialis longus, and extensor carpi radialis brevis.
Extensor Digitorum Communis
• The extensor digitorum is the main
extensor of the fingers.
• To test the function of the muscle, the
forearm is pronated, and the fingers
extended against resistance.
Attachments:
• Originates from the lateral epicondyle.
• The tendon continues into in the distal
part of the forearm, where it splits into
four
• Inserts into the extensor hood of each
finger.
Actions:
• Extension of the digits at the
interphalangeal and metacarpophalangeal
joints.
Innervation: Radial nerve (deep branch).
Insertion of the extensor digitorum, extensor carpi
ulnaris, and extensor indicis
Extensor Digiti Minimi
• The extensor digiti minimi is thought to originate from the extensor
digitorum muscle.
• In some people, these two muscles are fused together.
• Anatomically, the extensor digiti minimi lies medially to the extensor
digitorum.
Attachments:
• Originates from the lateral epicondyle of the humerus.
• It attaches, with the extensor digitorum tendon, into the extensor
hood of the little finger.
Actions:
• Extends the little finger, and contributes to extension at the wrist.
Innervation: Radial nerve (deep branch).
Extensor Carpi Ulnaris
• The extensor carpi ulnaris is located on the medial aspect of
the posterior forearm.
• Due to its position, it is able to produce adduction as well as
extension at the wrist.
Attachments:
• Originates from the lateral epicondyle of the humerus, and
• Attaches to the base of metacarpal V.
Actions:
• Extension and adduction of wrist.
Innervation: Radial nerve (deep branch).
Anconeus
• The anconeus is situated medially and proximally in the
extensor compartment of the forearm.
• It is blended with the fibres of the triceps brachii, and the
two muscles can be indistinguishable
Attachments:
• Originates from the lateral epicondyle
• Attaches to the posterior and lateral part of the olecranon.
Actions:
• Extends and stablises the elbow joint.
• Abducts the ulna during pronation of the forearm.
Innervation: Radial nerve.
Deep Muscles
• There are five muscles in the
deep compartment of the
posterior forearm
• Supinator
• Abductor Pollicis Longus
• Extensor Pollicis Brevis
• Extensor Pollicis Longus
• Extensor Indicis
With the exception of the
supinator, these muscles act on
the thumb and the index finger.
Supinator
• The supinator lies in the floor of the
cubital fossa.
• It has two heads, which the deep
branch of the radial nerve passes
between.
Attachments: It has two heads of origin.
• One originates from the lateral
epicondyle of the humerus, the other
originates from the posterior surface
of the ulna.
• They insert together into the posterior
surface of the radius.
Actions:
• Supinates the forearm.
Innervation: Radial nerve (deep branch).
Abductor Pollicis Longus
• The Abductor Pollicis Longus is situated immediately distal to
the supinator muscle.
• In the hand, its tendon contributes to the lateral border of the
anatomical snuffbox.
Attachments:
• Originates from the interosseous membrane and the adjacent
posterior surfaces of the radius and ulna.
• Attaches to the lateral side of the base of metacarpal I.
Actions:
• Abducts the thumb.
Innervation: Radial nerve (posterior interosseous branch).
Extensor Pollicis Brevis
• The Extensor Pollicis Brevis can be found medially and deep to
the abductor pollicis longus.
• In the hand, its tendon contributes to the lateral border of the
anatomical snuffbox.
Attachments:
• Originates from the posterior surface of the radius and
interosseous membrane.
• Attaches to the base of the proximal phalanx of the thumb.
Actions:
• Extends at the metacarpophalangeal and carpometacarpal joints
of the thumb.
Innervation: Radial nerve (posterior interosseous branch).
Extensor Pollicis Longus
• The Extensor Pollicis Longus muscle has a larger muscle belly than the
EPB.
• The tendon of the extensor pollicis longus forms the medial border of
the anatomical snuffbox in the hand.
• Attachments:
• Originates from the posterior surface of the ulna and interosseous
membrane.
• Attaches to the distal phalanx of the thumb.
Actions: Extends all joints of the thumb: carpometacarpal,
metacarpophalangeal and interphalangeal.
• Innervation: Radial nerve (posterior interosseous branch).
Extensor Indicis Proprius
• This muscle Extensor Indicis allows the index finger to be
independent of the other fingers during extension.
Attachments:
• Originates from the posterior surface of the ulna and
interosseous membrane, distal to the extensor pollicis
longus.
• Attaches to the extensor hood of the index finger.
Actions:
• Extends the index finger.
Innervation: Radial nerve (posterior interosseous branch).
Clinical Relevance: Wrist Drop
• Wrist drop is a sign of radial nerve injury that has occurred proximal
to the elbow.
• There are two common characteristic sites of damage:
• Axilla – injured via humeral dislocations or fractures of the proximal humerus.
• Radial groove of the humerus – injured via a humeral shaft fracture.
• The radial nerve innervates all muscles in the extensor compartment
of the forearm.
• In the event of a radial nerve lesion, these muscles are paralyzed.
• The muscles that flex the wrist are innervated by the median nerve,
and thus are unaffected.
• The tone of the flexor muscles produces unopposed flexion at the
wrist joint – wrist drop.
Posterior Interosseous Nerve: Origin
And Course
• The posterior interosseous
nerve is the deep terminal
branch of the radial nerve.
• It is motor and chief nerve of
the back of the forearm.
• It begins in the cubital fossa as
one of the two terminal branches
of radial nerve at the level of
lateral epicondyle of humerus.
• It leaves the cubital fossa by
winding around the lateral side
of the neck of radius in the
substance of supinator.
Posterior Interosseous Nerve: Origin
And Course
• After emerging from
supinator, it runs in the
fascial plane between
superficial and deep extensor
muscles.
• At the lower border of
extensor pollicis brevis, it
passes deep to the extensor
pollicis longus to lie on the
posterior surface of
interosseous nerve, on which it
runs downwards up to the
wrist where it ends into a
pseudoganglion.
Branches of Posterior Interosseous
Nerve : Muscular branches
• Before piercing supinator, it gives
branches to the
• Extensor carpi radialis brevis and
• Supinator.
• While passing through supinator, it
gives another branch to the supinator
• After emerging from supinator, it
gives branches to three superficial
extensors:
• Extensor digitorum
• Extensor digiti minimi
• Extensor carpi ulnaris and
• All Deep Extensors
Branches of Posterior Interosseous
Nerve : Articular branches
• Articular branches to the wrist joint, distal radio-ulnar
joint, and carpal joints.
N.B.
• All the muscles on the back of forearm are supplied by the
posterior interosseous nerve except:
• Brachioradialis,
• Extensor carpi radialis longus, and
• Anconeus, which are supplied by the radial nerve directly.
Clinical correlation
Lesion of posterior interosseous nerve:
• The posterior interosseous nerve (i.e., deep
terminal branch of the radial nerve) may be
damaged during surgical exposure of the head
of radius in fracture proximal end of radius.
• Since the extensor carpi radialis longus is
spared wrist drop does not occur.
Arterial Supply: Posterior
Interosseous Artery
• The posterior interosseous artery is a smaller terminal
branch of the common interosseous artery from ulnar
artery.
• It begins in the cubital fossa, enters the back of the
forearm by passing through the gap between the oblique
cord and upper margin of the interosseous membrane.
• From here, it passes between supinator and abductor pollicis
longus to accompany the posterior interosseous nerve.
Course and relations of the posterior interosseous artery
Arterial Supply: Posterior
Interosseous Artery
• In the lower part of the forearm, it becomes markedly
reduced and ends by anastomosing with the anterior
interosseous artery.
• In the lower part of forearm, the anterior interosseous
artery enters the back of the forearm by piercing
interosseous membrane just above the pronator quadratus
and supplies low one-fourth of the back of the forearm.
• The posterior interosseous artery in the cubital fossa gives
interosseous recurrent artery, which takes part in the
formation of anastomosis around the elbow joint.
ANATOMICAL SNUFF-BOX
• The anatomical snuffbox (also
known as the radial fossa)
• It is a triangular depression
found on the lateral aspect of
the dorsum of the hand when
the thumb is hyperextended
• It is located at the level of the
carpal bones, and best seen
when the thumb is extended.
• In the past, this depression was
used to hold snuff(grounded
tobacco) before inhaling via the
nose – hence it was given the
name ‘snuffbox’.
Borders or Boundaries
Posteromedially: Ulnar (medial)
border
• Tendon of the extensor pollicis longus.
Anterolaterally: Radial (lateral)
border:
• Tendons of the extensor pollicis
brevis
• Tendons of the abductor pollicis
longus.
Proximal border:
• Styloid process of the radius.
NB
Borders or Boundaries
Floor:
Carpal bones;
•Scaphoid and
•Trapezium.
Roof:
•Skin
•Superficial fascia
Contents
• The main contents of
the anatomical
snuffbox are the;
• Radial artery
• A branch of the
radial nerve
• Cephalic vein
Boundaries and contents of the anatomical snuffbox
(S = scaphoid).
Contents
Radial artery
• Crosses the floor of the
anatomical snuffbox, then
turns medially and travels
between the heads of the
adductor pollicis muscle.
• The radial pulse can be
palpated in some individuals
by placing two fingers on
the proximal portion of the
anatomical snuffbox.
Contents
Superficial branch of the
radial nerve
• Found in the skin and
subcutaneous tissue of
the anatomical snuffbox.
• It innervates the dorsal
surface of the lateral
three and half digits,
and the associated area
on the back of the hand.
Contents
Cephalic vein
• Arises from the
dorsal venous
network of the hand
and crosses the
anatomical snuffbox
to travel up the
anterolateral aspect
of the forearm.
Clinical correlation
Clinical significance of anatomical snuff box
• The pulsations of radial artery can be felt in the
anatomical box.
• The tenderness in the anatomical box indicates fracture of
scaphoid bone.
• The cephalic vein at this site is often used for giving
intravenous fluids.
• The superficial branches of the radial nerve can be rolled
over the tendon of extensor pollicis longus.
Clinical Relevance: Scaphoid Fracture
• The scaphoid bone of the hand is the most commonly fractured
carpal bone – typically by falling on an outstretched hand.
• In a fracture of the scaphoid, the characteristic clinical feature
is pain and tenderness in the anatomical snuffbox.
• The scaphoid is at particular risk of avascular necrosis after
fracture because of its so-called ‘retrograde blood supply’ which
enters at its distal end.
• This means that a fracture to the middle (or ‘waist’) of the
scaphoid may interrupt the blood supply to the proximal part
of the scaphoid bone rendering it avascular.
• Patients with a missed scaphoid fracture are likely to develop
osteoarthritis of the wrist in later life.
Radiograph of a fractured scaphoid
You might also like
- (download pdf) Human Anatomy 9th Edition Martini Solutions Manual full chapterDocument28 pages(download pdf) Human Anatomy 9th Edition Martini Solutions Manual full chapterpiipiindreaj100% (9)
- Muscles of The Hand & WristDocument43 pagesMuscles of The Hand & WristWasemBhatNo ratings yet
- Elbow RehabilitatioinDocument64 pagesElbow Rehabilitatioinnanahossam12345No ratings yet
- ForearmDocument31 pagesForearmRahaf MajadlyNo ratings yet
- Anterior Compartment of The ForearmDocument55 pagesAnterior Compartment of The ForearmAuza Moses IbrahimNo ratings yet
- Posterior Compartment of ForearmDocument60 pagesPosterior Compartment of Forearmnickmirad2No ratings yet
- Forearm Muscles: DR - Lubna NazliDocument44 pagesForearm Muscles: DR - Lubna NazliPavel OnofreiNo ratings yet
- The HandDocument16 pagesThe HandChidera EmmanuelNo ratings yet
- Forearm PostengDocument20 pagesForearm Postengaliqazal26No ratings yet
- Muscles of The Hand PDocument27 pagesMuscles of The Hand Pmansoorbadshah7809No ratings yet
- Ant Forearm MusclesDocument16 pagesAnt Forearm Musclesrukhsanatariq299No ratings yet
- Anterior Compartment of ForearmDocument25 pagesAnterior Compartment of Forearmromaisa akhtarNo ratings yet
- Muscle - System ANATOMYDocument54 pagesMuscle - System ANATOMYfatimamuzammil406No ratings yet
- Arm, Forearm, Hand MuscleDocument18 pagesArm, Forearm, Hand MusclerabeyaNo ratings yet
- Gross Anatomy of The ForearmDocument52 pagesGross Anatomy of The ForearmADELAJA SAMUELNo ratings yet
- The ForearmDocument26 pagesThe Forearmapi-249972919No ratings yet
- Posterior Compartment of ForearmDocument23 pagesPosterior Compartment of Forearmtaimas sallauNo ratings yet
- 4-Anatomy of The ForearmDocument31 pages4-Anatomy of The ForearmMuostafa KamelNo ratings yet
- Forearm Muscles: Anterior CompartmentDocument9 pagesForearm Muscles: Anterior CompartmentLM KishimotoNo ratings yet
- Upper Limb MusclesDocument10 pagesUpper Limb MusclesfatimaNo ratings yet
- L11 Lower Limb MusclesDocument32 pagesL11 Lower Limb MusclesAbubakar DucaysaneNo ratings yet
- Muscles of Hand: Nimra FarazDocument25 pagesMuscles of Hand: Nimra FarazNimra FarazNo ratings yet
- Muscles of The Upper and Lower LimbsDocument67 pagesMuscles of The Upper and Lower LimbsAngel 冯晓君No ratings yet
- Back of Forearm and Hand-1Document34 pagesBack of Forearm and Hand-1emanNo ratings yet
- 10th Lec Muscles Posterior of ForearmDocument16 pages10th Lec Muscles Posterior of ForearmMudasir razaNo ratings yet
- Lecture 5 MDocument116 pagesLecture 5 MKendidde LucasNo ratings yet
- ElbowDocument35 pagesElbowSanmukhiya Darshit ChandraNo ratings yet
- 13 ShaziabDocument31 pages13 Shaziabtaimourm51No ratings yet
- 11-Extensor Mus ForearmDocument24 pages11-Extensor Mus ForearmIbrahim Adel zaidNo ratings yet
- Anatomy MS WristJointSGDDocument24 pagesAnatomy MS WristJointSGDSpencerNo ratings yet
- Front of Forearm-1Document44 pagesFront of Forearm-1emanNo ratings yet
- Lecct. 2 Muscle 2Document13 pagesLecct. 2 Muscle 2Zaid AbdulqadirNo ratings yet
- Compartment of ThighDocument48 pagesCompartment of Thighhalarajeh2004No ratings yet
- Radial NerveDocument31 pagesRadial Nervek kishlayaNo ratings yet
- Flexor Region of The ForearmDocument13 pagesFlexor Region of The ForearmNeil DolendoNo ratings yet
- Di̇z Eklemi̇ni̇n Anatomi̇si̇ Ve Bi̇yomekani̇ği̇ - Bau (1) - 2Document67 pagesDi̇z Eklemi̇ni̇n Anatomi̇si̇ Ve Bi̇yomekani̇ği̇ - Bau (1) - 2erfan mohammadiNo ratings yet
- ANA L4 - Bones, Joints Muscles of The Upper Limb IIIDocument24 pagesANA L4 - Bones, Joints Muscles of The Upper Limb IIIjexshimadaNo ratings yet
- Anatomy Ii Notes-1-2-1Document66 pagesAnatomy Ii Notes-1-2-1khelianderrick81No ratings yet
- Anatomy of The ArmDocument38 pagesAnatomy of The ArmAkomolede AbosedeNo ratings yet
- ForearmDocument63 pagesForearmolamidealapa2608No ratings yet
- Muscles, Vessels, Nerves of Upper Lower ExtremitiesDocument93 pagesMuscles, Vessels, Nerves of Upper Lower Extremitiescansinunlu1559No ratings yet
- Anaphy ReportDocument28 pagesAnaphy ReportJunaisah P. PangaponNo ratings yet
- 6 Muscles of Forearm FinDocument46 pages6 Muscles of Forearm FinAbdelrhman AbubakrNo ratings yet
- Anatomy (302) - 1Document82 pagesAnatomy (302) - 1Shehzad Noman SajidNo ratings yet
- Anterior ArmDocument6 pagesAnterior ArmandrahlynNo ratings yet
- SGD 8Document3 pagesSGD 8Steph SantosNo ratings yet
- Anatomy Ofthe Upper ArmDocument37 pagesAnatomy Ofthe Upper ArmBenjamin JonathanNo ratings yet
- Anatomy of Hand-2Document24 pagesAnatomy of Hand-2Junaid AhmadNo ratings yet
- Nerves Nerve of Lower LimbDocument33 pagesNerves Nerve of Lower LimbSalsabeel SalamahNo ratings yet
- Lumbo - Sacral PlexusDocument41 pagesLumbo - Sacral Plexushariniselvam95drNo ratings yet
- Anatomy of The ForearmDocument2 pagesAnatomy of The ForearmAmal LadNo ratings yet
- 210420PM PPT - Femoral NerveDocument23 pages210420PM PPT - Femoral NerveAananda Raaj V MNo ratings yet
- Muscles of HandDocument15 pagesMuscles of HandAhmed TarekNo ratings yet
- LG 8Document56 pagesLG 8Joo Se HyukNo ratings yet
- Musculosk UL6 Muscles 4Document45 pagesMusculosk UL6 Muscles 4Zaid HamdanNo ratings yet
- RadialnervepresentationDocument22 pagesRadialnervepresentationmelburnveronNo ratings yet
- Elbow and Antebrachium NotesDocument8 pagesElbow and Antebrachium NoteschadNo ratings yet
- Muscles in The Posterior Compartment of The ThighDocument11 pagesMuscles in The Posterior Compartment of The Thighnandasheeras08No ratings yet
- Gross Anatomy of The Forearm: A CAL Package Designed By-Pratik SinhaDocument24 pagesGross Anatomy of The Forearm: A CAL Package Designed By-Pratik SinhaManvi JogiNo ratings yet
- A Simple Guide to the Voice Box and Its Disorders, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to the Voice Box and Its Disorders, Diagnosis, Treatment and Related ConditionsNo ratings yet
- The HeartDocument56 pagesThe HeartAuza Moses Ibrahim100% (1)
- 8 MediastinumDocument30 pages8 MediastinumAuza Moses Ibrahim100% (2)
- 9 PericardiumDocument19 pages9 PericardiumAuza Moses Ibrahim100% (2)
- Birth DefectsDocument46 pagesBirth DefectsAuza Moses IbrahimNo ratings yet
- Development of CNS and Spinal CordDocument41 pagesDevelopment of CNS and Spinal CordAuza Moses IbrahimNo ratings yet
- Integumentary SystemDocument51 pagesIntegumentary SystemAuza Moses IbrahimNo ratings yet
- Organogenetic PeriodDocument32 pagesOrganogenetic PeriodAuza Moses IbrahimNo ratings yet
- Development of The EarDocument58 pagesDevelopment of The EarAuza Moses IbrahimNo ratings yet
- GASTRULATIONDocument78 pagesGASTRULATIONAuza Moses IbrahimNo ratings yet
- Intro Head and NeckDocument74 pagesIntro Head and NeckAuza Moses Ibrahim100% (2)
- CerebrumDocument38 pagesCerebrumAuza Moses IbrahimNo ratings yet
- Anterior Compartment of The ArmDocument46 pagesAnterior Compartment of The ArmAuza Moses IbrahimNo ratings yet
- Anterior Compartment of The ForearmDocument55 pagesAnterior Compartment of The ForearmAuza Moses IbrahimNo ratings yet
- Axilla and Brachial PlexusDocument67 pagesAxilla and Brachial PlexusAuza Moses IbrahimNo ratings yet
- Anatomy of The Shoulder JointDocument44 pagesAnatomy of The Shoulder JointAuza Moses Ibrahim100% (1)
- Bednar MS, James MA, Light TR. Congenital Longitudinal Deficiency. J Hand Surg Am. 2009Document9 pagesBednar MS, James MA, Light TR. Congenital Longitudinal Deficiency. J Hand Surg Am. 2009AsdfNo ratings yet
- Carpal Instability - 2Document71 pagesCarpal Instability - 2mohammad farhanNo ratings yet
- Neill - A To Z of Bones JT & LigamentDocument272 pagesNeill - A To Z of Bones JT & LigamentPaul Vk100% (1)
- Outcomesof Tendon Transferto Restore Wrist Fingersand Thumb ExtensionDocument7 pagesOutcomesof Tendon Transferto Restore Wrist Fingersand Thumb ExtensionBecky YuliagustinaNo ratings yet
- Anat 51 To 92qDocument48 pagesAnat 51 To 92qMuhieddin GhosnNo ratings yet
- FixinDocument44 pagesFixinJaime EscobarNo ratings yet
- Anatomy 1 - MSS (Upper Limb)Document127 pagesAnatomy 1 - MSS (Upper Limb)Abdullah As'adNo ratings yet
- Resume Miologi Kaki Depan BlakangDocument1 pageResume Miologi Kaki Depan BlakangMade BagiNo ratings yet
- Ulnar Nerve Entrapment Massage Mag Whitney LoweDocument3 pagesUlnar Nerve Entrapment Massage Mag Whitney Lowewolfgangl70No ratings yet
- Plexopathy and MononeuropathyDocument38 pagesPlexopathy and MononeuropathySOUMYADEEP BHUINYANo ratings yet
- Acumed Surgical Technique Modular Hand System HNW00 04 A PDFDocument28 pagesAcumed Surgical Technique Modular Hand System HNW00 04 A PDFBey TaNo ratings yet
- Linear Algebra and Its Applications 5th Edition Lay Test BankDocument26 pagesLinear Algebra and Its Applications 5th Edition Lay Test BankJonathanSwansonbwyi100% (52)
- 1-Muscle of Upper Extremeties-TableDocument4 pages1-Muscle of Upper Extremeties-TableJan JeminoNo ratings yet
- Anatomy of The Hand: Khalid AyoubDocument53 pagesAnatomy of The Hand: Khalid Ayoubvaikunthan100% (2)
- Frog MusclesDocument1 pageFrog MusclesFama VicencioNo ratings yet
- Looking Again at The Forelimb of Tyrannosaurus Rex: Christine Lipkin and Kenneth CarpenterDocument25 pagesLooking Again at The Forelimb of Tyrannosaurus Rex: Christine Lipkin and Kenneth CarpenternomadNo ratings yet
- OinaDocument19 pagesOinaPauline JaleaNo ratings yet
- Wrist and Hand Complex BiomechanicsDocument94 pagesWrist and Hand Complex BiomechanicsManu kafeelNo ratings yet
- Soft Tissue Disorders and Fibromyalgia: Jaya Ravindran Consultant RheumatologistDocument54 pagesSoft Tissue Disorders and Fibromyalgia: Jaya Ravindran Consultant RheumatologistarunupadhayaNo ratings yet
- Female Muscle DiagramDocument1 pageFemale Muscle DiagrammakukikiNo ratings yet
- Distal Radial and Ulnar Arteries: The Alternative Forearm AccessDocument12 pagesDistal Radial and Ulnar Arteries: The Alternative Forearm AccessAlejandro Vazquez ManniseNo ratings yet
- Bio Mechanics of The ElbowDocument56 pagesBio Mechanics of The ElbowOnwaree Ing100% (4)
- ANATOMY Multiple Choice Questions 2012Document39 pagesANATOMY Multiple Choice Questions 2012kishorechandra100% (5)
- Nerve InjuriesDocument3 pagesNerve InjuriesAmber MerrittNo ratings yet
- Evolve Proline Operative TechniqueDocument20 pagesEvolve Proline Operative TechniqueRadomir CzajkaNo ratings yet
- Oina MusclesDocument73 pagesOina MusclesShen AndradeNo ratings yet
- Uts AnatomiDocument18 pagesUts AnatomiSuratmi UnnesNo ratings yet
- STT Tecnica QuirúrgicaDocument5 pagesSTT Tecnica QuirúrgicaNathaly GuevaraNo ratings yet
- Medical Picture Mnemonics PDFDocument28 pagesMedical Picture Mnemonics PDFAntoine JusticeNo ratings yet