
Health Assessment
Health Assessment
You might also like
- Gordon S Functional Health Pattern Assessment ToolDocument17 pagesGordon S Functional Health Pattern Assessment Toolmiss RN96% (45)
- Varicocele Secrets: The Underground Solution for Getting Rid of Varicocele for The Rest of Your Life [EN]From EverandVaricocele Secrets: The Underground Solution for Getting Rid of Varicocele for The Rest of Your Life [EN]No ratings yet
- Migrant Health FormDocument5 pagesMigrant Health FormImelda Junaedi100% (3)
- AdimeDocument4 pagesAdimeapi-294212644No ratings yet
- PFCMAtrix ToolkitDocument7 pagesPFCMAtrix ToolkitRold Brio Sos100% (3)
- Pathology I Practical Records PDFDocument73 pagesPathology I Practical Records PDFDeepinder Singh100% (1)
- Comprehensive Cardiovascular Medicine in The Primary Care Setting-Humana Press (2018) PDFDocument530 pagesComprehensive Cardiovascular Medicine in The Primary Care Setting-Humana Press (2018) PDFHaribabu ArumugamNo ratings yet
- Gordons Case Pres 1Document5 pagesGordons Case Pres 1JM Asentista0% (1)
- Gordons Interview Form (MCN)Document5 pagesGordons Interview Form (MCN)teuuuuNo ratings yet
- NURS 481L - Patient Profile DatabaseDocument7 pagesNURS 481L - Patient Profile DatabaseinnocentforeternityNo ratings yet
- ANTENATAL Assessment FINALDocument12 pagesANTENATAL Assessment FINALM. jehovah Nissie YeshalomeNo ratings yet
- Form "D" Report of Practical Experience: Nursing Clinical Practice IDocument29 pagesForm "D" Report of Practical Experience: Nursing Clinical Practice IAnderson RebaNo ratings yet
- Nursing/Nursing Forms/Gordon's 11 Functional Health Patterns Aoih0718Document14 pagesNursing/Nursing Forms/Gordon's 11 Functional Health Patterns Aoih0718jelaNo ratings yet
- Gordon S Functional Health Pattern Assessment TooL: EdisonDocument13 pagesGordon S Functional Health Pattern Assessment TooL: EdisonEdison Olad Dangkeo, RN,RM67% (3)
- Gordons Functional Health Pattern Assessment Tool (Bano, R.)Document3 pagesGordons Functional Health Pattern Assessment Tool (Bano, R.)ojay880% (1)
- Iii. Physical Assessment and Review of SystemDocument7 pagesIii. Physical Assessment and Review of SystemBiya MacunteNo ratings yet
- N.202-Introduction To Nursing Practice Health Assessment ToolDocument9 pagesN.202-Introduction To Nursing Practice Health Assessment ToolmNo ratings yet
- Clinical Pathway For Hypertensive Urgency (Revised)Document6 pagesClinical Pathway For Hypertensive Urgency (Revised)Heide Danica A. BaltazarNo ratings yet
- Assessment Tool On Neurological System: Baseline DataDocument21 pagesAssessment Tool On Neurological System: Baseline DataK HepsibaNo ratings yet
- Objective: Advanced Assessment (Gordon 11 Functional Assessment) H Ealth Perception-Health Management PatternDocument5 pagesObjective: Advanced Assessment (Gordon 11 Functional Assessment) H Ealth Perception-Health Management PatternAvery MarcelinoNo ratings yet
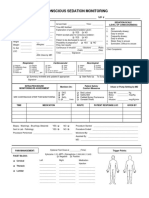
- 34 An Consious Sedation MonitoringDocument2 pages34 An Consious Sedation Monitoringabu alauon abed almohsenNo ratings yet
- Comprehensive Patient Assessment Form - 3 April 2017Document10 pagesComprehensive Patient Assessment Form - 3 April 2017sammichy1994No ratings yet
- Viral Haemorrhagic Fever - Case Investigation Form: Date of Detection of The Case Case IDDocument3 pagesViral Haemorrhagic Fever - Case Investigation Form: Date of Detection of The Case Case IDSalihu MustaphaNo ratings yet
- Activity Intolerance: NANDA Definition Discussion of The ProblemDocument42 pagesActivity Intolerance: NANDA Definition Discussion of The Problembeautifuljade_16No ratings yet
- GordonsDocument2 pagesGordonsAngelica OctotNo ratings yet
- Atrial FibrillationDocument28 pagesAtrial FibrillationKrisianne Mae Lorenzo FranciscoNo ratings yet
- Commed Template Family Report 2 1Document18 pagesCommed Template Family Report 2 1Ge NavNo ratings yet
- Obs ClerkingDocument3 pagesObs ClerkingEbrahim Adel Ali AhmedNo ratings yet
- Outbreaktoolkit Datacollectionform Lassafever enDocument2 pagesOutbreaktoolkit Datacollectionform Lassafever enAnton CamachoNo ratings yet
- NursereportDocument1 pageNursereportcodenurse95No ratings yet
- Heath Assessment ToolDocument8 pagesHeath Assessment ToolHouda Hayek100% (1)
- Ketikkan Emergency HostDocument2 pagesKetikkan Emergency HostBella ApNo ratings yet
- Gordon's FormDocument6 pagesGordon's FormHarry AglugobNo ratings yet
- Health Survey FormDocument3 pagesHealth Survey FormJazel SanchezNo ratings yet
- Health Appraisal Record I. PERSONAL DATA: Marbella, Marat B. Gender:MALE Age:16 II. Physical and Medical ExaminationDocument2 pagesHealth Appraisal Record I. PERSONAL DATA: Marbella, Marat B. Gender:MALE Age:16 II. Physical and Medical ExaminationMarat Marbella100% (1)
- MED-F-003 OPD Patient Assesment NurseDocument2 pagesMED-F-003 OPD Patient Assesment Nursedrakmalik71No ratings yet
- Health Appraisal Record: I. Personal Data: II. Physical and Medical ExaminationDocument2 pagesHealth Appraisal Record: I. Personal Data: II. Physical and Medical ExaminationJA BerzabalNo ratings yet
- Nursing Assessment Template 09Document3 pagesNursing Assessment Template 09jolibeecaldonaNo ratings yet
- Live @,upbringing, Schooling, Marriage: When:, S/O:, Home SituationsDocument5 pagesLive @,upbringing, Schooling, Marriage: When:, S/O:, Home SituationsJoy SalvadorNo ratings yet
- Case 4 - MCNP - Miguel, Mark Darren, T.Document3 pagesCase 4 - MCNP - Miguel, Mark Darren, T.markNo ratings yet
- Health Appraisal Record: I. Personal Data: II. Physical and Medical ExaminationDocument2 pagesHealth Appraisal Record: I. Personal Data: II. Physical and Medical ExaminationJA BerzabalNo ratings yet
- Physical Assessment ChecklistDocument3 pagesPhysical Assessment ChecklistIsang ButaNo ratings yet
- Comprehensive Nursing Assessment: Dengue Haemorrhagic Fever)Document4 pagesComprehensive Nursing Assessment: Dengue Haemorrhagic Fever)Devita PutriNo ratings yet
- Form "D" Report of Practical Experience: Nursing Clinical Practice IDocument24 pagesForm "D" Report of Practical Experience: Nursing Clinical Practice IMario Malvino Sengkey SengkeyNo ratings yet
- LRDR Forms PDFDocument17 pagesLRDR Forms PDFnursing filesNo ratings yet
- Clinic Name: A. Venous Health History FormDocument4 pagesClinic Name: A. Venous Health History Formnreddy10406862No ratings yet
- 7.8 Collect Data & Come Up With Plan For Day & Nursing Diagnosis Pre-Conference 8-9 Vitals Then Chart, AM Care, StartDocument2 pages7.8 Collect Data & Come Up With Plan For Day & Nursing Diagnosis Pre-Conference 8-9 Vitals Then Chart, AM Care, StartSade' CovingtonNo ratings yet
- Health Appraisal RecordDocument2 pagesHealth Appraisal RecordRandy PacquiaoNo ratings yet
- Gordon S Functional Health Pattern Assessment ToolDocument25 pagesGordon S Functional Health Pattern Assessment ToolMarc_Ulatan_3578No ratings yet
- Assessment FormDocument13 pagesAssessment FormKevin Bryan Manzano DyNo ratings yet
- Assessment Form: College of NursingDocument20 pagesAssessment Form: College of NursingSophia MayolNo ratings yet
- ANSAT CC - Nursing Assessment - Meeting The Care Needs of A Client-PatientDocument5 pagesANSAT CC - Nursing Assessment - Meeting The Care Needs of A Client-PatientjackydoodsonNo ratings yet
- Procedural Sedation RecordDocument2 pagesProcedural Sedation RecordRosanne AguilarNo ratings yet
- NURS 225V Principles III Data Collection ToolDocument2 pagesNURS 225V Principles III Data Collection ToolKrisNo ratings yet
- OB Patho Assessment Tool EditedDocument6 pagesOB Patho Assessment Tool EditedDarren RobertoNo ratings yet
- Clear & Simple Medical English in Dialogues: Vocabulary For ESL Health Care ProfessionalsFrom EverandClear & Simple Medical English in Dialogues: Vocabulary For ESL Health Care ProfessionalsNo ratings yet
- Heart of the Field "Refresher & Nha Certification Quick Notes"From EverandHeart of the Field "Refresher & Nha Certification Quick Notes"No ratings yet
- Joint Hypermobility Syndrome (Ehlers Danlos Syndrome)From EverandJoint Hypermobility Syndrome (Ehlers Danlos Syndrome)Rating: 1 out of 5 stars1/5 (1)
- 3 Weeks To A Better Back: Solutions for Healing the Structural, Nutritional, and Emotional Causes of Back PainFrom Everand3 Weeks To A Better Back: Solutions for Healing the Structural, Nutritional, and Emotional Causes of Back PainRating: 4 out of 5 stars4/5 (1)
- Spanish for Medical Professionals With Essential Questions and Responses Vol 3: A Cheat Sheet Of Medical Spanish Vocabulary, Phrases And Conversational Dialogues For Medical ProvidersFrom EverandSpanish for Medical Professionals With Essential Questions and Responses Vol 3: A Cheat Sheet Of Medical Spanish Vocabulary, Phrases And Conversational Dialogues For Medical ProvidersNo ratings yet
- Maxicare Prepaid-Health-Cards ProposalDocument10 pagesMaxicare Prepaid-Health-Cards ProposalTeddybear LiarsNo ratings yet
- CASP Checklist: Systematic ReviewDocument5 pagesCASP Checklist: Systematic ReviewWie SeptiaNiNo ratings yet
- Preparing Research Proposals in The Social and Behavioral Sciences: The Graduate Student Guide To FundingDocument38 pagesPreparing Research Proposals in The Social and Behavioral Sciences: The Graduate Student Guide To FundingTuân Hoàng ĐứcNo ratings yet
- Career Research EssayDocument2 pagesCareer Research Essayapi-600262102No ratings yet
- Newborn CareDocument30 pagesNewborn CareAlexandria P. OrcajadaNo ratings yet
- Managing Medicine SelectionDocument25 pagesManaging Medicine SelectionShoaib BiradarNo ratings yet
- Unit 4 Heath TopicDocument32 pagesUnit 4 Heath Topicralph allan bibatNo ratings yet
- Approach To Pediatric Periorbital EdemaDocument10 pagesApproach To Pediatric Periorbital EdemaismailtaaaNo ratings yet
- Inst Branchwise Mds 301022Document15 pagesInst Branchwise Mds 301022White WolfNo ratings yet
- 5440 15044 1 PBDocument10 pages5440 15044 1 PBDelfia Tanjung SariNo ratings yet
- English MultimodalDocument27 pagesEnglish Multimodalapi-240265090No ratings yet
- ILLINOIS - EE Health Policy Agreement PDFDocument2 pagesILLINOIS - EE Health Policy Agreement PDFKaren Cecilia RodriguezNo ratings yet
- Pascual, Paolo Enrino - LegCoun - 3A - Exercosim of Emily RoseDocument2 pagesPascual, Paolo Enrino - LegCoun - 3A - Exercosim of Emily RosePaolo Enrino PascualNo ratings yet
- North Maine POS SpecialistsDocument138 pagesNorth Maine POS SpecialistsMaine Trust For Local NewsNo ratings yet
- Anderson2008 Levofloxasin A ReviewDocument31 pagesAnderson2008 Levofloxasin A ReviewFazdrah AssyuaraNo ratings yet
- SITUATION 131 PagesDocument8 pagesSITUATION 131 PagesCharmaine Rose Inandan TriviñoNo ratings yet
- Potential Sources of Injury To The Care GiverDocument25 pagesPotential Sources of Injury To The Care Givernorhafizahstoh89No ratings yet
- Intellicare - Orientation DeckDocument54 pagesIntellicare - Orientation DeckLeinad Edino CruzNo ratings yet
- HyphemaDocument19 pagesHyphemaLiyanti RinceNo ratings yet
- IMNCIDocument31 pagesIMNCIJaya Prabha100% (2)
- Marie Antonette D.O. TanDocument159 pagesMarie Antonette D.O. TanJeffreydanceljr100% (5)
- Leprosy Control Program: Vision: Mission: ObjectivesDocument5 pagesLeprosy Control Program: Vision: Mission: ObjectivesAngelica VillalonNo ratings yet
- CPOT OriginalDocument9 pagesCPOT OriginalGaby ChocobarNo ratings yet
- Acute Abdominal PainDocument84 pagesAcute Abdominal PainFatimah AlshareefNo ratings yet
- Case Based DiscussionDocument22 pagesCase Based DiscussionAariNo ratings yet
- Anesthesia For Tracheal Surgery - Specific Procedures - UpToDateDocument29 pagesAnesthesia For Tracheal Surgery - Specific Procedures - UpToDateMaría Augusta Robayo UvilluzNo ratings yet

![Varicocele Secrets: The Underground Solution for Getting Rid of Varicocele for The Rest of Your Life [EN]](https://imgv2-1-f.scribdassets.com/img/word_document/544312715/149x198/dc87e19c66/1645158464?v=1)






















































































Download as docx, pdf, or txt
You might also like
- Gordon S Functional Health Pattern Assessment ToolDocument17 pagesGordon S Functional Health Pattern Assessment Toolmiss RN96% (45)
- Varicocele Secrets: The Underground Solution for Getting Rid of Varicocele for The Rest of Your Life [EN]From EverandVaricocele Secrets: The Underground Solution for Getting Rid of Varicocele for The Rest of Your Life [EN]No ratings yet
- Migrant Health FormDocument5 pagesMigrant Health FormImelda Junaedi100% (3)
- AdimeDocument4 pagesAdimeapi-294212644No ratings yet
- PFCMAtrix ToolkitDocument7 pagesPFCMAtrix ToolkitRold Brio Sos100% (3)
- Pathology I Practical Records PDFDocument73 pagesPathology I Practical Records PDFDeepinder Singh100% (1)
- Comprehensive Cardiovascular Medicine in The Primary Care Setting-Humana Press (2018) PDFDocument530 pagesComprehensive Cardiovascular Medicine in The Primary Care Setting-Humana Press (2018) PDFHaribabu ArumugamNo ratings yet
- Gordons Case Pres 1Document5 pagesGordons Case Pres 1JM Asentista0% (1)
- Gordons Interview Form (MCN)Document5 pagesGordons Interview Form (MCN)teuuuuNo ratings yet
- NURS 481L - Patient Profile DatabaseDocument7 pagesNURS 481L - Patient Profile DatabaseinnocentforeternityNo ratings yet
- ANTENATAL Assessment FINALDocument12 pagesANTENATAL Assessment FINALM. jehovah Nissie YeshalomeNo ratings yet
- Form "D" Report of Practical Experience: Nursing Clinical Practice IDocument29 pagesForm "D" Report of Practical Experience: Nursing Clinical Practice IAnderson RebaNo ratings yet
- Nursing/Nursing Forms/Gordon's 11 Functional Health Patterns Aoih0718Document14 pagesNursing/Nursing Forms/Gordon's 11 Functional Health Patterns Aoih0718jelaNo ratings yet
- Gordon S Functional Health Pattern Assessment TooL: EdisonDocument13 pagesGordon S Functional Health Pattern Assessment TooL: EdisonEdison Olad Dangkeo, RN,RM67% (3)
- Gordons Functional Health Pattern Assessment Tool (Bano, R.)Document3 pagesGordons Functional Health Pattern Assessment Tool (Bano, R.)ojay880% (1)
- Iii. Physical Assessment and Review of SystemDocument7 pagesIii. Physical Assessment and Review of SystemBiya MacunteNo ratings yet
- N.202-Introduction To Nursing Practice Health Assessment ToolDocument9 pagesN.202-Introduction To Nursing Practice Health Assessment ToolmNo ratings yet
- Clinical Pathway For Hypertensive Urgency (Revised)Document6 pagesClinical Pathway For Hypertensive Urgency (Revised)Heide Danica A. BaltazarNo ratings yet
- Assessment Tool On Neurological System: Baseline DataDocument21 pagesAssessment Tool On Neurological System: Baseline DataK HepsibaNo ratings yet
- Objective: Advanced Assessment (Gordon 11 Functional Assessment) H Ealth Perception-Health Management PatternDocument5 pagesObjective: Advanced Assessment (Gordon 11 Functional Assessment) H Ealth Perception-Health Management PatternAvery MarcelinoNo ratings yet
- 34 An Consious Sedation MonitoringDocument2 pages34 An Consious Sedation Monitoringabu alauon abed almohsenNo ratings yet
- Comprehensive Patient Assessment Form - 3 April 2017Document10 pagesComprehensive Patient Assessment Form - 3 April 2017sammichy1994No ratings yet
- Viral Haemorrhagic Fever - Case Investigation Form: Date of Detection of The Case Case IDDocument3 pagesViral Haemorrhagic Fever - Case Investigation Form: Date of Detection of The Case Case IDSalihu MustaphaNo ratings yet
- Activity Intolerance: NANDA Definition Discussion of The ProblemDocument42 pagesActivity Intolerance: NANDA Definition Discussion of The Problembeautifuljade_16No ratings yet
- GordonsDocument2 pagesGordonsAngelica OctotNo ratings yet
- Atrial FibrillationDocument28 pagesAtrial FibrillationKrisianne Mae Lorenzo FranciscoNo ratings yet
- Commed Template Family Report 2 1Document18 pagesCommed Template Family Report 2 1Ge NavNo ratings yet
- Obs ClerkingDocument3 pagesObs ClerkingEbrahim Adel Ali AhmedNo ratings yet
- Outbreaktoolkit Datacollectionform Lassafever enDocument2 pagesOutbreaktoolkit Datacollectionform Lassafever enAnton CamachoNo ratings yet
- NursereportDocument1 pageNursereportcodenurse95No ratings yet
- Heath Assessment ToolDocument8 pagesHeath Assessment ToolHouda Hayek100% (1)
- Ketikkan Emergency HostDocument2 pagesKetikkan Emergency HostBella ApNo ratings yet
- Gordon's FormDocument6 pagesGordon's FormHarry AglugobNo ratings yet
- Health Survey FormDocument3 pagesHealth Survey FormJazel SanchezNo ratings yet
- Health Appraisal Record I. PERSONAL DATA: Marbella, Marat B. Gender:MALE Age:16 II. Physical and Medical ExaminationDocument2 pagesHealth Appraisal Record I. PERSONAL DATA: Marbella, Marat B. Gender:MALE Age:16 II. Physical and Medical ExaminationMarat Marbella100% (1)
- MED-F-003 OPD Patient Assesment NurseDocument2 pagesMED-F-003 OPD Patient Assesment Nursedrakmalik71No ratings yet
- Health Appraisal Record: I. Personal Data: II. Physical and Medical ExaminationDocument2 pagesHealth Appraisal Record: I. Personal Data: II. Physical and Medical ExaminationJA BerzabalNo ratings yet
- Nursing Assessment Template 09Document3 pagesNursing Assessment Template 09jolibeecaldonaNo ratings yet
- Live @,upbringing, Schooling, Marriage: When:, S/O:, Home SituationsDocument5 pagesLive @,upbringing, Schooling, Marriage: When:, S/O:, Home SituationsJoy SalvadorNo ratings yet
- Case 4 - MCNP - Miguel, Mark Darren, T.Document3 pagesCase 4 - MCNP - Miguel, Mark Darren, T.markNo ratings yet
- Health Appraisal Record: I. Personal Data: II. Physical and Medical ExaminationDocument2 pagesHealth Appraisal Record: I. Personal Data: II. Physical and Medical ExaminationJA BerzabalNo ratings yet
- Physical Assessment ChecklistDocument3 pagesPhysical Assessment ChecklistIsang ButaNo ratings yet
- Comprehensive Nursing Assessment: Dengue Haemorrhagic Fever)Document4 pagesComprehensive Nursing Assessment: Dengue Haemorrhagic Fever)Devita PutriNo ratings yet
- Form "D" Report of Practical Experience: Nursing Clinical Practice IDocument24 pagesForm "D" Report of Practical Experience: Nursing Clinical Practice IMario Malvino Sengkey SengkeyNo ratings yet
- LRDR Forms PDFDocument17 pagesLRDR Forms PDFnursing filesNo ratings yet
- Clinic Name: A. Venous Health History FormDocument4 pagesClinic Name: A. Venous Health History Formnreddy10406862No ratings yet
- 7.8 Collect Data & Come Up With Plan For Day & Nursing Diagnosis Pre-Conference 8-9 Vitals Then Chart, AM Care, StartDocument2 pages7.8 Collect Data & Come Up With Plan For Day & Nursing Diagnosis Pre-Conference 8-9 Vitals Then Chart, AM Care, StartSade' CovingtonNo ratings yet
- Health Appraisal RecordDocument2 pagesHealth Appraisal RecordRandy PacquiaoNo ratings yet
- Gordon S Functional Health Pattern Assessment ToolDocument25 pagesGordon S Functional Health Pattern Assessment ToolMarc_Ulatan_3578No ratings yet
- Assessment FormDocument13 pagesAssessment FormKevin Bryan Manzano DyNo ratings yet
- Assessment Form: College of NursingDocument20 pagesAssessment Form: College of NursingSophia MayolNo ratings yet
- ANSAT CC - Nursing Assessment - Meeting The Care Needs of A Client-PatientDocument5 pagesANSAT CC - Nursing Assessment - Meeting The Care Needs of A Client-PatientjackydoodsonNo ratings yet
- Procedural Sedation RecordDocument2 pagesProcedural Sedation RecordRosanne AguilarNo ratings yet
- NURS 225V Principles III Data Collection ToolDocument2 pagesNURS 225V Principles III Data Collection ToolKrisNo ratings yet
- OB Patho Assessment Tool EditedDocument6 pagesOB Patho Assessment Tool EditedDarren RobertoNo ratings yet
- Clear & Simple Medical English in Dialogues: Vocabulary For ESL Health Care ProfessionalsFrom EverandClear & Simple Medical English in Dialogues: Vocabulary For ESL Health Care ProfessionalsNo ratings yet
- Heart of the Field "Refresher & Nha Certification Quick Notes"From EverandHeart of the Field "Refresher & Nha Certification Quick Notes"No ratings yet
- Joint Hypermobility Syndrome (Ehlers Danlos Syndrome)From EverandJoint Hypermobility Syndrome (Ehlers Danlos Syndrome)Rating: 1 out of 5 stars1/5 (1)
- 3 Weeks To A Better Back: Solutions for Healing the Structural, Nutritional, and Emotional Causes of Back PainFrom Everand3 Weeks To A Better Back: Solutions for Healing the Structural, Nutritional, and Emotional Causes of Back PainRating: 4 out of 5 stars4/5 (1)
- Spanish for Medical Professionals With Essential Questions and Responses Vol 3: A Cheat Sheet Of Medical Spanish Vocabulary, Phrases And Conversational Dialogues For Medical ProvidersFrom EverandSpanish for Medical Professionals With Essential Questions and Responses Vol 3: A Cheat Sheet Of Medical Spanish Vocabulary, Phrases And Conversational Dialogues For Medical ProvidersNo ratings yet
- Maxicare Prepaid-Health-Cards ProposalDocument10 pagesMaxicare Prepaid-Health-Cards ProposalTeddybear LiarsNo ratings yet
- CASP Checklist: Systematic ReviewDocument5 pagesCASP Checklist: Systematic ReviewWie SeptiaNiNo ratings yet
- Preparing Research Proposals in The Social and Behavioral Sciences: The Graduate Student Guide To FundingDocument38 pagesPreparing Research Proposals in The Social and Behavioral Sciences: The Graduate Student Guide To FundingTuân Hoàng ĐứcNo ratings yet
- Career Research EssayDocument2 pagesCareer Research Essayapi-600262102No ratings yet
- Newborn CareDocument30 pagesNewborn CareAlexandria P. OrcajadaNo ratings yet
- Managing Medicine SelectionDocument25 pagesManaging Medicine SelectionShoaib BiradarNo ratings yet
- Unit 4 Heath TopicDocument32 pagesUnit 4 Heath Topicralph allan bibatNo ratings yet
- Approach To Pediatric Periorbital EdemaDocument10 pagesApproach To Pediatric Periorbital EdemaismailtaaaNo ratings yet
- Inst Branchwise Mds 301022Document15 pagesInst Branchwise Mds 301022White WolfNo ratings yet
- 5440 15044 1 PBDocument10 pages5440 15044 1 PBDelfia Tanjung SariNo ratings yet
- English MultimodalDocument27 pagesEnglish Multimodalapi-240265090No ratings yet
- ILLINOIS - EE Health Policy Agreement PDFDocument2 pagesILLINOIS - EE Health Policy Agreement PDFKaren Cecilia RodriguezNo ratings yet
- Pascual, Paolo Enrino - LegCoun - 3A - Exercosim of Emily RoseDocument2 pagesPascual, Paolo Enrino - LegCoun - 3A - Exercosim of Emily RosePaolo Enrino PascualNo ratings yet
- North Maine POS SpecialistsDocument138 pagesNorth Maine POS SpecialistsMaine Trust For Local NewsNo ratings yet
- Anderson2008 Levofloxasin A ReviewDocument31 pagesAnderson2008 Levofloxasin A ReviewFazdrah AssyuaraNo ratings yet
- SITUATION 131 PagesDocument8 pagesSITUATION 131 PagesCharmaine Rose Inandan TriviñoNo ratings yet
- Potential Sources of Injury To The Care GiverDocument25 pagesPotential Sources of Injury To The Care Givernorhafizahstoh89No ratings yet
- Intellicare - Orientation DeckDocument54 pagesIntellicare - Orientation DeckLeinad Edino CruzNo ratings yet
- HyphemaDocument19 pagesHyphemaLiyanti RinceNo ratings yet
- IMNCIDocument31 pagesIMNCIJaya Prabha100% (2)
- Marie Antonette D.O. TanDocument159 pagesMarie Antonette D.O. TanJeffreydanceljr100% (5)
- Leprosy Control Program: Vision: Mission: ObjectivesDocument5 pagesLeprosy Control Program: Vision: Mission: ObjectivesAngelica VillalonNo ratings yet
- CPOT OriginalDocument9 pagesCPOT OriginalGaby ChocobarNo ratings yet
- Acute Abdominal PainDocument84 pagesAcute Abdominal PainFatimah AlshareefNo ratings yet
- Case Based DiscussionDocument22 pagesCase Based DiscussionAariNo ratings yet
- Anesthesia For Tracheal Surgery - Specific Procedures - UpToDateDocument29 pagesAnesthesia For Tracheal Surgery - Specific Procedures - UpToDateMaría Augusta Robayo UvilluzNo ratings yet