Download as pdf or txt
You might also like
- Participatory Approach For Safe Shelter Awareness (PASSA) ManualDocument134 pagesParticipatory Approach For Safe Shelter Awareness (PASSA) ManualInternational Federation of Red Cross Red Crescent Societies (IFRC)100% (2)
- Integration of Mirth Connect With OpenEMR2Document14 pagesIntegration of Mirth Connect With OpenEMR2Muhammad AliNo ratings yet
- Agriculture, Ecosystems and EnvironmentDocument14 pagesAgriculture, Ecosystems and Environmentsamuelpz1No ratings yet
- A Spatiodemographic Assessment of Solid Waste Handling Practises at Household Level in Bulawayo City, ZimbabweDocument23 pagesA Spatiodemographic Assessment of Solid Waste Handling Practises at Household Level in Bulawayo City, ZimbabweprosperNo ratings yet
- Nutritional Satus BrandsenDocument7 pagesNutritional Satus BrandsenTobias TijeraNo ratings yet
- Articledeconfrence ReprsentationssocialesDocument6 pagesArticledeconfrence ReprsentationssocialesLili MoralesNo ratings yet
- Food Security Through Sociocultural PerspectivesDocument10 pagesFood Security Through Sociocultural PerspectivesYounas KhanNo ratings yet
- Uamerica 22 .134446Document20 pagesUamerica 22 .134446Rimy Cruz GambaNo ratings yet
- Determinants of Rural Household Food Insecurity and Local Coping Strategies: The Case of Hoko District in Sidama Region, EthiopiaDocument8 pagesDeterminants of Rural Household Food Insecurity and Local Coping Strategies: The Case of Hoko District in Sidama Region, EthiopiaNovelty JournalsNo ratings yet
- Land Use Policy: SciencedirectDocument14 pagesLand Use Policy: SciencedirectJesus MierNo ratings yet
- Climate Change and Sustainable Practices: Telehealth As A Tool For Sharing Indigenous PracticesDocument8 pagesClimate Change and Sustainable Practices: Telehealth As A Tool For Sharing Indigenous PracticesIJAERS JOURNALNo ratings yet
- Studies On Variation of Some Metabolic Parameters in Rural and Urban PopulateDocument5 pagesStudies On Variation of Some Metabolic Parameters in Rural and Urban PopulateUzochukwu OnonujuNo ratings yet
- National Children's Science Congress: NCSC 2022 and 2023 Focal Theme and Sub-ThemesDocument11 pagesNational Children's Science Congress: NCSC 2022 and 2023 Focal Theme and Sub-ThemesnkhiangteNo ratings yet
- 24 Socio-Economic Profile and ExpenditureDocument7 pages24 Socio-Economic Profile and ExpenditureAbhishek VyasNo ratings yet
- Quality of Life (QoL) of Rural Dwellers in Nigeria: A Subjective Assessment of Residents of Ikeji-Arakeji, Osun-StateDocument7 pagesQuality of Life (QoL) of Rural Dwellers in Nigeria: A Subjective Assessment of Residents of Ikeji-Arakeji, Osun-StateSryahwa PublicationsNo ratings yet
- Case Study Community Problem and Solution AbilayDocument8 pagesCase Study Community Problem and Solution AbilayMark Laurence C. AbilayNo ratings yet
- Journal of Ecology - 2022 - M Ndez Vigo - Spatiotemporal Dynamics of Genetic Variation at The Quantitative and MolecularDocument16 pagesJournal of Ecology - 2022 - M Ndez Vigo - Spatiotemporal Dynamics of Genetic Variation at The Quantitative and MolecularRocío GRNo ratings yet
- Food SystemDocument14 pagesFood SystemM RefardianNo ratings yet
- 2023 - Graça, Roque Et Al. - How To Enable Sustainable Transitions in Schools - A Scoping ReviewDocument14 pages2023 - Graça, Roque Et Al. - How To Enable Sustainable Transitions in Schools - A Scoping ReviewiolandadiasmNo ratings yet
- Sustainability 13 03257 v2Document28 pagesSustainability 13 03257 v2GuillermoNo ratings yet
- Gaba and Bretagnolle - 2020Document11 pagesGaba and Bretagnolle - 2020Fritzner PIERRENo ratings yet
- Life-Cycle Energy Assessment and Carbon Footprint of Peri-Urban Horticulture. A Comparative Case Study of Local Food Systems in SpainDocument9 pagesLife-Cycle Energy Assessment and Carbon Footprint of Peri-Urban Horticulture. A Comparative Case Study of Local Food Systems in SpainFreddy Roberto Lema ChicaizaNo ratings yet
- Mediterranean Lifestyle Patterns Are AssDocument8 pagesMediterranean Lifestyle Patterns Are AssElton MatsushimaNo ratings yet
- 10 11648 J Ijpc 20210703 11Document8 pages10 11648 J Ijpc 20210703 11Abebaw AynewaNo ratings yet
- Research Protocol: A Synthesis of Qualitative Studies On The Process of Adaptation To Dependency in Elderly Persons and Their FamiliesDocument5 pagesResearch Protocol: A Synthesis of Qualitative Studies On The Process of Adaptation To Dependency in Elderly Persons and Their FamiliesAraNo ratings yet
- Assessement of Health ProblemsDocument9 pagesAssessement of Health Problemszerihundido72No ratings yet
- Dietary and Food Consumption Patterns and Their AsDocument16 pagesDietary and Food Consumption Patterns and Their AsToghrulNo ratings yet
- Mapping Food Systems: A Participatory Research Tool Tested in Kenya and BoliviaDocument11 pagesMapping Food Systems: A Participatory Research Tool Tested in Kenya and BoliviaYared Mesfin FikaduNo ratings yet
- Farming Systems Research Into The 21st Century: The New DynamicDocument30 pagesFarming Systems Research Into The 21st Century: The New DynamicVishnuvardhan RavichandranNo ratings yet
- Principles of Community Health NursingDocument37 pagesPrinciples of Community Health Nursingmaeliszxc kim100% (1)
- Focal and Sub ThemesDocument3 pagesFocal and Sub ThemesbirendrasinghrathiaNo ratings yet
- Her Land, Her Story: A Community-Run Digital Storytelling Project Exploring Climate-Gender-Health Relationships in Southern Senegal (1944 Words)Document6 pagesHer Land, Her Story: A Community-Run Digital Storytelling Project Exploring Climate-Gender-Health Relationships in Southern Senegal (1944 Words)MaddyAndersonNo ratings yet
- CabreraBarona Et Al. 2019 BMI Food Env. Activity SmokingDocument14 pagesCabreraBarona Et Al. 2019 BMI Food Env. Activity SmokingJuan Guillermo Cañón TorresNo ratings yet
- Boyé Et Al 2019Document18 pagesBoyé Et Al 2019chups oNo ratings yet
- 08 Handout in Participatory Community Health Program Managment 2Document41 pages08 Handout in Participatory Community Health Program Managment 2Bhargav MakwanaNo ratings yet
- MENDES, L. L. Et Al.. Individual and Environmental Factors Associated For Overweight in Urban Population of BrazilDocument7 pagesMENDES, L. L. Et Al.. Individual and Environmental Factors Associated For Overweight in Urban Population of Brazilalline.valleNo ratings yet
- Ipi 106950Document8 pagesIpi 106950darnia anitaNo ratings yet
- 1 s2.0 S0264837722002903 MainDocument10 pages1 s2.0 S0264837722002903 MainkacperNo ratings yet
- Role of Indigenous Knowledge Systems in The Conservation of The Bio-Physical Environment Among The Teso Community in Busia County-KenyaDocument9 pagesRole of Indigenous Knowledge Systems in The Conservation of The Bio-Physical Environment Among The Teso Community in Busia County-KenyaSamuel Richard NgodaNo ratings yet
- 2 Care FarmingDocument18 pages2 Care FarmingHyeonje ChoiNo ratings yet
- Cultural Practices and Health-Seeking Behaviours of The Mbororo Community in Mezam Division of North West CameroonDocument8 pagesCultural Practices and Health-Seeking Behaviours of The Mbororo Community in Mezam Division of North West CameroonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A More Diversified Diet May Be Also More AtherogenicDocument7 pagesA More Diversified Diet May Be Also More AtherogenicXochitl PonceNo ratings yet
- Community Function LandscapeDocument33 pagesCommunity Function LandscapePabitra NandyNo ratings yet
- Volenikova Oprsal 80 90Document11 pagesVolenikova Oprsal 80 90Chikondi TemboNo ratings yet
- Synopsis MardDocument31 pagesSynopsis MardPalak ChughNo ratings yet
- Literature Review On Agriculture and Sustainable DevelopmentDocument5 pagesLiterature Review On Agriculture and Sustainable DevelopmentaflstezqgNo ratings yet
- Hordyk 2015Document9 pagesHordyk 2015Francisca OyarzunNo ratings yet
- 1 Murillo-Pedrozo - Etal - 2021 - IntJEnvironResPublicHealthDocument13 pages1 Murillo-Pedrozo - Etal - 2021 - IntJEnvironResPublicHealthAlexis Buitrón ÁlvarezNo ratings yet
- ConceptOfCommunity&PhilHealthSituation Module CHN2 Jan2021Document18 pagesConceptOfCommunity&PhilHealthSituation Module CHN2 Jan2021Denise CastroNo ratings yet
- InternshipDocument13 pagesInternshipjudeuNo ratings yet
- Trophic Theory of Island BiogeographyDocument8 pagesTrophic Theory of Island BiogeographyAlejandro Guerrero LaverdeNo ratings yet
- Wang 2017Document10 pagesWang 2017Khairulina Mohd KamaruddinNo ratings yet
- Physiological Stress Does Not Increase With Urbanization in European Blackbirds - Evidence From Hormonal, Immunological and Cellular IndicatorsDocument9 pagesPhysiological Stress Does Not Increase With Urbanization in European Blackbirds - Evidence From Hormonal, Immunological and Cellular IndicatorsbuccaneerfosterNo ratings yet
- Docu 347Document7 pagesDocu 347Franco Cerna CuevaNo ratings yet
- B1996369-LI JING-Integrating Agro-Environmental Schemes Into Mainstream Agricultural PoliciesDocument89 pagesB1996369-LI JING-Integrating Agro-Environmental Schemes Into Mainstream Agricultural PoliciesArthur ZhouNo ratings yet
- 6-Are Determinants of Rural and Urban Food SecurityDocument21 pages6-Are Determinants of Rural and Urban Food SecuritylabaolcsgovNo ratings yet
- Resources, Conservation and RecyclingDocument8 pagesResources, Conservation and RecyclingAlexandra BobeșNo ratings yet
- Household Solid Waste Characterization by Family Socioeconomic Profile As Unit of AnalysisDocument8 pagesHousehold Solid Waste Characterization by Family Socioeconomic Profile As Unit of AnalysisRebeca García BennettNo ratings yet
- Periodontology 2000 - 2020 - Duran Pinedo - Metatranscriptomic Analyses of The Oral MicrobiomeDocument18 pagesPeriodontology 2000 - 2020 - Duran Pinedo - Metatranscriptomic Analyses of The Oral MicrobiomeAdil KaukabNo ratings yet
- Contributions of Sociometabolic Research To Sustainability ScienceDocument12 pagesContributions of Sociometabolic Research To Sustainability ScienceJaime AndradeNo ratings yet
- Sustainable Development - 2022 - Norde - Measuring Food Systems Sustainability in Heterogenous Countries The BrazilianDocument17 pagesSustainable Development - 2022 - Norde - Measuring Food Systems Sustainability in Heterogenous Countries The BrazilianratituNo ratings yet
- The Ecosystem Approach: Complexity, Uncertainty, and Managing for SustainabilityFrom EverandThe Ecosystem Approach: Complexity, Uncertainty, and Managing for SustainabilityNo ratings yet
- JA For Records User AccessDocument2 pagesJA For Records User Accesshabtamu hasenNo ratings yet
- Abyssinia Sample Collaction ManualDocument111 pagesAbyssinia Sample Collaction Manualhabtamu hasenNo ratings yet
- Master Register For All Doc FINAL July 29Document66 pagesMaster Register For All Doc FINAL July 29habtamu hasenNo ratings yet
- CH-3 Ja, JD& HRPDocument56 pagesCH-3 Ja, JD& HRPhabtamu hasenNo ratings yet
- CH-7 C&B Admin.Document38 pagesCH-7 C&B Admin.habtamu hasenNo ratings yet
- Ch-4 Recut and SelecDocument38 pagesCh-4 Recut and Selechabtamu hasenNo ratings yet
- Coping Strategies Vip EthiopiaDocument13 pagesCoping Strategies Vip Ethiopiahabtamu hasenNo ratings yet
- CH-6 PA and Job ChangeDocument31 pagesCH-6 PA and Job Changehabtamu hasenNo ratings yet
- Form 5 of DILG MC No. 2018-135 BPOC Monitoring Form 2 (DILG MC No. 2020-047) Ltia Form 3 (Dilg MC No. 2016-58)Document5 pagesForm 5 of DILG MC No. 2018-135 BPOC Monitoring Form 2 (DILG MC No. 2020-047) Ltia Form 3 (Dilg MC No. 2016-58)jacquelyn samson100% (1)
- CD 330+ Dimension DrawingDocument1 pageCD 330+ Dimension DrawingJOSUE FERNANDO FERNANDEZNo ratings yet
- Down SyndromeDocument12 pagesDown SyndromeUrbanus Matilu100% (1)
- The Risk of Skin Reactions Using Ecg Electrodes 0711Document3 pagesThe Risk of Skin Reactions Using Ecg Electrodes 0711Benjamin DoverNo ratings yet
- 11 - AASHTO Material Properties (2015)Document42 pages11 - AASHTO Material Properties (2015)mehdiNo ratings yet
- Yolk Gall EtcDocument5 pagesYolk Gall EtcNaveen BasudeNo ratings yet
- TCM Fd60-10Z8Document13 pagesTCM Fd60-10Z8Asif Ali50% (4)
- Micro Organisms Friend and FoeDocument11 pagesMicro Organisms Friend and FoeMir MurtazaNo ratings yet
- 12 - Umali Utilizing Onion (Allium Cepa L.) Peels Into Organic StrawDocument35 pages12 - Umali Utilizing Onion (Allium Cepa L.) Peels Into Organic Strawfaith tolentinoNo ratings yet
- Network Marketing Opportunity - Vestige Marketing Plan URTSAM - +919711572735Document16 pagesNetwork Marketing Opportunity - Vestige Marketing Plan URTSAM - +919711572735Samir K Mishra100% (1)
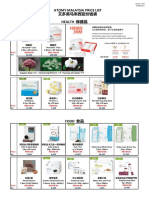
- Atomy Malaysia Price List 艾多美马来西亚价钱表 Health 保健品Document6 pagesAtomy Malaysia Price List 艾多美马来西亚价钱表 Health 保健品Lee Ling PengNo ratings yet
- Growing Temperate Fruit Trees in KenyaDocument138 pagesGrowing Temperate Fruit Trees in KenyanonimugoNo ratings yet
- Supply Chain Resilience and Healthcare Delivery in Disasters: A Structured ReviewDocument13 pagesSupply Chain Resilience and Healthcare Delivery in Disasters: A Structured ReviewShahnewaj SharanNo ratings yet
- Weldability Test For Thin Sheet MaterialsDocument6 pagesWeldability Test For Thin Sheet MaterialsAnonymous FHkX0ANo ratings yet
- TROLEX TX6114 Installation Operating DataDocument7 pagesTROLEX TX6114 Installation Operating DataprafulNo ratings yet
- Omoung LassiDocument3 pagesOmoung LassiWaqas MehmoodNo ratings yet
- Hydraulics NotesDocument193 pagesHydraulics NotesKunal KabraNo ratings yet
- Subanen HistoryDocument14 pagesSubanen HistoryAllan Mangangot100% (1)
- Home DistillerDocument18 pagesHome Distillerashoeman100% (1)
- Importance of Orthosis For Burn and Soft TissueDocument53 pagesImportance of Orthosis For Burn and Soft Tissuehashmilaiba847No ratings yet
- Exam Questions: Exam Title: Chapter MEK 8Document4 pagesExam Questions: Exam Title: Chapter MEK 8vishnu sharmaNo ratings yet
- Odisha Joint Entrance Examination (Ojee) - 2023Document1 pageOdisha Joint Entrance Examination (Ojee) - 2023Mango loveNo ratings yet
- All The Damn Vampires - Stacey Lawless PDFDocument13 pagesAll The Damn Vampires - Stacey Lawless PDFMark DingleNo ratings yet
- Request For Due Process - 04.24.2024Document12 pagesRequest For Due Process - 04.24.2024ABC Action NewsNo ratings yet
- Revised Cambridge Reference SequenceDocument6 pagesRevised Cambridge Reference SequenceRiemha Tiquie PurpleNo ratings yet
- EURO III System Dignostic ManualDocument131 pagesEURO III System Dignostic ManualsergeyNo ratings yet
- Westinghouse Oven ManualDocument21 pagesWestinghouse Oven ManualKeith BourdonNo ratings yet
- Skipping Breakfast Introduction 1 2Document38 pagesSkipping Breakfast Introduction 1 2Adrian PanlicanNo ratings yet