Download as pdf or txt
You might also like
- Year Book2008Document790 pagesYear Book2008Patricia GomesNo ratings yet
- Talking Fashion: Pierre Cardin Interviewed by Jan KedvesDocument5 pagesTalking Fashion: Pierre Cardin Interviewed by Jan KedvesJanKedves100% (1)
- Global E-Business and CollaborationDocument36 pagesGlobal E-Business and CollaborationTouhid AnikNo ratings yet
- Solastalgia The Distress Caused by Environmental ChangeDocument4 pagesSolastalgia The Distress Caused by Environmental ChangeAgonist IndNo ratings yet
- Neuroanatomical Considerations of Isolated Hearing Loss in Thalamic HemorrhageDocument3 pagesNeuroanatomical Considerations of Isolated Hearing Loss in Thalamic HemorrhageBella Cynthia BettabestariNo ratings yet
- Clinical Features and Outcomes in Patients With Non-Acoustic Cerebellopontine Angle TumoursDocument4 pagesClinical Features and Outcomes in Patients With Non-Acoustic Cerebellopontine Angle TumoursRikizu HobbiesNo ratings yet
- Tumefactive Demyelinating Lesions: Nine Cases and A Review of The LiteratureDocument9 pagesTumefactive Demyelinating Lesions: Nine Cases and A Review of The LiteraturePS NeuroNo ratings yet
- Accuracy of Imaging Technologies in The DiagnosisDocument7 pagesAccuracy of Imaging Technologies in The DiagnosisAGGREY DUDUNo ratings yet
- 5 5 5 Pontine Atypical Neurocytoma Case Report 副本Document8 pages5 5 5 Pontine Atypical Neurocytoma Case Report 副本singhNo ratings yet
- Axonal Sensorimotor Neuropathy in Patients With B-ThalassemiaDocument5 pagesAxonal Sensorimotor Neuropathy in Patients With B-ThalassemiaDesty PurnamasariNo ratings yet
- Herpes Simplex PolyanglionitisDocument5 pagesHerpes Simplex PolyanglionitisReani ZulfaNo ratings yet
- Original Article: Study of Computed Tomography (CT) Scan Finding in Neurofibromatosis Type 2Document4 pagesOriginal Article: Study of Computed Tomography (CT) Scan Finding in Neurofibromatosis Type 2Lisa SariNo ratings yet
- Cancer Stem Cells: To The EditorDocument4 pagesCancer Stem Cells: To The Editormira ariantiNo ratings yet
- Original Research Paper: Schwannomatosis: A Case Report and Literature ReviewDocument4 pagesOriginal Research Paper: Schwannomatosis: A Case Report and Literature ReviewEarthjournal PublisherNo ratings yet
- 5 THDocument17 pages5 THMohamed MohammedNo ratings yet
- Neurocysticercosis - Mimics and ChameleonsDocument8 pagesNeurocysticercosis - Mimics and ChameleonsNidia EscobarNo ratings yet
- InvestigationsDocument28 pagesInvestigationsAndrei BulgariuNo ratings yet
- The Long Term Outcome After Resection Of.20 PDFDocument9 pagesThe Long Term Outcome After Resection Of.20 PDFDragos IftimieNo ratings yet
- Mus 27395Document9 pagesMus 27395Denis Jesus Salgado GutierrezNo ratings yet
- Idiopatic SyringomyeliaDocument9 pagesIdiopatic SyringomyeliaIrenaNo ratings yet
- Archneur - 47 1990Document3 pagesArchneur - 47 1990Dra Carolina Escalante Neurologa de AdultosNo ratings yet
- Incidental Complex Repetitive Discharges On Needle ElectromyographyDocument4 pagesIncidental Complex Repetitive Discharges On Needle Electromyographyfulgencio garciaNo ratings yet
- Atretic Encephalocele, Tip of The IcebergDocument6 pagesAtretic Encephalocele, Tip of The IcebergAhmed H. Ali ElbestaweyNo ratings yet
- Surgical Management of Occipital Neuralgia A Systematic Review of The LiteratureDocument10 pagesSurgical Management of Occipital Neuralgia A Systematic Review of The Literatureosobucox1967No ratings yet
- Displasia Cortical de TaylorDocument11 pagesDisplasia Cortical de TaylorOscar F. Ochoa RuizNo ratings yet
- Spontaneous Infectious Discitis in Adults: Park Ridge, IllinoisDocument5 pagesSpontaneous Infectious Discitis in Adults: Park Ridge, IllinoisKarina PortilloNo ratings yet
- NHL CT FindingDocument7 pagesNHL CT FindingDwi Utari PratiwiNo ratings yet
- Small Stroke Causing Severe VertigoDocument5 pagesSmall Stroke Causing Severe VertigoDeTe Gun Rap'er ConkK'exsNo ratings yet
- Proceedings of The 2014 Spring Meeting of The Society of British 2014Document40 pagesProceedings of The 2014 Spring Meeting of The Society of British 2014rabiatul adawiyahNo ratings yet
- The Heart in Neurofibromatosis Type 1: An Echocardiographic StudyDocument6 pagesThe Heart in Neurofibromatosis Type 1: An Echocardiographic Studygaleno1985No ratings yet
- Cidp ParaneoDocument8 pagesCidp ParaneoPablo MarinNo ratings yet
- Intracerebral and Subarachnoid Hemorrhage in Patients With CancerDocument8 pagesIntracerebral and Subarachnoid Hemorrhage in Patients With CancerMadeNo ratings yet
- Vestibular Neuritis Affects Both Superior and Inferior Vestibular NervesDocument10 pagesVestibular Neuritis Affects Both Superior and Inferior Vestibular NervesSabina BădilăNo ratings yet
- 3 Territory Sign AJNRDocument4 pages3 Territory Sign AJNRAbdul AzeezNo ratings yet
- Pathology Clinical Questions @theMBBSvinesDocument16 pagesPathology Clinical Questions @theMBBSvinesMonil ShahNo ratings yet
- Foci Signal (Pseudo Lesions) To The Frontal: of Mri Anterior HornsDocument7 pagesFoci Signal (Pseudo Lesions) To The Frontal: of Mri Anterior HornsNourhan AliNo ratings yet
- Potential Role of Stem Cells For Neuropathic Pain DisordersDocument5 pagesPotential Role of Stem Cells For Neuropathic Pain Disordersmatheus derocoNo ratings yet
- SwchwanomaDocument5 pagesSwchwanomahockteo77No ratings yet
- Computed Tomography in Patients Presenting With Lacunar SyndromesDocument6 pagesComputed Tomography in Patients Presenting With Lacunar SyndromesPangestu KelvinNo ratings yet
- Tabrizi An 2009Document4 pagesTabrizi An 2009Dung Tran HoangNo ratings yet
- Acu Accident LumbarDocument2 pagesAcu Accident Lumbarrswongym449No ratings yet
- Eagle Syndrome An Unusual Cause of Head and Neck PainDocument2 pagesEagle Syndrome An Unusual Cause of Head and Neck PainCecilia AnderssonNo ratings yet
- Q PathologyDocument6 pagesQ PathologyTengku Soraya PutriNo ratings yet
- Oral Session I Which Theory Do The Structural Brain Changes Support?Document2 pagesOral Session I Which Theory Do The Structural Brain Changes Support?antonioopNo ratings yet
- Clinicalsigns, Imagingfeatures, Neuropathology, Andoutcome Incatsanddogswithcentralnervoussystemcryptococcosis FromcaliforniaDocument12 pagesClinicalsigns, Imagingfeatures, Neuropathology, Andoutcome Incatsanddogswithcentralnervoussystemcryptococcosis FromcaliforniaMicheleBerselliNo ratings yet
- Stickler 2006Document3 pagesStickler 2006leidy-riverosNo ratings yet
- Spinal Epidural Cavernous Hemangiomas in The 2024 International Journal of SDocument3 pagesSpinal Epidural Cavernous Hemangiomas in The 2024 International Journal of SRonald QuezadaNo ratings yet
- Heterotopia PV GruposDocument12 pagesHeterotopia PV GruposJuan D. HoyosNo ratings yet
- Intracranial Cavernomatous Hemangiomas As A Cause of Childhood Temporal Lobe EpilepsyDocument2 pagesIntracranial Cavernomatous Hemangiomas As A Cause of Childhood Temporal Lobe EpilepsyPrateek Kumar PandaNo ratings yet
- Lee 2007Document6 pagesLee 2007mmartinezs2507No ratings yet
- Intracranial Aneurysms in Childhood - 27 - Year Sigle Institution ExperienceDocument10 pagesIntracranial Aneurysms in Childhood - 27 - Year Sigle Institution ExperienceRony EvangelistaNo ratings yet
- Colreavy 2000Document6 pagesColreavy 2000Yi-Hung SungNo ratings yet
- Noc110069 346 351Document6 pagesNoc110069 346 351Carlos AlvaradoNo ratings yet
- Conclusion: Long-Term Follow-Up ForDocument31 pagesConclusion: Long-Term Follow-Up ForHima HuNo ratings yet
- Jhua16000143 PDFDocument3 pagesJhua16000143 PDFsamiratumananNo ratings yet
- Intracranial Aneurysms in Childhood: 27-Year Single-Institution ExperienceDocument10 pagesIntracranial Aneurysms in Childhood: 27-Year Single-Institution Experiencezrated786No ratings yet
- Neuropatías Por AtrapamientoDocument11 pagesNeuropatías Por AtrapamientoRamsses Rubio SalasNo ratings yet
- Jugular Desaturation Head: and After InjuryDocument7 pagesJugular Desaturation Head: and After Injuryzurique32No ratings yet
- Chan Low Sensitivity of Physical Examination FindingsDocument5 pagesChan Low Sensitivity of Physical Examination FindingsxelinenieNo ratings yet
- Seizures in Adults With Bacterial MeningitisDocument9 pagesSeizures in Adults With Bacterial MeningitiselaNo ratings yet
- Enterovirus ImagingDocument7 pagesEnterovirus ImagingMomeneo NeoNo ratings yet
- Neuralgias of The Head: Occipital Neuralgia: ReviewDocument10 pagesNeuralgias of The Head: Occipital Neuralgia: ReviewLuthfia PrasetiaNo ratings yet
- 2017 - Morris Et Al-AnnotatedDocument7 pages2017 - Morris Et Al-AnnotatedCemal GürselNo ratings yet
- Trigeminal Nerve Pain: A Guide to Clinical ManagementFrom EverandTrigeminal Nerve Pain: A Guide to Clinical ManagementAlaa Abd-ElsayedNo ratings yet
- Rephrasing Exercises Second TermDocument6 pagesRephrasing Exercises Second TermLulu SancNo ratings yet
- CDHA Infection ControlDocument2 pagesCDHA Infection ControlAliaa El WakeelNo ratings yet
- Section 1 GeneralDocument2 pagesSection 1 GeneralRached DouahchuaNo ratings yet
- Spsa - Edad 616bDocument18 pagesSpsa - Edad 616bapi-132081358No ratings yet
- Dishonour of Cheques and Negotiable Instruments - Legalsutra - Law Students' Knowledge-Base - Law School Projects, Moot Court Memorials, Class and Case Notes and More!Document8 pagesDishonour of Cheques and Negotiable Instruments - Legalsutra - Law Students' Knowledge-Base - Law School Projects, Moot Court Memorials, Class and Case Notes and More!Himanshu Mene100% (1)
- Atorvastatin (LIPITOR)Document2 pagesAtorvastatin (LIPITOR)Kristine Young100% (1)
- CMRL.12.18 : Section A: New Business, Regulatory and Sales-Related RequirementsDocument2 pagesCMRL.12.18 : Section A: New Business, Regulatory and Sales-Related RequirementsJovelyn ArgeteNo ratings yet
- DeputationDocument8 pagesDeputationAnand MauryaNo ratings yet
- Resume of Mohammad Efrad Hossain Job DocumentDocument5 pagesResume of Mohammad Efrad Hossain Job DocumentMohammad MonirNo ratings yet
- SDO Navotas Project-Assist - MAPEH Grade-8..Document17 pagesSDO Navotas Project-Assist - MAPEH Grade-8..Vanessa AsyaoNo ratings yet
- 哈佛商业评论 (Harvard Business Review)Document7 pages哈佛商业评论 (Harvard Business Review)h68f9trq100% (1)
- Open-Source Software For Automated Rodent Behavioral AnalysisDocument12 pagesOpen-Source Software For Automated Rodent Behavioral AnalysisGonzalo OrtegaNo ratings yet
- GR 6 Voc Words 4th QTRDocument5 pagesGR 6 Voc Words 4th QTRAzlynn Courtney FernandezNo ratings yet
- City of Tampa Disparity Study Report 050206 - Vol - 1Document102 pagesCity of Tampa Disparity Study Report 050206 - Vol - 1AsanijNo ratings yet
- RahmaDocument3 pagesRahmaAyyub RamadanNo ratings yet
- Film - The GuardianDocument1 pageFilm - The GuardianfisoxenekNo ratings yet
- Corporate Tax - UAEDocument48 pagesCorporate Tax - UAEUmair BaigNo ratings yet
- Week 1 Lesson 2 Tongue TwistersDocument14 pagesWeek 1 Lesson 2 Tongue Twistersapi-246058425No ratings yet
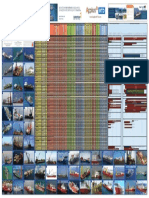
- Pipelay Capabilities WorldwideDocument1 pagePipelay Capabilities WorldwideJamesNo ratings yet
- Advanced Quality ManualDocument17 pagesAdvanced Quality ManualalexrferreiraNo ratings yet
- Six Examples of Large-Scale ProgramsDocument7 pagesSix Examples of Large-Scale ProgramsPhilcas LiNo ratings yet
- A Concept Paper About LoveDocument5 pagesA Concept Paper About LoveStephen Rivera100% (1)
- Oracle Switch ES1-24 Configuration GuideDocument88 pagesOracle Switch ES1-24 Configuration GuideNoe HernadezNo ratings yet
- Elegoo Saturn 8K LCD Light Curable 3D Printer User ManualDocument20 pagesElegoo Saturn 8K LCD Light Curable 3D Printer User ManualStanNo ratings yet
- Project Report Dam Level WarningDocument8 pagesProject Report Dam Level Warningpankaj_yadav007No ratings yet
- International Journal of Technical Innovation in Modern Engineering & Science (IJTIMES)Document3 pagesInternational Journal of Technical Innovation in Modern Engineering & Science (IJTIMES)Vikunj TilvaNo ratings yet