Download as pdf or txt
You might also like
- Pinata Unit Plan and Lessons PortfolioDocument7 pagesPinata Unit Plan and Lessons Portfolioapi-281759709No ratings yet
- 2022 05 06 - ZYG - Projekt Z - PanTum Detect Befund - Unauffällig - v4 (1) .De - enDocument2 pages2022 05 06 - ZYG - Projekt Z - PanTum Detect Befund - Unauffällig - v4 (1) .De - ennikola-avramov-8934No ratings yet
- Catalog: Set The Standard For Quality in Your Laboratory With CLSIDocument36 pagesCatalog: Set The Standard For Quality in Your Laboratory With CLSITrọng TínNo ratings yet
- dyassayENG NADP TBADocument2 pagesdyassayENG NADP TBAdewiNo ratings yet
- Martinez 2016Document4 pagesMartinez 2016Filipe JorgeNo ratings yet
- JR - Fingerstick Precision and Total ErrorDocument6 pagesJR - Fingerstick Precision and Total Errorpatologi klinikNo ratings yet
- CA-660 CA-650 4p ENDocument4 pagesCA-660 CA-650 4p ENanisaaanrNo ratings yet
- DownloadDocument12 pagesDownloadrelax soundNo ratings yet
- RandoxDocument32 pagesRandoxIta MaghfirahNo ratings yet
- Tchol H Met CobasDocument22 pagesTchol H Met CobasGhaith MaaniNo ratings yet
- Percepatan Deteksi Awal Covid-19 Dengan Artificial Intelligent (AI) Bidang Radiologi PERSI - 01 Agustus 2020Document14 pagesPercepatan Deteksi Awal Covid-19 Dengan Artificial Intelligent (AI) Bidang Radiologi PERSI - 01 Agustus 2020Enggay OmdoNo ratings yet
- Quality Control BrochureDocument40 pagesQuality Control BrochureRajeev PareekNo ratings yet
- Fat CATSTransfus Med 17Document9 pagesFat CATSTransfus Med 17Jamel GrineNo ratings yet
- BIOPRO J MET Uric Acid 508Document15 pagesBIOPRO J MET Uric Acid 508musembijosef2011No ratings yet
- C-Peptide: Diagnostic Automation, IncDocument6 pagesC-Peptide: Diagnostic Automation, IncmusiboyinaNo ratings yet
- DCA Vantage BrochureDocument2 pagesDCA Vantage BrochureaadasdsdsaNo ratings yet
- English CatalogDocument29 pagesEnglish CatalogMarcos RojasNo ratings yet
- S1665579616300515 PDFDocument6 pagesS1665579616300515 PDFService EngineerNo ratings yet
- Application Note LHS EN 0219Document2 pagesApplication Note LHS EN 0219JorgeNo ratings yet
- LC MS MS Became Routine in Clinical DiagnosticsDocument10 pagesLC MS MS Became Routine in Clinical DiagnosticsJorge TriforceNo ratings yet
- LT726 Specific Proteins 1Document40 pagesLT726 Specific Proteins 1Youssef SalehNo ratings yet
- Medi Test Urine Analysis ENDocument12 pagesMedi Test Urine Analysis ENCandy ManNo ratings yet
- Rwanda Pricelist-11-11-2016Document85 pagesRwanda Pricelist-11-11-2016BISHWEKA CherifNo ratings yet
- Biopro J Met Phosphorus 508Document15 pagesBiopro J Met Phosphorus 508Elizabeth FridayNo ratings yet
- Be 31 e 8Document32 pagesBe 31 e 8bananita86No ratings yet
- Urinary Organic Acids DR BralleyDocument5 pagesUrinary Organic Acids DR BralleyMetametrixNo ratings yet
- 5991-0350EN Water Brochure - 1Document4 pages5991-0350EN Water Brochure - 1Fahmi HamdaniNo ratings yet
- Efectos A La Exp Al Vino TintoDocument11 pagesEfectos A La Exp Al Vino TintoAdriana CoronadoNo ratings yet
- BD FACSCount BrochureDocument12 pagesBD FACSCount BrochureAhmed Ghassany100% (1)
- Monobind Assay Technical GuideDocument16 pagesMonobind Assay Technical GuideDaNny XaVierNo ratings yet
- INdiki Catálogo de PruebasDocument12 pagesINdiki Catálogo de PruebasrobertochaviraqfbNo ratings yet
- Framework of National Cancer Control Program in IndonesiaDocument20 pagesFramework of National Cancer Control Program in IndonesiaIndonesian Journal of Cancer100% (3)
- Pereira 2018Document6 pagesPereira 2018UnknownNo ratings yet
- Diagnostic Instrument Booklet ABX 00258Document44 pagesDiagnostic Instrument Booklet ABX 00258Moisés RodríguezNo ratings yet
- C.perfringens MF WaterDocument32 pagesC.perfringens MF WaterAgeng Wahyu PatrianitaNo ratings yet
- T-Level BookletDocument20 pagesT-Level BookletNowsathAliNo ratings yet
- Icsi652 PDFDocument80 pagesIcsi652 PDFClaire FineNo ratings yet
- CT2201-Diasino ControlSetDocument1 pageCT2201-Diasino ControlSethuripNo ratings yet
- Mutistix 10 SG With Clinitek Status Plus In-Service TrainingDocument44 pagesMutistix 10 SG With Clinitek Status Plus In-Service TrainingMyriam HernandezNo ratings yet
- EN - BioMajesty 6010 - CDocument2 pagesEN - BioMajesty 6010 - CmnemonicsNo ratings yet
- 2015E Updated GuidelinesDocument1,269 pages2015E Updated GuidelinesYipno Wanhar El MawardiNo ratings yet
- NCCN Head-And-neck 2020 Glándulas SalivaresDocument9 pagesNCCN Head-And-neck 2020 Glándulas Salivaresd.ayala1006No ratings yet
- sp1 CariesDocument2 pagessp1 CariesDaniela Herrera ConsumiNo ratings yet
- 2013-05-Sp Advances in Pharmaceutical AnalysisDocument36 pages2013-05-Sp Advances in Pharmaceutical AnalysismercedesNo ratings yet
- Reach Applicability CompassDocument9 pagesReach Applicability CompassMiguel GonzalezNo ratings yet
- A1791211477809240629 RLSDocument3 pagesA1791211477809240629 RLSShilpa NarkhedeNo ratings yet
- Catalog Ode Medi TecDocument13 pagesCatalog Ode Medi TecmotellawiNo ratings yet
- Phosphorus MDDocument1 pagePhosphorus MDPhong Nguyễn WindyNo ratings yet
- 2019 Web Catalog 2019.2.18Document192 pages2019 Web Catalog 2019.2.18David MuñozNo ratings yet
- PreciControl Lung Cancer - Ms - 07360070190.v2.en PDFDocument2 pagesPreciControl Lung Cancer - Ms - 07360070190.v2.en PDFARIF AHAMMED P100% (1)
- Drew DS360 BrochureDocument2 pagesDrew DS360 BrochureOo Kenx OoNo ratings yet
- 5991-0350EN Water BrochureDocument28 pages5991-0350EN Water Brochurepeeping.dogNo ratings yet
- Hands-On Experience: Accreditation of Pathology Laboratories According To ISO 15189 Alexandar Tzankova Luigi TornilloaDocument9 pagesHands-On Experience: Accreditation of Pathology Laboratories According To ISO 15189 Alexandar Tzankova Luigi TornilloaofusandeepNo ratings yet
- Kamecke Et Al 2017 Accuracy Assessment of An Improved Version of An Established Blood Glucose Monitoring System ForDocument3 pagesKamecke Et Al 2017 Accuracy Assessment of An Improved Version of An Established Blood Glucose Monitoring System ForRafat ElshemiNo ratings yet
- ACROBiosystems Product CatalogueDocument40 pagesACROBiosystems Product CatalogueArunee HansawongsakulNo ratings yet
- Vivid T9 BrochureDocument16 pagesVivid T9 Brochurebashir019No ratings yet
- PI e TC - HBA1C 33544 - 33547 2312 9Document1 pagePI e TC - HBA1C 33544 - 33547 2312 9Osama Ben DawNo ratings yet
- Trigly K Met 508Document19 pagesTrigly K Met 508Anachronistic girlNo ratings yet
- Particles and Nanoparticles in Pharmaceutical Products: Design, Manufacturing, Behavior and PerformanceFrom EverandParticles and Nanoparticles in Pharmaceutical Products: Design, Manufacturing, Behavior and PerformanceNo ratings yet
- PET-CT for the Management of Cancer Patients: A Review of the Existing EvidenceFrom EverandPET-CT for the Management of Cancer Patients: A Review of the Existing EvidenceNo ratings yet
- UviqoqDocument2 pagesUviqoqdewiNo ratings yet
- EEA002Document6 pagesEEA002dewiNo ratings yet
- PI e TBA - 21 3Document3 pagesPI e TBA - 21 3dewiNo ratings yet
- dyassayENG NADP TBADocument2 pagesdyassayENG NADP TBAdewiNo ratings yet
- Olympus AU400 ReagentsDocument2 pagesOlympus AU400 ReagentsdewiNo ratings yet
- Ingole Et Al 2013 cd4 Counts in Laboratory Monitoring of Hiv Disease Experience From Western IndiaDocument4 pagesIngole Et Al 2013 cd4 Counts in Laboratory Monitoring of Hiv Disease Experience From Western IndiadewiNo ratings yet
- Front MatterDocument1 pageFront MatterdewiNo ratings yet
- FM TadkaDocument2 pagesFM TadkarohitsahitaNo ratings yet
- Bacillus Subtilis Strains Isolated From Different Habitats: Amicoumacin Antibiotic Production and Genetic Diversity ofDocument7 pagesBacillus Subtilis Strains Isolated From Different Habitats: Amicoumacin Antibiotic Production and Genetic Diversity ofwisorNo ratings yet
- InsuranceDocument9 pagesInsurancePrashant MeenaNo ratings yet
- Ingles V e VIDocument314 pagesIngles V e VIAntonio MacaiaNo ratings yet
- Module. Major Foundations and Philosophies of CurriculumDocument7 pagesModule. Major Foundations and Philosophies of CurriculumJohn Dave MabántaNo ratings yet
- Why We Need The Individual MandateDocument3 pagesWhy We Need The Individual MandateCenter for American ProgressNo ratings yet
- Group 1 - OfW RemittancesDocument22 pagesGroup 1 - OfW RemittancesFLORENCE MAY SUMINDOLNo ratings yet
- 14740x 2016 Syllabus and Reading ListDocument11 pages14740x 2016 Syllabus and Reading ListFaysal HaqueNo ratings yet
- WACOM 2017 Org ChartDocument21 pagesWACOM 2017 Org ChartLeonorin FchNo ratings yet
- Bussey y Bandura (1992)Document16 pagesBussey y Bandura (1992)Lorena AyusoNo ratings yet
- Pa CourseworkDocument5 pagesPa Courseworkafjwoamzdxwmct100% (2)
- Verb Patterns - SlidesDocument13 pagesVerb Patterns - Slideskenya ortegaNo ratings yet
- History and Political Science: Solution: Practice Activity Sheet 3Document9 pagesHistory and Political Science: Solution: Practice Activity Sheet 3Faiz KhanNo ratings yet
- Continuous Probability DistributionDocument22 pagesContinuous Probability DistributionMusa AmanNo ratings yet
- How An Average Nigerian Can Cast Powerful Spells For Love, Money, Protection and Spiritual Power.Document22 pagesHow An Average Nigerian Can Cast Powerful Spells For Love, Money, Protection and Spiritual Power.Keysopedia WiredNo ratings yet
- Verified Component List Aama Certification Program: Part One Components of Certified Windows and DoorsDocument14 pagesVerified Component List Aama Certification Program: Part One Components of Certified Windows and Doorsjuan rodriguezNo ratings yet
- Learner's Development Assessment HRGDocument5 pagesLearner's Development Assessment HRGChiela BagnesNo ratings yet
- 4 January Personality - Google Search PDFDocument1 page4 January Personality - Google Search PDFNxxr Xleyxh chanelNo ratings yet
- Doctrine of RepugnancyDocument13 pagesDoctrine of RepugnancyAmita SinwarNo ratings yet
- Richard-2019-9-29 - (PO 1048) PDFDocument1 pageRichard-2019-9-29 - (PO 1048) PDFLeslie Ali TapodocNo ratings yet
- Inglês 11 Classe (Textos Editores) PDFDocument180 pagesInglês 11 Classe (Textos Editores) PDFNota Joao Tembo50% (2)
- Project Report (Aniket18GSOB1010055, Sakshi18GSOB1010164, Rupali18GSOB1010192)Document25 pagesProject Report (Aniket18GSOB1010055, Sakshi18GSOB1010164, Rupali18GSOB1010192)vidhya vijayanNo ratings yet
- 2nd Person StoryDocument1 page2nd Person Storynya.cooktillettNo ratings yet
- Pelman V McDonalds SDNYDocument65 pagesPelman V McDonalds SDNYfoodfightNo ratings yet
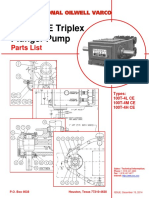
- 100T Pump Parts List PDFDocument30 pages100T Pump Parts List PDFGabriel Andres ValenciaNo ratings yet
- Afante Louie Anne E. Budgeting ProblemsDocument4 pagesAfante Louie Anne E. Budgeting ProblemsKyla Kim AriasNo ratings yet
- Solucion Error Cargue Mediante OPENROWSEDocument4 pagesSolucion Error Cargue Mediante OPENROWSEJEBUSOOONo ratings yet
- Word Form Exercises With KeyDocument5 pagesWord Form Exercises With KeyLoveu GoNo ratings yet
- Inward Reinsurance 14.05.2014Document14 pagesInward Reinsurance 14.05.2014Christian Njitche100% (1)