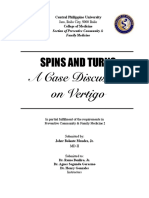
Utilising case history to diagnose Oesophageal Dysphagia
DYSPHAGIA
OROPHARYNGEAL DYSPHAGIA: OESOPHAGEAL DYSPHAGIA:
Reported level of dysphagia is HIGH Reported level of dysphagia may be
May be for liquids or solids HIGH, MID or LOW
Aspiration symptoms are usually immediate if present Aspiration symptoms are delayed if
Regurgitation is usually immediate if present present
Onset may be sudden or progressive Symptoms present for solids > liquids
Voice change may be present Regurgitation is delayed if present
Neurological history may be present Onset is usually slowly progressive
Voice change not necessarily present
Neurological history not necessarily
present
NOTE:
Overlap may occur
STRUCTURAL: Eg. Late stage FUNCTIONAL:
(eg. Stenosis, narrowing 2o stricture achalasia, (eg. Motility disorder)
or tumour) severe reflux & Slowly progressive in nature
Progressive in nature scleroderma Dysphagia for solids and liquids
Dysphagia for solids > liquids Pain / discomfort often a feature
Bolus obstruction may occur Aspiration is a feature of achalasia
Aspiration is a late feature &
infrequent
EXCEPTION:
Tracheo-
esophageal fistula
BENIGN: MALIGNANT: ACHALASIA & DIFFUSE SPASM:
Stricture Primary – SCC or SCLERODERMA: Evident for solids
Ring / web adenocarcinoma Progressive for = liquids
Caustic injury Secondary – solids liquids Inconsistent
Extrinsic extrinsic Consistent presentation
compression compression ( eg. presentation Pain is a key
(cardiac vs Lung cancer) Discomfort is feature
mediastinal) Weight loss is key often a key Worse for cold
feature feature substances
Can be rapidly
progressive
Nicola CLAYTON – NSW Dysphagia Interest Group 2016
You might also like
- PLAB 1700 MCQs Dr. Khalid - S Explanation of 1700 MCQDocument680 pagesPLAB 1700 MCQs Dr. Khalid - S Explanation of 1700 MCQguzelnor100% (35)
- Gastroenterology and Hepatology Complete PDFDocument257 pagesGastroenterology and Hepatology Complete PDFCarolina Gómez Ruiz100% (2)
- Toacs by ShireenDocument244 pagesToacs by ShireenMuhammad Zeeshan100% (1)
- NCM 116 - Git (Module 5)Document15 pagesNCM 116 - Git (Module 5)Meryville Jacildo100% (1)
- 2012 The Patient History - Evidence Based Appoach-368-376 PDFDocument9 pages2012 The Patient History - Evidence Based Appoach-368-376 PDFJoseph AndradeNo ratings yet
- Dysphagia: - Dr. Arjun SainiDocument80 pagesDysphagia: - Dr. Arjun SainiArjun SainiNo ratings yet
- Parkinsonismo Atípico Clinic 2015Document18 pagesParkinsonismo Atípico Clinic 2015Kharen VerjelNo ratings yet
- CS IvDocument71 pagesCS IvjNo ratings yet
- GI Sympt Mokhtar (2015)Document85 pagesGI Sympt Mokhtar (2015)Abdelrahman MokhtarNo ratings yet
- Gastrointestinal System: Symptomatology of TheDocument85 pagesGastrointestinal System: Symptomatology of TheAbdelrahman MokhtarNo ratings yet
- Neurologic DisturbancesssDocument2 pagesNeurologic DisturbancesssSJane FeriaNo ratings yet
- The Nervous SystemDocument24 pagesThe Nervous SystemKiara GovenderNo ratings yet
- DizzinessDocument6 pagesDizzinessRebecca WongNo ratings yet
- Ent Guidelines New 020616Document15 pagesEnt Guidelines New 020616Osasere EwekaNo ratings yet
- CN 118 - Lecture ReviewerDocument40 pagesCN 118 - Lecture ReviewerCamille SanguyoNo ratings yet
- Parkinson Disease & Other Movement Disorders: Cherian Abraham Karunapuzha, M.DDocument40 pagesParkinson Disease & Other Movement Disorders: Cherian Abraham Karunapuzha, M.DsafiraNo ratings yet
- Progressive Supranuclear PalsyDocument23 pagesProgressive Supranuclear PalsyAdonai Jireh Dionne BaliteNo ratings yet
- Dysarthria ChartDocument12 pagesDysarthria ChartTalia Garcia100% (1)
- Assessment of Head and NeckDocument13 pagesAssessment of Head and NeckBaniwas Marie AgnesNo ratings yet
- Movement DisordersDocument39 pagesMovement Disorderstcj4bpj2pnNo ratings yet
- Effects of Cancer What Is CancerDocument4 pagesEffects of Cancer What Is CancerL Rean Carmelle MAGALLONESNo ratings yet
- Prof. Hasan Machfoed 2017-10-13 PEKANBARU VERTIGODocument26 pagesProf. Hasan Machfoed 2017-10-13 PEKANBARU VERTIGOPutri Deas HadilofyaniNo ratings yet
- Clase Cefalea 2016Document60 pagesClase Cefalea 2016Juliana AndradeNo ratings yet
- Parkinsons Disease Copy 3Document41 pagesParkinsons Disease Copy 3Raghad AbbadyNo ratings yet
- LECTURE 3 - NONEPILEPTIC Events (Held in 14.2.19)Document57 pagesLECTURE 3 - NONEPILEPTIC Events (Held in 14.2.19)CristinaGheorgheNo ratings yet
- Dizziness and Loss of Consciousness: Cardiovascular CausesDocument4 pagesDizziness and Loss of Consciousness: Cardiovascular CausesMohammedNo ratings yet
- Chapter 13 - Parkinson S Disease - 2014 - Clinical NeuroscienceDocument17 pagesChapter 13 - Parkinson S Disease - 2014 - Clinical NeuroscienceMarta Casals CollNo ratings yet
- MS Disease ManagementsDocument27 pagesMS Disease ManagementstabiNo ratings yet
- Bec Quick CardsDocument14 pagesBec Quick CardsUmidagha BaghirzadaNo ratings yet
- Epilepsy: Causes of Seizures (Non-Epileptic)Document5 pagesEpilepsy: Causes of Seizures (Non-Epileptic)humdingerNo ratings yet
- Paralysis in Dogs and CatsDocument56 pagesParalysis in Dogs and Catscat clinic pdhbNo ratings yet
- Hidrosefalus Bertekanan Normal: WeaknessDocument5 pagesHidrosefalus Bertekanan Normal: WeaknessfathinbalweelNo ratings yet
- Parkinson-Plus SyndromeDocument2 pagesParkinson-Plus SyndromeRuth May de VillaNo ratings yet
- Pages From PEM - 5 Minute Pediatric Emergency Medicine Consult-2Document2 pagesPages From PEM - 5 Minute Pediatric Emergency Medicine Consult-2Dmitri KaramazovNo ratings yet
- Unit 3Document18 pagesUnit 3marlou agananNo ratings yet
- Multiple SlerosisDocument3 pagesMultiple SlerosisTrishia GuillermoNo ratings yet
- Falls History Exam Investigation and Management - ProtectedDocument5 pagesFalls History Exam Investigation and Management - ProtectedKLNo ratings yet
- Cardio Respiratory Asessment For PhysiotDocument10 pagesCardio Respiratory Asessment For PhysiotJayden HiiNo ratings yet
- Constipation and PUDDocument2 pagesConstipation and PUDm3d1kNo ratings yet
- Parkinson'S Disease: by - Nikita Borade BPT Final YearDocument42 pagesParkinson'S Disease: by - Nikita Borade BPT Final YearNikks BoradeNo ratings yet
- Pediatric CardiologyDocument7 pagesPediatric CardiologyMaikka IlaganNo ratings yet
- Gi - PathophysiologyDocument96 pagesGi - Pathophysiologyjmosser100% (4)
- Stroke Rehabilitation (Bayu) - EditDocument34 pagesStroke Rehabilitation (Bayu) - EditFinny BoekorsjomNo ratings yet
- Seizure Disorder Types: Partial - Local Onset May or May Not Impair Consciousness SimpleDocument4 pagesSeizure Disorder Types: Partial - Local Onset May or May Not Impair Consciousness Simpleampogison08No ratings yet
- Management of PX With Neurologic DysfunctionDocument12 pagesManagement of PX With Neurologic Dysfunctiongabrielle magdaraogNo ratings yet
- Examination and Superficial Palpation of The AbdomenDocument38 pagesExamination and Superficial Palpation of The AbdomenРопннпгпNo ratings yet
- WEEK 15 Pediatric Neuro and Muskuloskeletal DisordersDocument91 pagesWEEK 15 Pediatric Neuro and Muskuloskeletal Disordersrising starNo ratings yet
- Abruptio Placentae: (Accidental Hemorrhage, Premature Separation of Placenta)Document25 pagesAbruptio Placentae: (Accidental Hemorrhage, Premature Separation of Placenta)Akashdeep singhNo ratings yet
- PCFM Case DiscussionDocument17 pagesPCFM Case DiscussionJoherNo ratings yet
- (Surgery) Midterms PediatricsDocument5 pages(Surgery) Midterms Pediatricsalmira.s.mercadoNo ratings yet
- Approach To Seizures in ChildrenDocument12 pagesApproach To Seizures in ChildrenShamen KohNo ratings yet
- Increased Intracranial Pressure and Seizure Feb 14Document2 pagesIncreased Intracranial Pressure and Seizure Feb 14anime listNo ratings yet
- DysphagiaDocument2 pagesDysphagiaKimberlyLaw95No ratings yet
- Osmosis Esophageal Disease PDF Amm DR NotesDocument13 pagesOsmosis Esophageal Disease PDF Amm DR NotestajammalNo ratings yet
- VERTIGO Dr. Wirawan BaruDocument46 pagesVERTIGO Dr. Wirawan BaruSari CuuNo ratings yet
- Emergency Transient Loss of Consciousness1Document6 pagesEmergency Transient Loss of Consciousness1ananNo ratings yet
- Drug StudyDocument21 pagesDrug StudyRhuby Pascual AbenojaNo ratings yet
- Inv A Sion Pha Se: Bill Julius Samuel G. Alferez BSN IiiDocument1 pageInv A Sion Pha Se: Bill Julius Samuel G. Alferez BSN IiiRudelsa Agcolicol LangamanNo ratings yet
- Testicular Torsion, Peds Cases NotesDocument1 pageTesticular Torsion, Peds Cases NotesdzalhcNo ratings yet
- Pernicious AnemiaDocument28 pagesPernicious AnemiaEncee MianNo ratings yet
- Chest Pain EvaluationDocument2 pagesChest Pain Evaluatione-MedTools100% (5)
- Vertigo Vertigo: Pembimbing: Dr. Nella, Sp. SDocument40 pagesVertigo Vertigo: Pembimbing: Dr. Nella, Sp. SAbdil AbdelNo ratings yet
- The Psychology of Hysteria - A Selection of Classic Articles on the Analysis and Symptoms of HysteriaFrom EverandThe Psychology of Hysteria - A Selection of Classic Articles on the Analysis and Symptoms of HysteriaNo ratings yet
- Vertigo, A Simple Guide to The Condition, Treatment And Related ConditionsFrom EverandVertigo, A Simple Guide to The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Clinical Approach To A Patient With Dysphagia: Medicine UpdateDocument3 pagesClinical Approach To A Patient With Dysphagia: Medicine UpdateAnonymous XFDJfsGviNo ratings yet
- Gastrointestinal System DisordersDocument112 pagesGastrointestinal System DisordersTaate MohammedNo ratings yet
- The Australian Med Students Study GuideDocument58 pagesThe Australian Med Students Study GuideLydiaNo ratings yet
- Gastroenterology EsophagusDocument2 pagesGastroenterology EsophagusJayanthNo ratings yet
- MCQ Surgery 1Document6 pagesMCQ Surgery 1Abdallah GamalNo ratings yet
- All Previous Essay Surgery 2Document162 pagesAll Previous Essay Surgery 2DR/ AL-saifiNo ratings yet
- Functional Heartburn. An Underrecognized Cause of PPI-refractory Symptoms 2019Document8 pagesFunctional Heartburn. An Underrecognized Cause of PPI-refractory Symptoms 2019Ricardo Robles AlfaroNo ratings yet
- Surgery 3 White Part 1Document87 pagesSurgery 3 White Part 1Håíthãm KhãtïßNo ratings yet
- Bolile EsofagulDocument13 pagesBolile Esofagulelisabeth-ward-skipNo ratings yet
- Esophagus: DrzaiterDocument37 pagesEsophagus: DrzaiterdrynwhylNo ratings yet
- Disorders of Esophagus and StomachDocument29 pagesDisorders of Esophagus and StomachSamuel kuriaNo ratings yet
- 61st Annual Conference of Indian Society of Gastroenterology, Num 04 Virtual Diamond Jubilee ISGCON 2020, 19-20th December 2020Document127 pages61st Annual Conference of Indian Society of Gastroenterology, Num 04 Virtual Diamond Jubilee ISGCON 2020, 19-20th December 2020Chawki MokademNo ratings yet
- Best Practice Guidelines and Cochrane Reviews in Gastroenterology and Hepatology-2019Document573 pagesBest Practice Guidelines and Cochrane Reviews in Gastroenterology and Hepatology-2019Engin UçarNo ratings yet
- Pemicu 1 Blok GIT SintaDocument85 pagesPemicu 1 Blok GIT SintasimranNo ratings yet
- Osmosis Esophageal Disease PDF Amm DR NotesDocument13 pagesOsmosis Esophageal Disease PDF Amm DR NotestajammalNo ratings yet
- 1st LE - Surgery 2Document3 pages1st LE - Surgery 2Valerie Gonzaga-CarandangNo ratings yet
- Dr. Khalid - S Explanation of 1700 MCQ1Document683 pagesDr. Khalid - S Explanation of 1700 MCQ1heba100% (1)
- Dysphagia SurgicalDocument75 pagesDysphagia Surgicalian ismail100% (1)
- CSAMM2014 AbstractBookDocument270 pagesCSAMM2014 AbstractBookAfiqah RahahNo ratings yet
- L28 - Esophageal DiseasesDocument16 pagesL28 - Esophageal DiseasesNimer Abdelhadi AliNo ratings yet
- Nihms 1764910Document62 pagesNihms 1764910afg_19No ratings yet
- EsophagomyotomyDocument3 pagesEsophagomyotomySamVelascoNo ratings yet
- Plab-1 1700 MCQs Solved With Explanation (Shared by Ussama Maqbool)Document729 pagesPlab-1 1700 MCQs Solved With Explanation (Shared by Ussama Maqbool)Omar Abo el nagaNo ratings yet
- Barium SwallowDocument24 pagesBarium SwallowFaria KhanNo ratings yet
- ENT MCQsDocument14 pagesENT MCQsAlmushawth Emmo100% (6)