Download as pdf or txt
You might also like
- Resting Membrane, Graded, Action Potentials AtfDocument4 pagesResting Membrane, Graded, Action Potentials AtfdaphneNo ratings yet
- What Would You DoDocument4 pagesWhat Would You DoNicolas GiraldoNo ratings yet
- Laboratory and Blood Bank Surveillance (Labs) Form 1: Epidemiology BureauDocument1 pageLaboratory and Blood Bank Surveillance (Labs) Form 1: Epidemiology BureauEvo SingsonNo ratings yet
- HIV Testing Labs FlowchartDocument1 pageHIV Testing Labs Flowcharthamody662002No ratings yet
- NPEP Procedure Flowchart TemplateDocument2 pagesNPEP Procedure Flowchart TemplatededekfridayNo ratings yet
- Understanding Your Hepatitis B Blood TestsDocument2 pagesUnderstanding Your Hepatitis B Blood TestsSam Sep A SixtyoneNo ratings yet
- Understanding Your Hepatitis B Blood Tests Fact Sheet Updated January 2020Document2 pagesUnderstanding Your Hepatitis B Blood Tests Fact Sheet Updated January 2020taycolaramae07No ratings yet
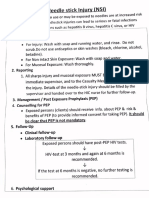
- Protocol Needlestick InjuriesDocument1 pageProtocol Needlestick InjuriesMrLarry Dolor100% (1)
- En - Acc Exposure Blood Body Fluids - PosterDocument1 pageEn - Acc Exposure Blood Body Fluids - Posterdhira aninditaNo ratings yet
- Hepatitis GeneralDocument14 pagesHepatitis GeneralMarysol UlloaNo ratings yet
- PDF DocumentDocument1 pagePDF DocumentellaNo ratings yet
- UTI Diagnostic Flowchart NICE-October 2020-FINALDocument78 pagesUTI Diagnostic Flowchart NICE-October 2020-FINALShaarikh PasandNo ratings yet
- Humanimmunodeficiency Virusinitialassessmentand Routinefollow-UpDocument16 pagesHumanimmunodeficiency Virusinitialassessmentand Routinefollow-UpBriando Stevano LinelejanNo ratings yet
- STEP 1 Could It Be HIV? STEP 2 Informed Consent and Testing STEP 3 Conveying Test ResultsDocument2 pagesSTEP 1 Could It Be HIV? STEP 2 Informed Consent and Testing STEP 3 Conveying Test ResultsahjkseflhasefNo ratings yet
- CDC LSHT STSH Brochure Pep InfographicsDocument2 pagesCDC LSHT STSH Brochure Pep Infographicskistephane5No ratings yet
- Routine HIV Screening in Health Care Settings: Background and DefinitionsDocument23 pagesRoutine HIV Screening in Health Care Settings: Background and Definitionsarya maulanaNo ratings yet
- Penny R. Thayer, FNP, BC Gastro/Hepatology NP James H. Quillen, VAMCDocument27 pagesPenny R. Thayer, FNP, BC Gastro/Hepatology NP James H. Quillen, VAMCPatresya LantanNo ratings yet
- U.S. Preventive Services Task Force (USPSTF) Recommendations - Stats - Medbullets Step 2 - 3Document5 pagesU.S. Preventive Services Task Force (USPSTF) Recommendations - Stats - Medbullets Step 2 - 3mtataNo ratings yet
- Webinar Hepatitis IDI SdaDocument42 pagesWebinar Hepatitis IDI SdaUbed An'threeNo ratings yet
- Hepatitis B SerologijaDocument3 pagesHepatitis B Serologijaxmen menxNo ratings yet
- Information For People We Support: How Do I Get Tested? Other Blood Borne Viruses (BBVS)Document2 pagesInformation For People We Support: How Do I Get Tested? Other Blood Borne Viruses (BBVS)Abhijeet GhorpadeNo ratings yet
- AlemayehuDocument8 pagesAlemayehuasriadiNo ratings yet
- Section 2-Session 4Document29 pagesSection 2-Session 4foleyNo ratings yet
- HIV Infection: Detection, Counseling, and ReferralDocument71 pagesHIV Infection: Detection, Counseling, and ReferralJohn Bocanegra NeriNo ratings yet
- Who Recommends Hiv Self-Testing: Reaching People With Undiagnosed HIVDocument2 pagesWho Recommends Hiv Self-Testing: Reaching People With Undiagnosed HIVtashoneNo ratings yet
- Annex 5-5Document20 pagesAnnex 5-5Dandi PremaNo ratings yet
- Post-Exposure Prophylaxis For Hiv: CDC GuidelinesDocument26 pagesPost-Exposure Prophylaxis For Hiv: CDC GuidelinesnetradeepNo ratings yet
- Management 2Document16 pagesManagement 2Moin PandithNo ratings yet
- HepB Provider Tipsheet 508Document2 pagesHepB Provider Tipsheet 508Jamshaid AhmedNo ratings yet
- Hiv Testing in The Era of Prep:: When The Tests Are DiscordantDocument17 pagesHiv Testing in The Era of Prep:: When The Tests Are DiscordantAldren GilanaNo ratings yet
- Hepatitis B Vaccination PresDocument21 pagesHepatitis B Vaccination PresmaponlooNo ratings yet
- En Abbott Realtime Hiv-1: Customer Service International: Call Your Abbott RepresentativeDocument24 pagesEn Abbott Realtime Hiv-1: Customer Service International: Call Your Abbott RepresentativegdurouxNo ratings yet
- HepatitisDocument2 pagesHepatitismuhammad soffiudinNo ratings yet
- Breastfeeding in Hiv Positive MothersDocument13 pagesBreastfeeding in Hiv Positive MothersBeverly MenendezNo ratings yet
- Anecca 10 Points Poster EnglishDocument1 pageAnecca 10 Points Poster EnglishDrake Wa YesuNo ratings yet
- Dr. Lydia Tandri, SP - PD: Treatment & Guideliness For Hepatitis B-C Virus in Practice ClinicDocument42 pagesDr. Lydia Tandri, SP - PD: Treatment & Guideliness For Hepatitis B-C Virus in Practice ClinicveraanaNo ratings yet
- Adverse Event Reporting PolicyDocument5 pagesAdverse Event Reporting Policycs nagarNo ratings yet
- LabCorpTestingProtocol6 08Document4 pagesLabCorpTestingProtocol6 08Olga CîrsteaNo ratings yet
- CASE ANALYSIS Vincent Parong Patrick TuralbaDocument10 pagesCASE ANALYSIS Vincent Parong Patrick TuralbaisaacdarylNo ratings yet
- Understanding Blood TestsDocument2 pagesUnderstanding Blood TestsAnonymous NUn6MESxNo ratings yet
- United States HIV Testing and Prophylaxis To Prevent Mother-to-Child Transmission in TheDocument10 pagesUnited States HIV Testing and Prophylaxis To Prevent Mother-to-Child Transmission in TheGerry ValdyNo ratings yet
- Blue Orange Creative Diabetes PresentationDocument8 pagesBlue Orange Creative Diabetes PresentationFernando MunaycoNo ratings yet
- Clinical Guideline: HIV in PregnancyDocument18 pagesClinical Guideline: HIV in PregnancyM Iqbal EffendiNo ratings yet
- Management of Human Immunodeficiency Virus Infection (HIV)Document1 pageManagement of Human Immunodeficiency Virus Infection (HIV)zenagit123456No ratings yet
- Pre Employment Health AssessmentDocument7 pagesPre Employment Health AssessmentMP13No ratings yet
- Sharp Injury Surveillance CMEDocument47 pagesSharp Injury Surveillance CMENOR HASSIDANo ratings yet
- Understanding Blood Tests PDFDocument2 pagesUnderstanding Blood Tests PDFKishor SinghNo ratings yet
- Heatlh Care ProfessionalDocument2 pagesHeatlh Care ProfessionalawangbokNo ratings yet
- Hepatitis B in PregnancyDocument12 pagesHepatitis B in PregnancyTasya Felicia MacellinNo ratings yet
- Multisystem & Genetic - BoardsDocument10 pagesMultisystem & Genetic - BoardsSoojung NamNo ratings yet
- Prevention of Parent To Child Transmission of HIV : Dr. ShobhaDocument52 pagesPrevention of Parent To Child Transmission of HIV : Dr. ShobhajijaniNo ratings yet
- CDC Hiv Pep101Document2 pagesCDC Hiv Pep101Sangeetha HospitalNo ratings yet
- Needle: Stick Injury (NSI)Document5 pagesNeedle: Stick Injury (NSI)dr rajoreNo ratings yet
- Chronic He PB Testing FL W UpDocument2 pagesChronic He PB Testing FL W UpSumit MitraNo ratings yet
- Hepatitis B PDFDocument15 pagesHepatitis B PDFAvicenna_MSCNo ratings yet
- AFAO HIV in Australia 2022Document2 pagesAFAO HIV in Australia 2022Yingying LiNo ratings yet
- DOH 2021 Interim Guidelines PrEPDocument6 pagesDOH 2021 Interim Guidelines PrEPithran khoNo ratings yet
- Hepatitis Viral - Dr. José Gonzáles BenavidesDocument64 pagesHepatitis Viral - Dr. José Gonzáles BenavidesEfrain Brian SilvaNo ratings yet
- Hepatitis B (HepB Vaccine)Document6 pagesHepatitis B (HepB Vaccine)Desiree EscobidoNo ratings yet
- Management of Hepatitis B in Pregnancy C Obs 50Document17 pagesManagement of Hepatitis B in Pregnancy C Obs 50EndaleNo ratings yet
- MT 6322 - Mycology and Virology 2nd Shifting OLADocument9 pagesMT 6322 - Mycology and Virology 2nd Shifting OLAlily bluesNo ratings yet
- Pre-Exposure Prophylaxis (PrEP) For HIV Prevention: A Beginners Guide to PrEP for HIV Prevention.From EverandPre-Exposure Prophylaxis (PrEP) For HIV Prevention: A Beginners Guide to PrEP for HIV Prevention.No ratings yet
- ECG Notes - Eng - Doubell 2016Document57 pagesECG Notes - Eng - Doubell 2016MaleehaNo ratings yet
- Local Anaesthetic AgentsDocument43 pagesLocal Anaesthetic AgentsMaleehaNo ratings yet
- Andre Tans Surgery Notes Compiled-1Document117 pagesAndre Tans Surgery Notes Compiled-1MaleehaNo ratings yet
- 8.health Professional Act (See Only)Document65 pages8.health Professional Act (See Only)MaleehaNo ratings yet
- RenalDocument134 pagesRenalMaleehaNo ratings yet
- RenalDocument4 pagesRenalMaleehaNo ratings yet
- KERRIER Kit Mixing Instructions Rev 1 3Document3 pagesKERRIER Kit Mixing Instructions Rev 1 3jpsbhandalNo ratings yet
- Name of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesDocument2 pagesName of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesKarl Lourenz DeysolongNo ratings yet
- Research Secondary HypertensionDocument51 pagesResearch Secondary HypertensionDomeng TalksNo ratings yet
- Treatment of Angina Pectoris-2Document19 pagesTreatment of Angina Pectoris-2Habib UllahNo ratings yet
- Becozyme AmpDocument1 pageBecozyme AmpMohammed IbrahimNo ratings yet
- Poster Template - SYMPOSIUM 2023 (1) 2Document1 pagePoster Template - SYMPOSIUM 2023 (1) 2Ana PopoviciNo ratings yet
- SPC - Vpa22664-150-001Document5 pagesSPC - Vpa22664-150-001hallaqyara8No ratings yet
- Zantac (Ranitidine) - Safety Information - NDMA Found in Samples of Some Ranitidine Medicines - FDADocument2 pagesZantac (Ranitidine) - Safety Information - NDMA Found in Samples of Some Ranitidine Medicines - FDACuam CaracasNo ratings yet
- Geriatric PsychiatryDocument91 pagesGeriatric PsychiatryVipindeep SandhuNo ratings yet
- Ampi+Salbactum Amo+ Clavulanate Piper+Tazobactam: ST ST ND ND ND ND TH ST ND TH TH TH RD RD RD TH THDocument1 pageAmpi+Salbactum Amo+ Clavulanate Piper+Tazobactam: ST ST ND ND ND ND TH ST ND TH TH TH RD RD RD TH THAnnieNo ratings yet
- Anti Hypertensive DrugsDocument40 pagesAnti Hypertensive DrugsjawadNo ratings yet
- LT208 RIQAS EQA Programmes SEP20Document8 pagesLT208 RIQAS EQA Programmes SEP20PannaMkNo ratings yet
- Can Ethnopharmacology Contribute To The Dev of Antiviral Drug - Vlietinck1991Document13 pagesCan Ethnopharmacology Contribute To The Dev of Antiviral Drug - Vlietinck1991Tyasmeita14No ratings yet
- Review Article: DPP-4 Inhibitors As Treatments For Type 1 Diabetes Mellitus: A Systematic Review and Meta-AnalysisDocument11 pagesReview Article: DPP-4 Inhibitors As Treatments For Type 1 Diabetes Mellitus: A Systematic Review and Meta-AnalysisGREESTYNo ratings yet
- Endorsement SheetDocument2 pagesEndorsement SheetGabilou Danao BunuanNo ratings yet
- indica) as α-glucosidase inhibitor and: Endosperm of Indramayu mango (Mangifera antioxidantDocument7 pagesindica) as α-glucosidase inhibitor and: Endosperm of Indramayu mango (Mangifera antioxidantAdriani HasyimNo ratings yet
- Vinayaka College of Nursing Nadiad: Time Table 2 Year B.SC NursingDocument1 pageVinayaka College of Nursing Nadiad: Time Table 2 Year B.SC NursingSiddhiNo ratings yet
- Pone 0214727Document14 pagesPone 0214727Inanda DamantiaNo ratings yet
- KRONE Products We Manufacturer - Updated List NewDocument11 pagesKRONE Products We Manufacturer - Updated List Newneeraj kumar100% (1)
- Pharmaceutical Calculations Course OutlineDocument2 pagesPharmaceutical Calculations Course OutlineAmiir KooNo ratings yet
- Toxicology: DR Frank Kakuba G MD, Mmed Path (Mak)Document24 pagesToxicology: DR Frank Kakuba G MD, Mmed Path (Mak)Mwanja MosesNo ratings yet
- AtracuriumDocument1 pageAtracuriumMohammed IbrahimNo ratings yet
- Price List - Ist Sept.2015 PDFDocument2 pagesPrice List - Ist Sept.2015 PDFMohammed shamiul ShahidNo ratings yet
- ITP Review ArticleDocument12 pagesITP Review ArticleMuhammad FauzanNo ratings yet
- BioanalyticalMethodDevelopment PDFDocument10 pagesBioanalyticalMethodDevelopment PDFvikram kushwahaNo ratings yet
- S. B. No. 2573: Second Regular SessionDocument13 pagesS. B. No. 2573: Second Regular SessionmkoguicoNo ratings yet
- Acne DissertationDocument6 pagesAcne DissertationPaySomeoneToDoMyPaperUK100% (1)
- First Aid Management of HemorrhageDocument68 pagesFirst Aid Management of HemorrhageAbdulaziz AlharbiNo ratings yet