Download as pdf or txt
You might also like
- Letter To The Editor: ReferencesDocument1 pageLetter To The Editor: ReferencesUmer HussainNo ratings yet
- Osteochondral Lesions of The Knee Differentiating The Most Common Entities at MRI ODLICNODocument18 pagesOsteochondral Lesions of The Knee Differentiating The Most Common Entities at MRI ODLICNOdrbane123No ratings yet
- MRI Changes in The Temporomandibular Joint After Mandibular AdvancementDocument7 pagesMRI Changes in The Temporomandibular Joint After Mandibular AdvancementNaveenNo ratings yet
- Glomus 2020Document10 pagesGlomus 2020Ezequías PortilloNo ratings yet
- Panduan Praktik Klinis OsteomielitisDocument4 pagesPanduan Praktik Klinis OsteomielitisAstri HapsariNo ratings yet
- Pi Is 0363502317302241Document5 pagesPi Is 0363502317302241ashik MohamedNo ratings yet
- Nippolainen2020 Article NearInfraredSpectroscopyEnableDocument11 pagesNippolainen2020 Article NearInfraredSpectroscopyEnablebilel_seifNo ratings yet
- Vi 2Document8 pagesVi 2Diego Ivan IslasNo ratings yet
- In Vivo Measurement of Shear Modulus of The Human Cornea Using Optical Coherence ElastographyDocument10 pagesIn Vivo Measurement of Shear Modulus of The Human Cornea Using Optical Coherence ElastographyovyNo ratings yet
- Biopsy of Musculoskeletal Tumors: BackgroundDocument9 pagesBiopsy of Musculoskeletal Tumors: BackgroundK ENo ratings yet
- Functional Outcomes of Nonunion Scaphoid Fracture Treated by PDFDocument6 pagesFunctional Outcomes of Nonunion Scaphoid Fracture Treated by PDFHazorthoNo ratings yet
- Neurosurgical Focus An Introductory Overview of Orbital TumorsDocument9 pagesNeurosurgical Focus An Introductory Overview of Orbital Tumorsnadia emildaNo ratings yet
- Chondral Tumours - Discrepancy Rate Between Needle Biopsy and Surgical HistologyDocument11 pagesChondral Tumours - Discrepancy Rate Between Needle Biopsy and Surgical Histologychenth3r3No ratings yet
- Four-Segment Classification of Proximal Humeral Fractures - Purpose and Reliable Use - Neer2002Document12 pagesFour-Segment Classification of Proximal Humeral Fractures - Purpose and Reliable Use - Neer2002lliuyueeNo ratings yet
- Prevalence and Predictors of Hering S Response In.7Document6 pagesPrevalence and Predictors of Hering S Response In.7Ariana VelasquezNo ratings yet
- NIH Public Access: Author ManuscriptDocument28 pagesNIH Public Access: Author ManuscriptEka JuliantaraNo ratings yet
- Intramural Unicystic Ameloblastoma: Journal of The College of Physicians and Surgeons - Pakistan: JCPSP March 2017Document3 pagesIntramural Unicystic Ameloblastoma: Journal of The College of Physicians and Surgeons - Pakistan: JCPSP March 2017dr.filipcristian87No ratings yet
- Endoscopic Resection of Symptomatic Osteochondroma of The Distal FemurDocument4 pagesEndoscopic Resection of Symptomatic Osteochondroma of The Distal FemurAlex CirlanNo ratings yet
- Antony2017 PDFDocument8 pagesAntony2017 PDFM. JahangirNo ratings yet
- Antony2017 PDFDocument8 pagesAntony2017 PDFM. JahangirNo ratings yet
- Role of Magnetic Resonance Imaging in The Management of Patients With Multiple Myeloma A Consensus Statement JClinOncol-Feb2015Document12 pagesRole of Magnetic Resonance Imaging in The Management of Patients With Multiple Myeloma A Consensus Statement JClinOncol-Feb2015Andy LNo ratings yet
- The Meniscus Is A Fibercartilagenous Structure, Which Plays A Significant Role in MaintainingDocument7 pagesThe Meniscus Is A Fibercartilagenous Structure, Which Plays A Significant Role in MaintainingStefan StefNo ratings yet
- Cartilage Injury in The Knee Assessment And.2Document9 pagesCartilage Injury in The Knee Assessment And.2cooperorthopaedicsNo ratings yet
- Subaxial Cervical Spine Trauma: Evaluation and Surgical Decision-MakingDocument7 pagesSubaxial Cervical Spine Trauma: Evaluation and Surgical Decision-Makingvicky174No ratings yet
- 1-S2.0-S0020138322001954-MainDocument6 pages1-S2.0-S0020138322001954-MainSeptianNo ratings yet
- Sinha 2020Document10 pagesSinha 2020ABKarthikeyanNo ratings yet
- Save The MeniscusDocument8 pagesSave The MeniscusRocio CabreraNo ratings yet
- Bicondylar Tibial PlateauDocument7 pagesBicondylar Tibial PlateauMin Banyar AungNo ratings yet
- Tripathy 2015Document19 pagesTripathy 2015Someshwar GuptNo ratings yet
- PDF Hosted at The Radboud Repository of The Radboud University NijmegenDocument5 pagesPDF Hosted at The Radboud Repository of The Radboud University NijmegenGazal KhanNo ratings yet
- ch13Document6 pagesch13boopathiraja.chinnasamyNo ratings yet
- Ijcmr 1538 3Document8 pagesIjcmr 1538 3drelvNo ratings yet
- Proceedings of The 16th Italian Association of Equine Veterinarians CongressDocument5 pagesProceedings of The 16th Italian Association of Equine Veterinarians CongressCabinet VeterinarNo ratings yet
- 1990 JBJS VANCOUVER External Fixation and Delayed Intramedullary Nailing of Open Fractures of The Tibial Shaft. A Sequential ProtocolDocument8 pages1990 JBJS VANCOUVER External Fixation and Delayed Intramedullary Nailing of Open Fractures of The Tibial Shaft. A Sequential ProtocolnireguiNo ratings yet
- Retromandibular Approach To The Mandibular Condyle: A Clinical and Cadaveric StudyDocument4 pagesRetromandibular Approach To The Mandibular Condyle: A Clinical and Cadaveric StudyNachiketa parikhNo ratings yet
- 2009 Article 52Document7 pages2009 Article 52vanessa_werbickyNo ratings yet
- Le Mound 2017Document9 pagesLe Mound 2017Nadia RamírezNo ratings yet
- CME1020 RadiologyDocument10 pagesCME1020 Radiologyeternal sunshineNo ratings yet
- Musculoskeletal Sports Ultrasound.1Document2 pagesMusculoskeletal Sports Ultrasound.1Mateus AssisNo ratings yet
- Evaluation of Intraoral Verticosagittal Hashemi2008Document4 pagesEvaluation of Intraoral Verticosagittal Hashemi2008carolina vega hernandezNo ratings yet
- Fractura Metafisaria Distal de TibiaDocument9 pagesFractura Metafisaria Distal de TibiaCirian Perez FuentesNo ratings yet
- CBCT in OA PDFDocument8 pagesCBCT in OA PDFHồ TiênNo ratings yet
- Inside Out Menico RampaDocument6 pagesInside Out Menico RampaNilia AbadNo ratings yet
- Reamed Versus UnreamedDocument9 pagesReamed Versus UnreamedthanawatsimaNo ratings yet
- Subaxial Cervical Spine Trauma: Evaluation and Surgical Decision-MakingDocument8 pagesSubaxial Cervical Spine Trauma: Evaluation and Surgical Decision-Makingvicky174No ratings yet
- Tian 2012Document6 pagesTian 2012Orto MespNo ratings yet
- Cios 4 129Document5 pagesCios 4 129kansamotor.autopartNo ratings yet
- Magnetic Resonance Imaging (MRI) of The Knee: Identification of Difficult-To-Diagnose Meniscal LesionsDocument10 pagesMagnetic Resonance Imaging (MRI) of The Knee: Identification of Difficult-To-Diagnose Meniscal LesionsDanaAmaranducaiNo ratings yet
- Ajnr A5528 FullDocument9 pagesAjnr A5528 FullMehranNasrallaNo ratings yet
- Tiempo y FracturaDocument7 pagesTiempo y FracturaPedro TorresNo ratings yet
- Effectiveness of Ocriplasmin in Real World Settings A Systematic Literature Review, Meta Analysis, and Comparison With Randomized TrialsDocument14 pagesEffectiveness of Ocriplasmin in Real World Settings A Systematic Literature Review, Meta Analysis, and Comparison With Randomized Trialsmistic0No ratings yet
- Corneal Neurotization: A Novel Solution To Neurotrophic KeratopathyDocument9 pagesCorneal Neurotization: A Novel Solution To Neurotrophic KeratopathyJosé Castro SoaresNo ratings yet
- Brainstem Cavernous MalformationDocument22 pagesBrainstem Cavernous MalformationIwan SurotoNo ratings yet
- s41420 021 00418 yDocument15 pagess41420 021 00418 yValen EstevezNo ratings yet
- Orthopedic JournalDocument9 pagesOrthopedic JournalAdinarayana KashyapNo ratings yet
- Distal Humerus Fractures: Roongsak Limthongthang, MD, and Jesse B. Jupiter, MDDocument10 pagesDistal Humerus Fractures: Roongsak Limthongthang, MD, and Jesse B. Jupiter, MDRadu UrcanNo ratings yet
- Shoulder 2 Ada MriDocument4 pagesShoulder 2 Ada MriNirmalasari AnirNo ratings yet
- Dens FractureDocument10 pagesDens Fracturenberwar090No ratings yet
- Surgery of the Cranio-Vertebral JunctionFrom EverandSurgery of the Cranio-Vertebral JunctionEnrico TessitoreNo ratings yet
- Oculopathy: Disproves the orthodox and theoretical bases upon which glasses are so freely prescribed, and puts forward natural remedial methods of treatment for what are sometimes termed incurable visual defectsFrom EverandOculopathy: Disproves the orthodox and theoretical bases upon which glasses are so freely prescribed, and puts forward natural remedial methods of treatment for what are sometimes termed incurable visual defectsNo ratings yet
- Clinical and RadiographicDocument2 pagesClinical and RadiographicJose IgnacioNo ratings yet
- Onmam 5Document1 pageOnmam 5Jose IgnacioNo ratings yet
- Pathogenesis ONMAM - Final Bueno para Desconocimiento de BronjDocument10 pagesPathogenesis ONMAM - Final Bueno para Desconocimiento de BronjJose IgnacioNo ratings yet
- Bibliometric Analysis of Medication Related Osteonecrosis of The Jaw HighDocument17 pagesBibliometric Analysis of Medication Related Osteonecrosis of The Jaw HighJose IgnacioNo ratings yet
- A Review On Tecoma StansDocument3 pagesA Review On Tecoma StansBaru Chandrasekhar RaoNo ratings yet
- Activity 18 AgingDocument27 pagesActivity 18 AgingKendrix Aguiluz FlorendoNo ratings yet
- Cancer Immunotherapy: Dra. Cristina Nadal Oncologia Medica Hospital Clinic BarcelonaDocument63 pagesCancer Immunotherapy: Dra. Cristina Nadal Oncologia Medica Hospital Clinic BarcelonaOlga Peña HernandezNo ratings yet
- Cocoa Pest ManagementDocument13 pagesCocoa Pest ManagementAprilia WilonaNo ratings yet
- Office Work HiraDocument2 pagesOffice Work HiratirthNo ratings yet
- Streeoverlord PIDocument1 pageStreeoverlord PIdoobiedoodooNo ratings yet
- NewEarth - University COVID-19 Intelligence BriefDocument47 pagesNewEarth - University COVID-19 Intelligence BriefTony Lambert100% (1)
- Charles Mann ProbableDocument2 pagesCharles Mann ProbableKIRO 7 Eyewitness NewsNo ratings yet
- M PostpartumDocument23 pagesM PostpartumDonaJeanNo ratings yet
- Prakriti Analysis of COVID 19 Patients: An Observational StudyDocument12 pagesPrakriti Analysis of COVID 19 Patients: An Observational StudySaurabh SumanNo ratings yet
- 28-Abhishek TiwariDocument3 pages28-Abhishek TiwariAbhishek TiwariNo ratings yet
- Tension Pneumothorax PDFDocument2 pagesTension Pneumothorax PDFClarissa Aileen Caliva AdoraNo ratings yet
- THROMBOSISDocument18 pagesTHROMBOSISShruti Verma100% (1)
- Hoërskool Roodepoort: COVID-19 PolicyDocument24 pagesHoërskool Roodepoort: COVID-19 PolicyScarfacembali MbaliNo ratings yet
- Daftar Puastaka BaruuuDocument2 pagesDaftar Puastaka BaruuuEvan AninditoNo ratings yet
- Nota Biologi Tingkatan 4 BAB 2Document12 pagesNota Biologi Tingkatan 4 BAB 2Firas Muhammad100% (2)
- Addiction Recovery ManagementDocument71 pagesAddiction Recovery ManagementThe Stacie Mathewson FoundationNo ratings yet
- Actualizacion de La PreeclampsiaDocument8 pagesActualizacion de La PreeclampsiaPierina VeramatosNo ratings yet
- California Mastitis Test (CMT) : BackgroundDocument2 pagesCalifornia Mastitis Test (CMT) : BackgroundAriel VicenteNo ratings yet
- Skin Cancer Detection Using Multi-Scale Deep Learning and Transfer LearningDocument9 pagesSkin Cancer Detection Using Multi-Scale Deep Learning and Transfer Learningcerberus thanatosNo ratings yet
- Final Study Guide 2020 - Nursing 1119Document5 pagesFinal Study Guide 2020 - Nursing 1119KashaNo ratings yet
- MED CERT DR LUNA (Alva)Document4 pagesMED CERT DR LUNA (Alva)Bea Lourrainne de GuzmanNo ratings yet
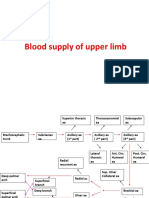
- Blood Supply of Upper LimbDocument36 pagesBlood Supply of Upper Limbteklay100% (2)
- Adolescent HealthDocument47 pagesAdolescent HealthsushmaNo ratings yet
- CBD DR Saugi IrfanDocument88 pagesCBD DR Saugi IrfanFebri BimayanaNo ratings yet
- Zhan ZhuangDocument46 pagesZhan ZhuangAndrzej KaliszNo ratings yet
- Imaging of Solitary and Multiple Pulmonary NodulesDocument75 pagesImaging of Solitary and Multiple Pulmonary NodulesAnshulVarshneyNo ratings yet
- Final Year Project PresentationDocument32 pagesFinal Year Project PresentationAin Shii AmirNo ratings yet
- DNB India Anaesthesia - Sample PaperDocument1 pageDNB India Anaesthesia - Sample PaperChandanJhaNo ratings yet
- Research Paper Topics For Health PromotionDocument8 pagesResearch Paper Topics For Health Promotionafnkaufhczyvbc100% (1)