Download as docx, pdf, or txt
You might also like
- EBOOK Health Psychology 10Th Edition Ebook PDF Download Full Chapter PDF KindleDocument61 pagesEBOOK Health Psychology 10Th Edition Ebook PDF Download Full Chapter PDF Kindlejennifer.meyer98898% (50)
- Anneke LucasDocument11 pagesAnneke LucasMaica Iustina100% (4)
- Oplan Tokhang Thesis Paper, UP DilimanDocument66 pagesOplan Tokhang Thesis Paper, UP DilimanMagtira Paolo85% (41)
- Treating Sex and Porn AddictionDocument28 pagesTreating Sex and Porn AddictionObinna OkaforNo ratings yet
- Stimulus Edn 1 Final ReducedDocument92 pagesStimulus Edn 1 Final Reducedamss_documentsNo ratings yet
- Wa0010.Document8 pagesWa0010.Ronika KashyapNo ratings yet
- Substance Use and Addictive DisordersDocument5 pagesSubstance Use and Addictive DisordersKaye NeeNo ratings yet
- LP - HEALTH 2nd QuarterDocument7 pagesLP - HEALTH 2nd QuarterReca BoltronNo ratings yet
- Detailed Lesson Plan (DLP) Format: 1 MAPEH (Health) 9 2ndDocument6 pagesDetailed Lesson Plan (DLP) Format: 1 MAPEH (Health) 9 2ndHaydee Surait CarpizoNo ratings yet
- Lesson Plan Fonn S.1Document10 pagesLesson Plan Fonn S.1Sandeep MeenaNo ratings yet
- Neurobiological Basis of Drug Reward and Reinforcement: Chapter OutlineDocument18 pagesNeurobiological Basis of Drug Reward and Reinforcement: Chapter Outlineal sharpNo ratings yet
- First-Episode Psychosis and Drug UseDocument54 pagesFirst-Episode Psychosis and Drug UseifclarinNo ratings yet
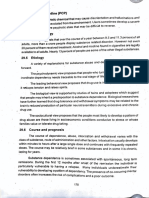
- 29.3.10 Phencyclidine (PCP) Disorientation: Dependency. ComplicationsDocument7 pages29.3.10 Phencyclidine (PCP) Disorientation: Dependency. ComplicationsPsychology StudentNo ratings yet
- Jade Dufour Lesson PlanDocument5 pagesJade Dufour Lesson Planapi-604347267No ratings yet
- Lesson 6 Health (2nd Quarter)Document13 pagesLesson 6 Health (2nd Quarter)Anonymous b6TnI2No ratings yet
- COT-2 HEALTH-Q2-January 19, 2024Document3 pagesCOT-2 HEALTH-Q2-January 19, 2024Angela Marie LoricaNo ratings yet
- Substance AbuseDocument5 pagesSubstance Abusejuliene13No ratings yet
- 06 Addictive and Sexual DisordersDocument58 pages06 Addictive and Sexual DisordersSteven T.No ratings yet
- 1st Psychiatry TransDocument41 pages1st Psychiatry Transmia liaNo ratings yet
- National Service Training Program REVIEWERDocument22 pagesNational Service Training Program REVIEWERdegomajennyrose27No ratings yet
- Module 3Document8 pagesModule 3Jannine Andrei LopezNo ratings yet
- Unit 1 (2markers) - Substance Abuse - Adults and AdolescentsDocument8 pagesUnit 1 (2markers) - Substance Abuse - Adults and Adolescentsriya maliekalNo ratings yet
- Cognitive Behavioural Interventions in Addictive Disorders: Paulomi M. SudhirDocument6 pagesCognitive Behavioural Interventions in Addictive Disorders: Paulomi M. SudhirNorma FloresNo ratings yet
- Module 1 - Drug EducationDocument5 pagesModule 1 - Drug EducationCasandra CalacatNo ratings yet
- Substance-Related DisordersDocument186 pagesSubstance-Related DisordersGirma KelboreNo ratings yet
- Lesson Plan On Ssssybtsnace AbuseDocument7 pagesLesson Plan On Ssssybtsnace Abusepritidinda3070No ratings yet
- Mapeh 9 Lesson PlanDocument2 pagesMapeh 9 Lesson PlanJohnlyndon SinajonNo ratings yet
- Health 2 PDFDocument5 pagesHealth 2 PDFYen Pama RiveroNo ratings yet
- Health Peace Values HGP 5Document4 pagesHealth Peace Values HGP 5SirVin D'chavezNo ratings yet
- CATCHup FRIDAYS Teaching GuideDocument13 pagesCATCHup FRIDAYS Teaching GuideAshley Jane BenlayoNo ratings yet
- Health Education Substance AbuseDocument13 pagesHealth Education Substance Abusekiran mahal100% (2)
- 5.2 Substance Use DisordersDocument40 pages5.2 Substance Use DisordersJacinta SmithNo ratings yet
- Protocol Assignment # 3Document7 pagesProtocol Assignment # 3KenPedresoNo ratings yet
- Substance-Related and Addictive Disorders (Presentation)Document219 pagesSubstance-Related and Addictive Disorders (Presentation)Ryan Wong [Aizen]100% (2)
- Substance-Related and Addictive Disorders (Presentation)Document219 pagesSubstance-Related and Addictive Disorders (Presentation)Ryan Wong [Aizen]No ratings yet
- Social Pharmacy Notes - 1Document5 pagesSocial Pharmacy Notes - 1Gerald Limo Arap ChebiiNo ratings yet
- Vice and Drug Education Control (Module 1) : Trina Valerie D. Merencillo Part-Time InstructorDocument32 pagesVice and Drug Education Control (Module 1) : Trina Valerie D. Merencillo Part-Time InstructorRyan BaylonNo ratings yet
- The Brain Disease Model of Addiction: Butler Center For Research May 2021Document2 pagesThe Brain Disease Model of Addiction: Butler Center For Research May 2021cultura84No ratings yet
- Q2 - Grade 9 - Week 4 - Day 1 - Health - NuestroDocument5 pagesQ2 - Grade 9 - Week 4 - Day 1 - Health - Nuestrorica may nuestroNo ratings yet
- P110.M4.Substance Related Disorders.2023-1Document29 pagesP110.M4.Substance Related Disorders.2023-1Ruth MartinezNo ratings yet
- Grade 9 - Health - LC 3Document6 pagesGrade 9 - Health - LC 3Leah Casano100% (1)
- Substance AbuseDocument17 pagesSubstance AbuseRENEROSE TORRESNo ratings yet
- DRUG LP Jan 21-23Document2 pagesDRUG LP Jan 21-23Jean CatandijanNo ratings yet
- Department of Education Division of Capiz Maayon National High School Maayon, CapizDocument3 pagesDepartment of Education Division of Capiz Maayon National High School Maayon, CapizEmerson Biclar GolipardoNo ratings yet
- Health 2NDDocument21 pagesHealth 2NDJulie AlayonNo ratings yet
- Valencia Colleges (Buk.) Incorporated: NSTP 1: National Service Training Program 1Document6 pagesValencia Colleges (Buk.) Incorporated: NSTP 1: National Service Training Program 1Damon LofrancoNo ratings yet
- Critical Analysis of Research StudyDocument6 pagesCritical Analysis of Research Studykiran mahalNo ratings yet
- Understanding Substance Abuse DisordersDocument8 pagesUnderstanding Substance Abuse DisordersRahul GuptaNo ratings yet
- 2nd Quarter Health Week 1Document6 pages2nd Quarter Health Week 1Jenelyn FailonNo ratings yet
- DRUG PREVENTIONGroup5Document3 pagesDRUG PREVENTIONGroup5jasper pachingelNo ratings yet
- Introduction To Self:: Time Specific Objective Content Teaching AND Learning Activity EvaluationDocument20 pagesIntroduction To Self:: Time Specific Objective Content Teaching AND Learning Activity EvaluationKiran Kour100% (2)
- Addiction Psychiatric MedicineDocument207 pagesAddiction Psychiatric MedicineDragutin Petrić100% (2)
- Bautista LeDocument6 pagesBautista LePRECIOUS BAUTISTANo ratings yet
- Drug Misuse and AbuseDocument5 pagesDrug Misuse and AbusePRECIOUS BAUTISTANo ratings yet
- A Comparative Case Study of Addictive and Non Addictive IndividiualsDocument13 pagesA Comparative Case Study of Addictive and Non Addictive Individiualsdeepikat2005No ratings yet
- Untitled DesignDocument8 pagesUntitled DesignKwon Min RaNo ratings yet
- Finals Topic: Substance Related DisordersDocument26 pagesFinals Topic: Substance Related Disordersエニエルカム オレーバンNo ratings yet
- CDI4002Document11 pagesCDI4002Justine MacapobreNo ratings yet
- Drug Education and Vice ControlDocument16 pagesDrug Education and Vice ControlSinagTalaNo ratings yet
- Substance-Related DisorderDocument2 pagesSubstance-Related DisorderRichelle Delos ReyesNo ratings yet
- Signs and Symptoms of Substance Abuse: OutlineDocument4 pagesSigns and Symptoms of Substance Abuse: OutlineIsabel CastilloNo ratings yet
- DSM & ICD ComparisonDocument6 pagesDSM & ICD ComparisonRyan Wong [Aizen]No ratings yet
- Lesson Plan Fonn S.3Document17 pagesLesson Plan Fonn S.3Sandeep Meena100% (1)
- Determinants of Addiction: Neurobiological, Behavioral, Cognitive, and Sociocultural FactorsFrom EverandDeterminants of Addiction: Neurobiological, Behavioral, Cognitive, and Sociocultural FactorsNo ratings yet
- NephritisDocument20 pagesNephritisSaima ParveenNo ratings yet
- TPR MonitoringDocument6 pagesTPR MonitoringSaima ParveenNo ratings yet
- Circulatory Disturbance - Thombosism, Emolism, ShockDocument16 pagesCirculatory Disturbance - Thombosism, Emolism, ShockSaima ParveenNo ratings yet
- Lesson Plan On SterlizationDocument8 pagesLesson Plan On SterlizationSaima ParveenNo ratings yet
- GNM Vol I Community Health Nursing Part 1 MinDocument490 pagesGNM Vol I Community Health Nursing Part 1 MinSaima ParveenNo ratings yet
- FONDTIONi.v InjectionDocument5 pagesFONDTIONi.v InjectionSaima ParveenNo ratings yet
- Staining Lesson PlanDocument2 pagesStaining Lesson PlanSaima ParveenNo ratings yet
- Unit Allottment Post BSCDocument1 pageUnit Allottment Post BSCSaima ParveenNo ratings yet
- Unit Plan of GNM 1st YrDocument3 pagesUnit Plan of GNM 1st YrSaima Parveen100% (1)
- (Slideshare Downloader La) 63d76c0a0016fDocument21 pages(Slideshare Downloader La) 63d76c0a0016fSaima ParveenNo ratings yet
- CT Sad A ManualDocument309 pagesCT Sad A ManualStephen FreckletonNo ratings yet
- Alcoholism Chapter XxxiiiDocument13 pagesAlcoholism Chapter XxxiiiLian Amascual Claridad BasogNo ratings yet
- Overcoming Alcohol Use Problems - A Cognitive-Behavioral Treatment Program Workbook (2009, Oxford University Press, USA)Document208 pagesOvercoming Alcohol Use Problems - A Cognitive-Behavioral Treatment Program Workbook (2009, Oxford University Press, USA)Sarah Peña100% (1)
- Social Research MethodsDocument12 pagesSocial Research Methodsapi-3825778No ratings yet
- Alcoholism and SmokingDocument41 pagesAlcoholism and SmokingAlbert Azai BautistaNo ratings yet
- Prevention of Rising Alcoholism For Happy and Healthy SocietyDocument15 pagesPrevention of Rising Alcoholism For Happy and Healthy SocietyYusuf MonafNo ratings yet
- Invitation Package For Possible Board of Advisors (At WWW - Cpcsc.info)Document611 pagesInvitation Package For Possible Board of Advisors (At WWW - Cpcsc.info)Stefan PastiNo ratings yet
- En Bigbook Chapt2 PDFDocument13 pagesEn Bigbook Chapt2 PDFAmina IbrahimNo ratings yet
- Substance Use Disorder - Manual For PhysiciansDocument213 pagesSubstance Use Disorder - Manual For PhysiciansRoh JitenNo ratings yet
- Addiction Part 1 Benzodiazepines Side Effects, About Risk and AlternativesDocument11 pagesAddiction Part 1 Benzodiazepines Side Effects, About Risk and AlternativesEga Candra FaurizaNo ratings yet
- Practical Research GilDocument14 pagesPractical Research Giljohn lloyd gil100% (1)
- The Doctor-Patient RelationshipDocument9 pagesThe Doctor-Patient Relationshipravi dadlani parasramNo ratings yet
- Provide Responsible Service of Alcohol BookletDocument8 pagesProvide Responsible Service of Alcohol BookletNicky HarreNo ratings yet
- The Spychiatrists, by Frater PyramidatusDocument76 pagesThe Spychiatrists, by Frater PyramidatusBrian Adam Newman (Frater Pyramidatus)100% (2)
- Integrating Object Relations and Alcoholics Anonymous Principles in The Treatment of Schizoid Personality DisorderDocument16 pagesIntegrating Object Relations and Alcoholics Anonymous Principles in The Treatment of Schizoid Personality DisorderMaria Fernanda HiguitaNo ratings yet
- 0-Detachment With LoveDocument1 page0-Detachment With LovePotenciar teNo ratings yet
- KanabisDocument8 pagesKanabisFadil MuhammadNo ratings yet
- Year 11 Alcoholic Beverages The Mother of All EvilsDocument3 pagesYear 11 Alcoholic Beverages The Mother of All EvilsSam ManNo ratings yet
- Reading On Substance Abuse-MataDocument13 pagesReading On Substance Abuse-MataNicole Keesha MataNo ratings yet
- Uncle ErnestDocument10 pagesUncle ErnestJaroos MohamedNo ratings yet
- Suicide and Its Prevention: The Urgent Need in India: Lakshmi VijaykumarDocument4 pagesSuicide and Its Prevention: The Urgent Need in India: Lakshmi VijaykumarJona JoyNo ratings yet
- The Adverse Childhood Experiences (ACE) StudyDocument14 pagesThe Adverse Childhood Experiences (ACE) Studyalongtheheavens100% (5)
- substanceuseAPA PDFDocument130 pagessubstanceuseAPA PDFAušrinė RadišauskaitėNo ratings yet
- Community Health Nursing Care PlanDocument4 pagesCommunity Health Nursing Care Plankate russelNo ratings yet
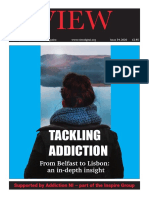
- Tackling Addiction: From Belfast To Lisbon: An In-Depth InsightDocument32 pagesTackling Addiction: From Belfast To Lisbon: An In-Depth InsightSonia EstevesNo ratings yet