Download as pdf or txt
You might also like
- Drug Discovery and DevelopmentDocument47 pagesDrug Discovery and DevelopmentSalahBensaber100% (3)
- Supercritical Fluid Technology For Drug Product Development (2004)Document688 pagesSupercritical Fluid Technology For Drug Product Development (2004)Regiani Almeida Rezende100% (1)
- NSU-Introduction To Drug DiscoveryDocument42 pagesNSU-Introduction To Drug DiscoveryAmina Akther Mim 1821179649No ratings yet
- In-Silico Drug Designing: - Drug Discovery and DevelopmentDocument3 pagesIn-Silico Drug Designing: - Drug Discovery and DevelopmentSeemron BiswalNo ratings yet
- Lecture 8 Drug DesigningDocument22 pagesLecture 8 Drug DesigningMaleeha HussainNo ratings yet
- Drug Targets and Drug DesigningDocument32 pagesDrug Targets and Drug DesigningUmair MazharNo ratings yet
- "Probability and Statistics" " (ASSIGNMENT #2) "Document24 pages"Probability and Statistics" " (ASSIGNMENT #2) "ahmedNo ratings yet
- Instrumental Techniques in Drug DiscoveryDocument110 pagesInstrumental Techniques in Drug Discoverykunasahu1No ratings yet
- DrugDocument17 pagesDrugprinceoftolgateNo ratings yet
- Chapter 2 - ProductDocument69 pagesChapter 2 - Productbassamnader566No ratings yet
- Kimia Medisinal 4Document18 pagesKimia Medisinal 4Dangsony DangNo ratings yet
- Term Paper: Various Techniques in Drug SynthesisDocument14 pagesTerm Paper: Various Techniques in Drug SynthesisUmair MazharNo ratings yet
- Wk7 FunMed - 5. Drug Discovery (DR Malekigorji)Document43 pagesWk7 FunMed - 5. Drug Discovery (DR Malekigorji)ziaduddinNo ratings yet
- DRA Unit 1Document44 pagesDRA Unit 1Oyshi RaoNo ratings yet
- MedicinalDocument165 pagesMedicinalPolitic FeverNo ratings yet
- Pengembangan Obat BaruDocument20 pagesPengembangan Obat BaruDwi Nurma YunitaNo ratings yet
- Bioinformatics in Drug Discovery A ReviewDocument3 pagesBioinformatics in Drug Discovery A ReviewBONFRINGNo ratings yet
- Unit 1 Notes DRADocument10 pagesUnit 1 Notes DRASkb ArsalaanNo ratings yet
- Computer Aided Drug DesignDocument53 pagesComputer Aided Drug DesignVidya M50% (2)
- Drug DevelopmentDocument26 pagesDrug DevelopmentHujjat UllahNo ratings yet
- Introduction To Drug DiscoveryDocument20 pagesIntroduction To Drug DiscoveryNarutoNo ratings yet
- Drug Development: FDA's Definition of A New DrugDocument11 pagesDrug Development: FDA's Definition of A New DrugSophie MendezNo ratings yet
- The Time From Conception To Approval of A New Drug Is Typically 12Document6 pagesThe Time From Conception To Approval of A New Drug Is Typically 12MomaNo ratings yet
- Computational Modelling in Drug DiscoveryDocument44 pagesComputational Modelling in Drug DiscoverySalna Susan AbrahamNo ratings yet
- New Drug Development DR G A WaghmareDocument55 pagesNew Drug Development DR G A WaghmareRia AdrianiNo ratings yet
- Drug Design and DevelopmentDocument5 pagesDrug Design and DevelopmentMark Russel Sean LealNo ratings yet
- Rational Drug DesignDocument25 pagesRational Drug DesignWaseem KhanNo ratings yet
- Introduction To Medicinal Chemistry 1431 PDFDocument230 pagesIntroduction To Medicinal Chemistry 1431 PDFjames mellaleievNo ratings yet
- Preclinical Drug Discovery and Development: David S. DuchDocument26 pagesPreclinical Drug Discovery and Development: David S. DuchAkanksha PatelNo ratings yet
- Final Project LevofloxacinDocument102 pagesFinal Project LevofloxacinJalwaz TihamiNo ratings yet
- Computational Drug Discovery Is A Field of Research That Utilizes Computational Techniques and Methods To Discover and Design New DrugsDocument10 pagesComputational Drug Discovery Is A Field of Research That Utilizes Computational Techniques and Methods To Discover and Design New Drugs21056745003No ratings yet
- Drug Discovery and Development Lecture NotesDocument75 pagesDrug Discovery and Development Lecture NotesJameel BakhshNo ratings yet
- YMER2201F7Document20 pagesYMER2201F7Kausik SenNo ratings yet
- Introduction To Drug Discovery and DevelopmentDocument25 pagesIntroduction To Drug Discovery and Developmentafnanosman2002No ratings yet
- Drug Discovery StrategiesDocument5 pagesDrug Discovery Strategiesminad53929 dineroacom100% (1)
- BMMDocument19 pagesBMMRitika agrawalNo ratings yet
- Biomedical Applications of Functionalized Nanomaterials: Concepts, Development and Clinical TranslationFrom EverandBiomedical Applications of Functionalized Nanomaterials: Concepts, Development and Clinical TranslationNo ratings yet
- Drug Development Process - Part 1Document19 pagesDrug Development Process - Part 1thang nguyen100% (1)
- Medicinal QUIMICADocument53 pagesMedicinal QUIMICAIsmael RodriguezNo ratings yet
- PreClinical Development FinalDocument60 pagesPreClinical Development FinalSayed jannat fatemaNo ratings yet
- 06 - Chapter 1Document37 pages06 - Chapter 1Vikash KushwahaNo ratings yet
- N Asmita Bandyopadhyay 2233645 - Cia IDocument10 pagesN Asmita Bandyopadhyay 2233645 - Cia IN ASMITA BANDYOPADHYAY 2233645No ratings yet
- Computer Aided Drug DesigningDocument19 pagesComputer Aided Drug DesigningPitchumaniangayarkanni S.No ratings yet
- Computer Aided Drug Design Unit 1Document19 pagesComputer Aided Drug Design Unit 1krithigaNo ratings yet
- Drug DevelopmentDocument96 pagesDrug DevelopmentSheena GagarinNo ratings yet
- Role of Toxicopathologist in Drug Discovery and DevelopmentDocument22 pagesRole of Toxicopathologist in Drug Discovery and DevelopmentinnocentjeevaNo ratings yet
- DRUG DesignDocument19 pagesDRUG DesignAmit SharmaNo ratings yet
- Current Trends in Drug Discovery Target Identifica PDFDocument5 pagesCurrent Trends in Drug Discovery Target Identifica PDFKashish GuptaNo ratings yet
- Intracellular Delivery of Nanoparticles in Infectious DiseasesDocument19 pagesIntracellular Delivery of Nanoparticles in Infectious Diseasessanjana jainNo ratings yet
- Unit 5-Bioinformatics-DRUG DISCOVERY-02.01.22Document8 pagesUnit 5-Bioinformatics-DRUG DISCOVERY-02.01.2220SMB24 - ShafanaNo ratings yet
- Dddl1 IntroductionDocument52 pagesDddl1 Introductionsttechon.aljeronmedicalNo ratings yet
- Drug DevelopmentDocument17 pagesDrug DevelopmentMelissa STanNo ratings yet
- CCS0053 - M4 - NewDocument34 pagesCCS0053 - M4 - NewMarvin PanaliganNo ratings yet
- S7a SeminarDocument32 pagesS7a SeminarFarhan SkNo ratings yet
- Drug DesignDocument28 pagesDrug DesignDr Nilesh Patel0% (1)
- AI in Drug DiscoveryDocument23 pagesAI in Drug Discoverygowtham sai100% (2)
- Divij Gulati FInalDocument45 pagesDivij Gulati FInalDivij GulatiNo ratings yet
- ICH Safety GuidelinesDocument28 pagesICH Safety GuidelinesTanvi PardhiNo ratings yet
- Overcoming Obstacles in Drug Discovery and Development: Surmounting the Insurmountable—Case Studies for Critical ThinkingFrom EverandOvercoming Obstacles in Drug Discovery and Development: Surmounting the Insurmountable—Case Studies for Critical ThinkingKan HeNo ratings yet
- A Pharmacology Primer: Techniques for More Effective and Strategic Drug DiscoveryFrom EverandA Pharmacology Primer: Techniques for More Effective and Strategic Drug DiscoveryRating: 1 out of 5 stars1/5 (1)
- Prodrug Design: Perspectives, Approaches and Applications in Medicinal ChemistryFrom EverandProdrug Design: Perspectives, Approaches and Applications in Medicinal ChemistryRating: 3 out of 5 stars3/5 (1)
- Granularity of TT Technology TransferDocument3 pagesGranularity of TT Technology Transfer121815102042 gitamNo ratings yet
- Lab Activity #8Document3 pagesLab Activity #8Kristelito Grace MarinoNo ratings yet
- Sedative Hypnotic Drugs - ArfDocument69 pagesSedative Hypnotic Drugs - Arfaditia1984No ratings yet
- Stok Obat pra-ED April 2023-Maret 2024Document14 pagesStok Obat pra-ED April 2023-Maret 2024Nada Arum WardhaniNo ratings yet
- Biopharmaceutics Modelling As A Fundamental Tool To Support Accelerated AccessDocument20 pagesBiopharmaceutics Modelling As A Fundamental Tool To Support Accelerated AccessMaria Rey RicoNo ratings yet
- Healthcare: Dow Corning Q7-2587, 30% Simethicone Emulsion USPDocument2 pagesHealthcare: Dow Corning Q7-2587, 30% Simethicone Emulsion USPSari RofiqohNo ratings yet
- Pharmaceutical Packaging & Storage ConditionDocument42 pagesPharmaceutical Packaging & Storage ConditionEph Rem100% (1)
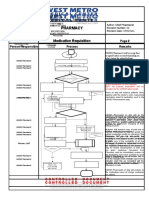
- Pharmacy Pharmacy: Medication Requisition Medication RequisitionDocument1 pagePharmacy Pharmacy: Medication Requisition Medication RequisitionSharie Grace ImlanNo ratings yet
- On Cleaning Validation Recovery Studies: Common MisconceptionsDocument9 pagesOn Cleaning Validation Recovery Studies: Common MisconceptionsMiguel Angel Pacahuala CristobalNo ratings yet
- Pharmaceutical Defects: A Critical Review On Defects of Various Dosage Forms and Regulatory ImpactsDocument5 pagesPharmaceutical Defects: A Critical Review On Defects of Various Dosage Forms and Regulatory ImpactsPrasannaNo ratings yet
- Set Khitan 26 Jan 23Document1 pageSet Khitan 26 Jan 23abu_abdisysyaakirNo ratings yet
- Dossier Format Generic Prescriptions MedicineDocument3 pagesDossier Format Generic Prescriptions MedicineChaNo ratings yet
- Pricelist OGB Phapros PKP 2020Document6 pagesPricelist OGB Phapros PKP 2020Farmasi beltimNo ratings yet
- Unnati Garg (ICH Guidelines)Document66 pagesUnnati Garg (ICH Guidelines)Unnati GargNo ratings yet
- IM InjectionsDocument3 pagesIM InjectionsZafar MahmoodNo ratings yet
- PDP 406 Clinical Toxicology: Pharm.D Fourth YearDocument18 pagesPDP 406 Clinical Toxicology: Pharm.D Fourth Yearabirami pNo ratings yet
- Hospital Formulary ADocument13 pagesHospital Formulary Alesliemaebarlaan03No ratings yet
- ADR & IncompatibilitiesDocument14 pagesADR & IncompatibilitiesKate EvangelistaNo ratings yet
- Drug Formulary 2219844Document1,224 pagesDrug Formulary 2219844gszzq8cj4mNo ratings yet
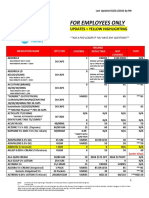
- Employee Only Pricing Sheet 02.11.22Document10 pagesEmployee Only Pricing Sheet 02.11.22rickyNo ratings yet
- Ciavarella 2016Document12 pagesCiavarella 2016mukesh choudharyNo ratings yet
- Kinase InhibitorDocument85 pagesKinase InhibitorSowjanya NekuriNo ratings yet
- Impo Bio KineticsDocument23 pagesImpo Bio Kineticshamam salih badriNo ratings yet
- Obat Prekursor Dan OOTDocument7 pagesObat Prekursor Dan OOTAbdul kadir100% (1)
- Drug Delivery SystemsDocument57 pagesDrug Delivery SystemsGagan Kumar JanghelNo ratings yet
- SOP For In-Process Sampling and Analysis of Oral Drug ProductsDocument9 pagesSOP For In-Process Sampling and Analysis of Oral Drug ProductsMubarak PatelNo ratings yet
- RALTEGRAVIRDocument11 pagesRALTEGRAVIRDeepti AtluriNo ratings yet
- Lecture 2 PharmacologyDocument27 pagesLecture 2 Pharmacologyalifa982941No ratings yet
- Adverse Eeffects of Drugs and Their Management in PaediatricsDocument6 pagesAdverse Eeffects of Drugs and Their Management in PaediatricsRinchin ChhotenNo ratings yet