Download as pdf or txt
You might also like
- Graber - Orthodontics Current Principles and Techniques 5th EditionDocument1,072 pagesGraber - Orthodontics Current Principles and Techniques 5th Editionortodoncia 201880% (44)
- Biological Consideration in Mandibular Impression ProceduresDocument41 pagesBiological Consideration in Mandibular Impression ProceduresSaravanan Thangarajan67% (3)
- Laboratory Procedure Prescription: Margin DesignDocument1 pageLaboratory Procedure Prescription: Margin Designdrmohamad drmohamadNo ratings yet
- Az 1575Document41 pagesAz 1575Arleig Augusto de MatosNo ratings yet
- 4Document1 page4alnoel tordillaNo ratings yet
- Scheda MDS02 PDFDocument1 pageScheda MDS02 PDFThomas RiatoNo ratings yet
- Affri enDocument56 pagesAffri enDeepak KumarNo ratings yet
- New Periodic TableDocument1 pageNew Periodic Tableharpal_abhNo ratings yet
- 5322-01-01 - Rigla 1Document1 page5322-01-01 - Rigla 1CezzarinoNo ratings yet
- Poligonal 20 - A3Document1 pagePoligonal 20 - A3ABDIASmamanigallegosNo ratings yet
- Elevation Isometric View: Section Aa'Document2 pagesElevation Isometric View: Section Aa'44 khushi DhuriNo ratings yet
- Relative Material HardnessDocument1 pageRelative Material HardnessrizkiNo ratings yet
- Project 1 - 57 Jean Street, Seven Hills - Site SurveyDocument1 pageProject 1 - 57 Jean Street, Seven Hills - Site SurveyAlbert LiuNo ratings yet
- A340 Parker GasketsDocument6 pagesA340 Parker GasketsjckfNo ratings yet
- Denah Lantai 1 - Gedung Fis Um: Shaft Shaft Lift Barang Shaft Shaft Lift BarangDocument1 pageDenah Lantai 1 - Gedung Fis Um: Shaft Shaft Lift Barang Shaft Shaft Lift BarangRegi WahyuNo ratings yet
- R1 Donor Cut Tower: Waste Hexane Drum Item No. D-718Document1 pageR1 Donor Cut Tower: Waste Hexane Drum Item No. D-718NoppolNorasriNo ratings yet
- Denah Lantai Basement & 1Document1 pageDenah Lantai Basement & 1Ivan GeovaniNo ratings yet
- Group Housing: North Pooja Yadav Ar. Manish GuptaDocument1 pageGroup Housing: North Pooja Yadav Ar. Manish GuptavijetaNo ratings yet
- Rhcaeta: Structural Design Calculation Sheet For Block of Duplex FOR MR & Mrs Adokiye Precious CharlesDocument17 pagesRhcaeta: Structural Design Calculation Sheet For Block of Duplex FOR MR & Mrs Adokiye Precious CharlesEze NonsoNo ratings yet
- 364+650 Proposed PlanDocument3 pages364+650 Proposed PlanVivek G. AbhyankarNo ratings yet
- Sdp-si Gear CatalogueDocument166 pagesSdp-si Gear CataloguedanduerangoNo ratings yet
- Rebar Physical PropertiesDocument2 pagesRebar Physical PropertiesJuan RodriguezNo ratings yet
- Gold Note: 30 October 2007Document10 pagesGold Note: 30 October 2007anamq1No ratings yet
- Lever Style Plungers Locking Non Locking Stainless SteelDocument3 pagesLever Style Plungers Locking Non Locking Stainless SteelPedro CaraveoNo ratings yet
- Residência - Fernanda de Lima Sobreiro: FURO R100Document1 pageResidência - Fernanda de Lima Sobreiro: FURO R100MARIONo ratings yet
- Furnace Coil DrawingDocument1 pageFurnace Coil DrawingpurNo ratings yet
- EV-Disc BR PADS-2132K PDFDocument1 pageEV-Disc BR PADS-2132K PDFSpeedyGonsalesNo ratings yet
- Worm IntroductionDocument4 pagesWorm IntroductionRoby MastreNo ratings yet
- Saxophone enDocument2 pagesSaxophone enccbplaysmusicNo ratings yet
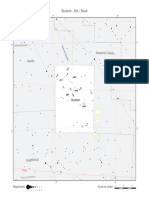
- Scutum - SCT - Scuti: Serpens Cauda AquilaDocument1 pageScutum - SCT - Scuti: Serpens Cauda Aquilaefrain dalmagroNo ratings yet
- P1359 SWA S001 - Rev4Document1 pageP1359 SWA S001 - Rev4geethsanNo ratings yet
- Steinel Springs CatalogDocument49 pagesSteinel Springs CatalogRafael Zavaleta AhonNo ratings yet
- Soldering Plating Stonesetting ENDocument16 pagesSoldering Plating Stonesetting ENAsia MarinoNo ratings yet
- SSV18 TrailMap Standish 1.0 WebsiteDocument1 pageSSV18 TrailMap Standish 1.0 Websiteahoussian14No ratings yet
- SBSG Rwy-12-30 Vac 20221201Document2 pagesSBSG Rwy-12-30 Vac 20221201Fernando CarmelNo ratings yet
- Khushi Dhuri Special Skills Workshop 2000701044Document3 pagesKhushi Dhuri Special Skills Workshop 200070104444 khushi DhuriNo ratings yet
- Iervolino Et Al BEE Central ItalyDocument19 pagesIervolino Et Al BEE Central ItalyEdgardo DavidiNo ratings yet
- Orifice Plate With Carrier Ring Assembly PDFDocument1 pageOrifice Plate With Carrier Ring Assembly PDFaravindNo ratings yet
- Orifice Plate With Carrier Ring Assembly PDFDocument1 pageOrifice Plate With Carrier Ring Assembly PDFRajeev ChaudNo ratings yet
- 2 Kiks-ModelDocument1 page2 Kiks-ModelAndeNo ratings yet
- Khoidaudam 2Document1 pageKhoidaudam 2tai taiNo ratings yet
- Sadar Bazar Tdi City, Sector-117, Mohali: Sector Dividing Road 200'-0" Wide RoadDocument1 pageSadar Bazar Tdi City, Sector-117, Mohali: Sector Dividing Road 200'-0" Wide Roadmanit SangwanNo ratings yet
- Precision Diffraction Slits Manual OS 8453Document3 pagesPrecision Diffraction Slits Manual OS 8453Brenda CruzNo ratings yet
- Ann Whs ElevationsDocument1 pageAnn Whs Elevationssimbwa2016No ratings yet
- Material P-Number - Chai (Rev3)Document3 pagesMaterial P-Number - Chai (Rev3)Chaitanya Sai TNo ratings yet
- Steel Racks Steel Racks With Machined Ends: Recommended Mating PinionsDocument1 pageSteel Racks Steel Racks With Machined Ends: Recommended Mating Pinionsindro wibowoNo ratings yet
- Citymap - Textured - Modified Copy03Document1 pageCitymap - Textured - Modified Copy03GabrielNo ratings yet
- Station Connector Height RevisionDocument1 pageStation Connector Height RevisionQazi NoorNo ratings yet
- Autocad Sample WorkDocument1 pageAutocad Sample WorkrobinNo ratings yet
- TPE 2 RaoulDocument1 pageTPE 2 RaoulRaoul officielNo ratings yet
- Do Not Scale: DescriptionDocument6 pagesDo Not Scale: DescriptionPalyyNo ratings yet
- Holtzblatt PDFDocument94 pagesHoltzblatt PDFVictor Manuel PeñeñoryNo ratings yet
- Casebook: EditionDocument30 pagesCasebook: EditionNaura TsabitaNo ratings yet
- Winter MTB Tour/ BMX Otjiwarongo Winter MTB Tour/ BMX OtjiwarongoDocument2 pagesWinter MTB Tour/ BMX Otjiwarongo Winter MTB Tour/ BMX Otjiwarongojohanita de waalNo ratings yet
- Pilar Lantai 4 de Vasa ExtentionDocument2 pagesPilar Lantai 4 de Vasa ExtentionLIFE STONENo ratings yet
- Schwarzkopf Mar Apr 2014 PromosDocument24 pagesSchwarzkopf Mar Apr 2014 PromosVansh LuthrraNo ratings yet
- GudangDocument1 pageGudangAji PrayogaNo ratings yet
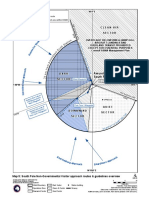
- Map5 SouthPole ASMA v10Document1 pageMap5 SouthPole ASMA v10Ricardo Salinas FournierNo ratings yet
- RAMBU K3-Model-2 PDFDocument1 pageRAMBU K3-Model-2 PDFmuhamad ilham fachrudinNo ratings yet
- Flashforge Filament Guides: Shop All FilamentsDocument1 pageFlashforge Filament Guides: Shop All FilamentsPedro DiasNo ratings yet
- 00 Ball Float Full WebDocument9 pages00 Ball Float Full WebWagner LimaNo ratings yet
- The Rough Guide to Beijing (Travel Guide eBook)From EverandThe Rough Guide to Beijing (Travel Guide eBook)Rating: 2 out of 5 stars2/5 (1)
- RadioDocument9 pagesRadioMohammed JabrNo ratings yet
- School Health Examination Card: Republic of The Philippines Department of EducationDocument4 pagesSchool Health Examination Card: Republic of The Philippines Department of EducationNEIL DUGAYNo ratings yet
- PG Case History Proforma MODIFIEDDocument11 pagesPG Case History Proforma MODIFIEDSahin mollickNo ratings yet
- 5 Klasisifikasi ECCDocument3 pages5 Klasisifikasi ECCSusi AbidinNo ratings yet
- Considerations and Concepts of Case Selection in The Mangement of Post Treatment Endo. DiseaseDocument25 pagesConsiderations and Concepts of Case Selection in The Mangement of Post Treatment Endo. DiseaseWatinee WanichwetinNo ratings yet
- 82984-Article Text-200031-1-10-20121112Document3 pages82984-Article Text-200031-1-10-20121112Yusuf DiansyahNo ratings yet
- Burkets Oral Medicine Diagnosis and TreatmentDocument3 pagesBurkets Oral Medicine Diagnosis and Treatmentgrishmabaral1No ratings yet
- Root Resorption: DR Brijesh Kumar Singh MDS 2018-21Document37 pagesRoot Resorption: DR Brijesh Kumar Singh MDS 2018-21Brijesh Kumar Singh100% (1)
- Dentsply Rinn CatalogDocument31 pagesDentsply Rinn CatalogudirmusaNo ratings yet
- DIAGNOSISDocument274 pagesDIAGNOSISArun ThakurNo ratings yet
- Anatomy Orofacial Structures 8th Brand Test BankDocument14 pagesAnatomy Orofacial Structures 8th Brand Test BankfahedqNo ratings yet
- Luki Gummetal W Ortodoncji 0Document16 pagesLuki Gummetal W Ortodoncji 0Zhiao Liu100% (1)
- Esthetic Considerations in Interdental Papilla PDFDocument11 pagesEsthetic Considerations in Interdental Papilla PDFXavier AltamiranoNo ratings yet
- Basic Guide To Dental Procedures - (Glossary of Terms)Document4 pagesBasic Guide To Dental Procedures - (Glossary of Terms)ofentsemphotlharipeNo ratings yet
- 14 Kelly 1977 Centric Relation, Centric Occlusion, and Posterior Tooth Forms and ArrangementDocument7 pages14 Kelly 1977 Centric Relation, Centric Occlusion, and Posterior Tooth Forms and Arrangementjorefe12No ratings yet
- Medically Compromised PatientDocument109 pagesMedically Compromised PatientShubham khandkeNo ratings yet
- IPS+Style+Ceram IndiaDocument86 pagesIPS+Style+Ceram IndiaAllen SharonNo ratings yet
- Biomimetic Materials in Pediatric Dentistry: From Past To FutureDocument6 pagesBiomimetic Materials in Pediatric Dentistry: From Past To FutureIJAR JOURNALNo ratings yet
- Cure Tooth Decay: Remineralize Cavities and Repair Your Teeth Naturally With Good Food - Ramiel NagelDocument5 pagesCure Tooth Decay: Remineralize Cavities and Repair Your Teeth Naturally With Good Food - Ramiel Nagelborunuti100% (1)
- Int Endodontic J - 2022 - Chevalier - Preclinical 3D Printed Laboratory Simulation of Deep Caries and The Exposed PulpDocument14 pagesInt Endodontic J - 2022 - Chevalier - Preclinical 3D Printed Laboratory Simulation of Deep Caries and The Exposed PulpAnuj BhardwajNo ratings yet
- Maxillofacial Rehabilitation Prosthodontic and SurDocument4 pagesMaxillofacial Rehabilitation Prosthodontic and SurAnuragNo ratings yet
- Evaluation - of - Microleakage - of - Stainless - Steel.94 (CA)Document4 pagesEvaluation - of - Microleakage - of - Stainless - Steel.94 (CA)renabodeNo ratings yet
- Principles of The Alexander DisciplineDocument5 pagesPrinciples of The Alexander DisciplineSarah Fauzia SiregarNo ratings yet
- Three-Dimensional Evaluation of Dentofacial Transverse Widths in Adults With Different Sagittal Facial Patterns PDFDocument10 pagesThree-Dimensional Evaluation of Dentofacial Transverse Widths in Adults With Different Sagittal Facial Patterns PDFSoe San KyawNo ratings yet
- Third Stage Begg MechanotherapyDocument32 pagesThird Stage Begg MechanotherapyNaziya ShaikNo ratings yet
- K. DamonAbstractsVol1Document17 pagesK. DamonAbstractsVol1correoandroideNo ratings yet
- Ethics in DentistryDocument45 pagesEthics in DentistryMaryam KardoustNo ratings yet
- The Dung Ages - AnalysisDocument1 pageThe Dung Ages - AnalysisSophia FletcherNo ratings yet