Download as pdf or txt
You might also like
- Income Calculation WorksheetDocument1 pageIncome Calculation Worksheetrush2serveNo ratings yet
- Certificate of Agreement For Coverage of Student LoanDocument4 pagesCertificate of Agreement For Coverage of Student LoanJohn BaileyNo ratings yet
- Other Percentage TaxDocument3 pagesOther Percentage TaxHafi DisoNo ratings yet
- N202669852876 Template012 131071016 09 22 2020 05 19 17 ENDocument8 pagesN202669852876 Template012 131071016 09 22 2020 05 19 17 ENmaraki2012No ratings yet
- EligibilityResultsNotice 4Document11 pagesEligibilityResultsNotice 4Jeremy L. BellerNo ratings yet
- 1010EZ FillableDocument5 pages1010EZ FillableFilozófus ÖnjelöltNo ratings yet
- 2015 Uc Health FaaDocument4 pages2015 Uc Health Faaapi-263913260No ratings yet
- Mission Charity Care Response April 30, 2020Document54 pagesMission Charity Care Response April 30, 2020Jennifer EmertNo ratings yet
- EligibilityResultsNotice 4Document12 pagesEligibilityResultsNotice 4Jessica StreitNo ratings yet
- Your 2024 Social Security Cost of Living IncreaseDocument4 pagesYour 2024 Social Security Cost of Living IncreaseABUDUAOA KOOA9WNo ratings yet
- Pparx ApplicationsDocument8 pagesPparx ApplicationsJames MullinsNo ratings yet
- Amerita Vision PlanDocument41 pagesAmerita Vision Planbutt7474No ratings yet
- Vha 10 10ezr FillDocument4 pagesVha 10 10ezr Fillcicin8190No ratings yet
- State ManualDocument31 pagesState ManualKEILYBNo ratings yet
- Lillycares Application PDFDocument3 pagesLillycares Application PDFRuben TorresNo ratings yet
- Kimberly Sullivan, SVP Chief Revenue Cycle Officer Vicki Head, Dir Patient AccessDocument6 pagesKimberly Sullivan, SVP Chief Revenue Cycle Officer Vicki Head, Dir Patient AccessDan SmithNo ratings yet
- May 30 Provider Relief Fund FAQ RedlineDocument23 pagesMay 30 Provider Relief Fund FAQ RedlineRachel Cohrs100% (1)
- Terms Conditions Provider Relief 20 BDocument11 pagesTerms Conditions Provider Relief 20 BRanal QurbanovNo ratings yet
- Claim FormDocument3 pagesClaim FormInvestor ProtegeNo ratings yet
- Eligibility Results NoticeDocument12 pagesEligibility Results NoticeDesign to BlessNo ratings yet
- Assurant Health Access: in Force Underwriting Change PacketDocument10 pagesAssurant Health Access: in Force Underwriting Change PacketSwisskelly1No ratings yet
- Eligibility NoticeDocument17 pagesEligibility NoticeFlintston3No ratings yet
- General ForbearanceDocument2 pagesGeneral Forbearancemyedaccount.orgNo ratings yet
- Your 2024 Social Security Cost of Living IncreaseDocument4 pagesYour 2024 Social Security Cost of Living IncreasenazoyaqNo ratings yet
- Terms Conditions Phase 2 General Distribution Relief FundDocument10 pagesTerms Conditions Phase 2 General Distribution Relief FundRanal Qurbanov100% (1)
- Week 7 Chapter 15Document27 pagesWeek 7 Chapter 15Ogweno OgwenoNo ratings yet
- Eligibility Results NoticeDocument12 pagesEligibility Results NoticeDaBaddest ManagementNo ratings yet
- Colorado Application For Public Assistance (English)Document16 pagesColorado Application For Public Assistance (English)OSCAR SPENCER RAMIREZNo ratings yet
- Assignment of Benefits MedicareDocument6 pagesAssignment of Benefits Medicarepmojoumpd100% (1)
- Eligibility Results NoticeDocument11 pagesEligibility Results NoticeAlex LawroskyNo ratings yet
- Print ApplicationDocument7 pagesPrint ApplicationHarris HoneycuttNo ratings yet
- Consumer Health Insurance Appeal Denied ClaimsDocument4 pagesConsumer Health Insurance Appeal Denied Claimssahapdeen haiderNo ratings yet
- Terms Conditions Phase 4 General Distribution Relief FundDocument10 pagesTerms Conditions Phase 4 General Distribution Relief FundRanal QurbanovNo ratings yet
- 2015 EligibilityNotice SasDocument18 pages2015 EligibilityNotice SasSharif M Mizanur RahmanNo ratings yet
- EligibilityResultsNotice 5Document7 pagesEligibilityResultsNotice 5Larisa AbrahamyanNo ratings yet
- InternationalDocument14 pagesInternationalAston Martin DollaNo ratings yet
- File 01944773Document5 pagesFile 01944773kieramatherlyNo ratings yet
- Order_2617136_Adverse_20240103162103Document7 pagesOrder_2617136_Adverse_20240103162103bkeller0627No ratings yet
- Eligibility NoticeDocument17 pagesEligibility NoticeDJPhrostNo ratings yet
- Eligibility Notice: You May Be Eligible For Free or Low-Cost Coverage Through Medicaid or The Children's Health Insurance Program (CHIP)Document10 pagesEligibility Notice: You May Be Eligible For Free or Low-Cost Coverage Through Medicaid or The Children's Health Insurance Program (CHIP)Jun ChewningNo ratings yet
- Disability Advisory Council BookletDocument36 pagesDisability Advisory Council BookletBernewsAdminNo ratings yet
- Eligibility Results NoticeDocument11 pagesEligibility Results NoticeWilliam PeeleNo ratings yet
- Eligibility Results NoticeDocument7 pagesEligibility Results NoticeDorie WoodwardNo ratings yet
- Your Eligibility Results: Department of Health and Human Services 465 Industrial Boulevard London, Kentucky 40750-0001Document16 pagesYour Eligibility Results: Department of Health and Human Services 465 Industrial Boulevard London, Kentucky 40750-0001John SpiersNo ratings yet
- EligibilityResultsNotice PDFDocument10 pagesEligibilityResultsNotice PDFtoluNo ratings yet
- 6065 Hca DL Ip1 Gen PKT PDFDocument17 pages6065 Hca DL Ip1 Gen PKT PDFAlayssia CanoraNo ratings yet
- Cliff Notes - PM UW Policy IssueDocument4 pagesCliff Notes - PM UW Policy IssueJohnathan JohnsonNo ratings yet
- Lincoln Financial Authorization To Release InformationDocument1 pageLincoln Financial Authorization To Release InformationSDNo ratings yet
- EligibilityResultsNotice 5Document10 pagesEligibilityResultsNotice 5Smit PatelNo ratings yet
- FS PrivateInsuranceDocument2 pagesFS PrivateInsuranceIndiana Family to FamilyNo ratings yet
- Aetna Hmo 20 GeorgiaDocument94 pagesAetna Hmo 20 Georgiabill_w85081No ratings yet
- DescriptionOfCoverage StudyUSADocument26 pagesDescriptionOfCoverage StudyUSAHungNo ratings yet
- Health Insurance FAQ From IntrawestDocument9 pagesHealth Insurance FAQ From IntrawestScott FranzNo ratings yet
- 2012 EnrollApp CA KPIF Charlotte Ikner LCKDocument24 pages2012 EnrollApp CA KPIF Charlotte Ikner LCKcharanmann9165No ratings yet
- WPS-217317406 613letDocument5 pagesWPS-217317406 613letfjpz6vfqktNo ratings yet
- FWA Provider Training - Oct 2019Document23 pagesFWA Provider Training - Oct 2019Anushree PawanrajNo ratings yet
- Instructions For Completing Enrollment Application For Health BenefitsDocument5 pagesInstructions For Completing Enrollment Application For Health BenefitsDonna Mae RafolNo ratings yet
- Eligibility Results NoticeDocument12 pagesEligibility Results NoticeLagannNo ratings yet
- Maness Adverse Action Letter - PDF - PDF ExpertDocument6 pagesManess Adverse Action Letter - PDF - PDF Expertjeremy.manessNo ratings yet
- How To File Your Own Bankruptcy: The Step-by-Step Handbook to Filing Your Own Bankruptcy PetitionFrom EverandHow To File Your Own Bankruptcy: The Step-by-Step Handbook to Filing Your Own Bankruptcy PetitionNo ratings yet
- Health Care Reform Act: Critical Tax and Insurance RamificationsFrom EverandHealth Care Reform Act: Critical Tax and Insurance RamificationsNo ratings yet
- Social Security / Medicare Handbook for Federal Employees and Retirees: All-New 4th EditionFrom EverandSocial Security / Medicare Handbook for Federal Employees and Retirees: All-New 4th EditionNo ratings yet
- Chapter 12Document38 pagesChapter 12Nguyễn Vinh QuangNo ratings yet
- Iesco Online BillDocument2 pagesIesco Online BillHORAIRA ABBASINo ratings yet
- An Analysis of Philippine Income TaxationDocument14 pagesAn Analysis of Philippine Income TaxationCrizedhen VardeleonNo ratings yet
- Public Finance BBA 6th SyllabusDocument2 pagesPublic Finance BBA 6th SyllabusPrashant Raj NeupaneNo ratings yet
- Payslip March 2021Document2 pagesPayslip March 2021Aravind SammandhamNo ratings yet
- Discount SGST CGST Round Off: Buyer (Bill To)Document1 pageDiscount SGST CGST Round Off: Buyer (Bill To)Dwivedi ShubhamNo ratings yet
- Test Bank For South Western Federal Taxation 2021 Individual Income Taxes 44th Edition James C Young Annette Nellen William A Raabe William H Hoffman JR David M Maloney 2Document37 pagesTest Bank For South Western Federal Taxation 2021 Individual Income Taxes 44th Edition James C Young Annette Nellen William A Raabe William H Hoffman JR David M Maloney 2sierraenarmedgj2n100% (35)
- Pbcom vs. CirDocument2 pagesPbcom vs. CirCaroline A. LegaspinoNo ratings yet
- DineroDocument4 pagesDineroValeria Amaya Burgos0% (1)
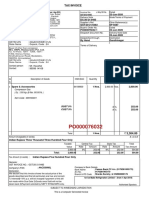
- Tax Invoice: Product Description Qty Gross A Mount Discount Taxable V Alue Igst TotalDocument3 pagesTax Invoice: Product Description Qty Gross A Mount Discount Taxable V Alue Igst TotalANIL KUMARNo ratings yet
- Instructional Materials For Income TaxationDocument126 pagesInstructional Materials For Income TaxationNadi HoodNo ratings yet
- Tax Invoice: Ice Make Refrigeration Limited - (From 1-Apr-2019)Document1 pageTax Invoice: Ice Make Refrigeration Limited - (From 1-Apr-2019)Sunil PatelNo ratings yet
- Accounting For Income TaxDocument6 pagesAccounting For Income TaxKakay EspirituNo ratings yet
- ACCT5942 Week4 PresentationDocument13 pagesACCT5942 Week4 PresentationDuongPhamNo ratings yet
- Quizzer - PREFINALDocument19 pagesQuizzer - PREFINALrav dano50% (2)
- Tax Invoice: Page 1 of 2Document2 pagesTax Invoice: Page 1 of 2Kemala AndrianiNo ratings yet
- Dr. Shannu Narayan PGP - Fintax Batch Session 3Document18 pagesDr. Shannu Narayan PGP - Fintax Batch Session 3ayman abdul salamNo ratings yet
- Payroll DetailDocument7 pagesPayroll Detailnileshbj.taskseverydayNo ratings yet
- Practice Questions Residential Status 1Document2 pagesPractice Questions Residential Status 1Varsha .kNo ratings yet
- Comparative Statement of Profit and LossDocument6 pagesComparative Statement of Profit and LossHimanshi ChopraNo ratings yet
- Assignment #12Document3 pagesAssignment #12Soleil AsierNo ratings yet
- Tutorial 3: Employment and Personal Taxation: Universiti Tunku Abdul Rahman Faculty of Business and FinanceDocument2 pagesTutorial 3: Employment and Personal Taxation: Universiti Tunku Abdul Rahman Faculty of Business and FinanceKAY PHINE NGNo ratings yet
- Tutorial 2 (3) 3 (E)Document2 pagesTutorial 2 (3) 3 (E)Shan JeefNo ratings yet
- Tax Invoice - Ezcash: Transaction DetailsDocument1 pageTax Invoice - Ezcash: Transaction Detailsmominacolano30No ratings yet
- Provincial Tuition and Education Amounts: Schedule ON (S11)Document1 pageProvincial Tuition and Education Amounts: Schedule ON (S11)api-3836185No ratings yet
- BIR Updates Issue No. 2Document2 pagesBIR Updates Issue No. 2Jy GoNo ratings yet
- Pay Stub (1) - 11.30.2022Document1 pagePay Stub (1) - 11.30.2022துவேந்தர் சண்முகம்No ratings yet
- Chapter 5Document5 pagesChapter 5Kristine Jhoy Nolasco SecopitoNo ratings yet