Download as pdf or txt
You might also like
- Advanced Fitness Assessment and Exercise Prescription 8th Edition Ebook PDF VersionDocument62 pagesAdvanced Fitness Assessment and Exercise Prescription 8th Edition Ebook PDF Versionalan.lewis48994% (65)
- Advanced Fitness Assessment and Exercise Prescription 8th Edition Ebook PDF VersionDocument62 pagesAdvanced Fitness Assessment and Exercise Prescription 8th Edition Ebook PDF Versionalan.lewis48994% (65)
- Advanced Emt A Clinical Reasoning Approach 2nd Edition Ebook PDFDocument61 pagesAdvanced Emt A Clinical Reasoning Approach 2nd Edition Ebook PDFalan.lewis48996% (46)
- Advanced Emt A Clinical Reasoning Approach 2nd Edition Ebook PDFDocument61 pagesAdvanced Emt A Clinical Reasoning Approach 2nd Edition Ebook PDFalan.lewis48996% (46)
- Materi MPPC XXXDocument22 pagesMateri MPPC XXXEther Manuputty II100% (6)
- Comptia Project Pk0 005 Cert Guide 2Nd Edition Robin Abernathy Ann Lang Full ChapterDocument67 pagesComptia Project Pk0 005 Cert Guide 2Nd Edition Robin Abernathy Ann Lang Full Chapterlatasha.delvalle550100% (5)
- Lobola Bridewealth in Contemporary Southern Africa Implications For Gender Equality 1St Ed 2021 Edition Lovemore Togarasei Editor Full ChapterDocument68 pagesLobola Bridewealth in Contemporary Southern Africa Implications For Gender Equality 1St Ed 2021 Edition Lovemore Togarasei Editor Full Chapterdiane.jurado739100% (8)
- Comptia Security All in One Exam Guide Exam Sy0 501 5Th Edition WM Arthur Conklin Full ChapterDocument67 pagesComptia Security All in One Exam Guide Exam Sy0 501 5Th Edition WM Arthur Conklin Full Chapterlatasha.delvalle550100% (8)
- Treasures GR 3 Unit 4 6 Mcgraw Hill Mcgraw Hill All ChapterDocument67 pagesTreasures GR 3 Unit 4 6 Mcgraw Hill Mcgraw Hill All Chapterfelipe.canada376100% (7)
- Local Integration of Migrants Policy European Experiences and Challenges Jochen Franzke Full ChapterDocument67 pagesLocal Integration of Migrants Policy European Experiences and Challenges Jochen Franzke Full Chapterdiane.jurado739100% (4)
- The Bible in History How The Texts Have Shaped The Times 2Nd Edition David W Kling Full ChapterDocument67 pagesThe Bible in History How The Texts Have Shaped The Times 2Nd Edition David W Kling Full Chapterronnie.otero744100% (5)
- Local Invisibility Postcolonial Feminisms 1St Ed Edition Laura Fantone Full ChapterDocument67 pagesLocal Invisibility Postcolonial Feminisms 1St Ed Edition Laura Fantone Full Chapterdiane.jurado739100% (6)
- Lobstah Gahden Speak Out Against Pollution With A Wicked Awesome Boston Accent Alli Brydon Full ChapterDocument65 pagesLobstah Gahden Speak Out Against Pollution With A Wicked Awesome Boston Accent Alli Brydon Full Chapterdiane.jurado739100% (8)
- Tree Diversity Effects On Leaf Insect Damage On Pedunculate Oak - The Role of Landscape Context and Forest Stratum Bastien Castagneyrol Brice Giffard Elena Valdes Correcher Arndt Hampe All ChapterDocument31 pagesTree Diversity Effects On Leaf Insect Damage On Pedunculate Oak - The Role of Landscape Context and Forest Stratum Bastien Castagneyrol Brice Giffard Elena Valdes Correcher Arndt Hampe All Chapterfelipe.canada376100% (6)
- Treating Stalking A Practical Guide For Clinicians Troy Mcewan All ChapterDocument67 pagesTreating Stalking A Practical Guide For Clinicians Troy Mcewan All Chapterfelipe.canada376100% (6)
- Local Integration of Migrants Policy European Experiences and Challenges 1St Ed Edition Jochen Franzke Full ChapterDocument67 pagesLocal Integration of Migrants Policy European Experiences and Challenges 1St Ed Edition Jochen Franzke Full Chapterdiane.jurado739100% (7)
- Bilateral Cooperation and Human Trafficking: Eradicating Modern Slavery Between The United Kingdom and Nigeria 1st Edition May Ikeora (Auth.)Document68 pagesBilateral Cooperation and Human Trafficking: Eradicating Modern Slavery Between The United Kingdom and Nigeria 1st Edition May Ikeora (Auth.)ivan.jones400100% (7)
- Fundamentals of Risk Management Understanding Evaluating and Implementing Effective Risk Management 4th Edition Paul HopkinDocument54 pagesFundamentals of Risk Management Understanding Evaluating and Implementing Effective Risk Management 4th Edition Paul Hopkindiana.shelby469100% (13)
- The Bible in History David W Kling Full ChapterDocument67 pagesThe Bible in History David W Kling Full Chapterronnie.otero744100% (8)
- Full Chapter Atlas of Pediatric Brain Tumors 2Nd Edition Adekunle M Adesina PDFDocument53 pagesFull Chapter Atlas of Pediatric Brain Tumors 2Nd Edition Adekunle M Adesina PDFmichael.bones265100% (8)
- Solution Manual For Chemistry A Molecular Approach With Masteringchemistry 2Nd Edition by Tro Isbn 0321706153 9780321706157 Full Chapter PDFDocument36 pagesSolution Manual For Chemistry A Molecular Approach With Masteringchemistry 2Nd Edition by Tro Isbn 0321706153 9780321706157 Full Chapter PDFthomas.chatman911100% (13)
- Textbook Frontiers of Cyberlearning Emerging Technologies For Teaching and Learning J Michael Spector Ebook All Chapter PDFDocument53 pagesTextbook Frontiers of Cyberlearning Emerging Technologies For Teaching and Learning J Michael Spector Ebook All Chapter PDFmonica.bennett747100% (15)
- Organizational Behavior 12Th Edition Schermerhorn Solutions Manual PDFDocument25 pagesOrganizational Behavior 12Th Edition Schermerhorn Solutions Manual PDFruth.cave622100% (16)
- The Big Picture Gross Anatomy Medical Course Step 1 Review 2Nd Edition Edition David A Morton Full ChapterDocument67 pagesThe Big Picture Gross Anatomy Medical Course Step 1 Review 2Nd Edition Edition David A Morton Full Chapterronnie.otero744100% (8)
- PDF Identity Structure Analysis and Teacher Mentorship Across The Context of Schools and The Individual Graham Passmore Ebook Full ChapterDocument54 pagesPDF Identity Structure Analysis and Teacher Mentorship Across The Context of Schools and The Individual Graham Passmore Ebook Full Chaptertia.kempf329100% (2)
- Organizational Behavior 13Th Edition Bien Solutions Manual PDFDocument25 pagesOrganizational Behavior 13Th Edition Bien Solutions Manual PDFruth.cave622100% (16)
- The British General Election of 2019 Robert Ford Full Download ChapterDocument51 pagesThe British General Election of 2019 Robert Ford Full Download Chapterjohn.villanueva589100% (8)
- Textbook Fundamentals of Risk Management Fifth Edition Paul Hopkin Ebook All Chapter PDFDocument53 pagesTextbook Fundamentals of Risk Management Fifth Edition Paul Hopkin Ebook All Chapter PDFdiana.shelby469100% (14)
- Comptia Network Certification All in One Exam Guide Seventh Edition Exam N10 007 Meyers Full ChapterDocument77 pagesComptia Network Certification All in One Exam Guide Seventh Edition Exam N10 007 Meyers Full Chapterlatasha.delvalle550100% (8)
- Textbook Real World Decision Support Systems Case Studies 1St Edition Jason Papathanasiou Ebook All Chapter PDFDocument53 pagesTextbook Real World Decision Support Systems Case Studies 1St Edition Jason Papathanasiou Ebook All Chapter PDFhazel.sherlock724100% (5)
- PDF Joint Ownership in Eu Tunisia Relations Power and Negotiation Federica Zardo Ebook Full ChapterDocument53 pagesPDF Joint Ownership in Eu Tunisia Relations Power and Negotiation Federica Zardo Ebook Full Chaptermargo.martinez615100% (3)
- Creative Health For Pianists Concepts Exercises Compositions Pedro de Alcantara Full ChapterDocument67 pagesCreative Health For Pianists Concepts Exercises Compositions Pedro de Alcantara Full Chapterroman.nelson216100% (8)
- Household Gods The Religious Lives of The Adams Family Sara Georgini Full ChapterDocument67 pagesHousehold Gods The Religious Lives of The Adams Family Sara Georgini Full Chapterthelma.germany870100% (13)
- Inter and Post War Tourism in Western Europe 1916 1960 1St Ed Edition Carmelo Pellejero Martinez Full ChapterDocument51 pagesInter and Post War Tourism in Western Europe 1916 1960 1St Ed Edition Carmelo Pellejero Martinez Full Chaptercalvin.ponder874100% (6)
- Promoting Civic Health Through University Community Partnerships Global Contexts and Experiences 1St Ed 2020 Edition Thomas Andrew Bryer All ChapterDocument68 pagesPromoting Civic Health Through University Community Partnerships Global Contexts and Experiences 1St Ed 2020 Edition Thomas Andrew Bryer All Chapterrodolfo.wood436100% (6)
- Textbook Pedagogies For Internationalising Research Education Intellectual Equality Theoretic Linguistic Diversity and Knowledge Chuangxin 1St Edition Michael Singh Ebook All Chapter PDFDocument54 pagesTextbook Pedagogies For Internationalising Research Education Intellectual Equality Theoretic Linguistic Diversity and Knowledge Chuangxin 1St Edition Michael Singh Ebook All Chapter PDFnicholas.street673100% (7)
- Border Crossing and Comedy at The Theatre Italien 1716 1723 Transnational Theatre Histories 1St Ed 2021 Edition Mcmahan Download 2024 Full ChapterDocument48 pagesBorder Crossing and Comedy at The Theatre Italien 1716 1723 Transnational Theatre Histories 1St Ed 2021 Edition Mcmahan Download 2024 Full Chapterchristi.lewis617100% (11)
- Big Data and Public Policy Course Content and Outcome Rebecca Moody 2 Full ChapterDocument67 pagesBig Data and Public Policy Course Content and Outcome Rebecca Moody 2 Full Chapterruby.thornley305100% (5)
- Value Creation For Owners and Directors A Practical Guide On How To Lead Your Business Massimo Massa All ChapterDocument67 pagesValue Creation For Owners and Directors A Practical Guide On How To Lead Your Business Massimo Massa All Chaptermatthew.ferguson216100% (8)
- Textbook Thermal Power Plant Control and Instrumentation The Control of Boilers and Hrsgs 2Nd Edition David Lindsley Ebook All Chapter PDFDocument53 pagesTextbook Thermal Power Plant Control and Instrumentation The Control of Boilers and Hrsgs 2Nd Edition David Lindsley Ebook All Chapter PDFtim.bass844100% (5)
- Patricia Highsmith On Screen 1St Ed Edition Wieland Schwanebeck Full Chapter PDF ScribdDocument67 pagesPatricia Highsmith On Screen 1St Ed Edition Wieland Schwanebeck Full Chapter PDF Scribdwayne.garofalo759100% (8)
- Children and Young Peoples Participation in Child Protection International Research and Practical Applications Katrin Kriz Full ChapterDocument49 pagesChildren and Young Peoples Participation in Child Protection International Research and Practical Applications Katrin Kriz Full Chapterlouis.ballew766100% (10)
- Vernacular Politics in Northeast India Democracy Ethnicity and Indigeneity Jelle J P Wouters Ed Ebook Full ChapterDocument48 pagesVernacular Politics in Northeast India Democracy Ethnicity and Indigeneity Jelle J P Wouters Ed Ebook Full Chapterpeter.rivera411100% (7)
- Textbook Fundamentals of Hazardous Waste Site Remediation First Edition Sellers Ebook All Chapter PDFDocument47 pagesTextbook Fundamentals of Hazardous Waste Site Remediation First Edition Sellers Ebook All Chapter PDFtiffany.mcintyre649100% (12)
- Textbook Further Advances in Pragmatics and Philosophy Part 1 From Theory To Practice 1St Edition Alessandro Capone Ebook All Chapter PDFDocument53 pagesTextbook Further Advances in Pragmatics and Philosophy Part 1 From Theory To Practice 1St Edition Alessandro Capone Ebook All Chapter PDFdiana.shelby469100% (14)
- Trevor Winchester Swan Volume Ii Contributions To Economic Theory and Policy Peter L Swan All ChapterDocument47 pagesTrevor Winchester Swan Volume Ii Contributions To Economic Theory and Policy Peter L Swan All Chapterfelipe.canada376100% (9)
- PDF Ict Innovations 2019 Big Data Processing and Mining 11Th International Conference Ict Innovations 2019 Ohrid North Macedonia October 17 19 2019 Proceedings Sonja Gievska Ebook Full ChapterDocument54 pagesPDF Ict Innovations 2019 Big Data Processing and Mining 11Th International Conference Ict Innovations 2019 Ohrid North Macedonia October 17 19 2019 Proceedings Sonja Gievska Ebook Full Chaptertia.kempf329100% (2)
- Theory of Cryptography 16th International Conference TCC 2018 Panaji India November 11 14 2018 Proceedings Part I Amos BeimelDocument54 pagesTheory of Cryptography 16th International Conference TCC 2018 Panaji India November 11 14 2018 Proceedings Part I Amos Beimeltim.bass844100% (3)
- Full Ebook of Paul Tillich and Sino Christian Theology 1St Edition Jiafu Chen Online PDF All ChapterDocument69 pagesFull Ebook of Paul Tillich and Sino Christian Theology 1St Edition Jiafu Chen Online PDF All Chaptervijithrifi100% (4)
- Sovereignty and Event The Political in John D Caputos Radical Theology Calvin D Ullrich Full Download ChapterDocument51 pagesSovereignty and Event The Political in John D Caputos Radical Theology Calvin D Ullrich Full Download Chapteralexis.stoner527100% (6)
- Organizational Behavior 12Th Edition Schermerhorn Test Bank PDFDocument25 pagesOrganizational Behavior 12Th Edition Schermerhorn Test Bank PDFruth.cave622100% (16)
- Interpretation of Micromorphological Features of Soils and Regoliths 2Nd Edition Georges Stoops Full ChapterDocument51 pagesInterpretation of Micromorphological Features of Soils and Regoliths 2Nd Edition Georges Stoops Full Chapteralice.reynolds656100% (8)
- Age As Disease Anti Aging Technologies Sites and Practices 1St Edition David Jack Fletcher Full ChapterDocument51 pagesAge As Disease Anti Aging Technologies Sites and Practices 1St Edition David Jack Fletcher Full Chapterkenneth.milot991100% (12)
- (Download PDF) Architectural Graphic Standards Student Edition Keith E Hedges Editor in Chief Online Ebook All Chapter PDFDocument42 pages(Download PDF) Architectural Graphic Standards Student Edition Keith E Hedges Editor in Chief Online Ebook All Chapter PDFmarian.sortore151100% (9)
- PDF Identity Development in The Lifecourse A Semiotic Cultural Approach To Transitions in Early Adulthood Mariann Martsin Ebook Full ChapterDocument54 pagesPDF Identity Development in The Lifecourse A Semiotic Cultural Approach To Transitions in Early Adulthood Mariann Martsin Ebook Full Chaptertia.kempf329100% (2)
- Textbook Fundamentals of The Study of Urine and Body Fluids 1St Edition John W Ridley Ebook All Chapter PDFDocument53 pagesTextbook Fundamentals of The Study of Urine and Body Fluids 1St Edition John W Ridley Ebook All Chapter PDFdiana.shelby469100% (15)
- Covid 19 and International Political Theory Assessing The Potential For Normative Shift Ruairidh Brown Full ChapterDocument67 pagesCovid 19 and International Political Theory Assessing The Potential For Normative Shift Ruairidh Brown Full Chaptergloria.stiltner757100% (9)
- Australia in The Age of International Development 1945 1975 Colonial and Foreign Aid Policy in Papua New Guinea and Southeast Asia 1St Ed Edition Nicholas Ferns Full ChapterDocument52 pagesAustralia in The Age of International Development 1945 1975 Colonial and Foreign Aid Policy in Papua New Guinea and Southeast Asia 1St Ed Edition Nicholas Ferns Full Chaptermax.myers343100% (8)
- Out of The Fire A Military Sci Fi Series Out of The Earth Book 3 Jake Bible Full ChapterDocument57 pagesOut of The Fire A Military Sci Fi Series Out of The Earth Book 3 Jake Bible Full Chaptersandra.collier368100% (10)
- Strategic Management A Competitive Advantage Approach Concepts and Cases 14th Edition David Solutions Manual instant download all chapterDocument36 pagesStrategic Management A Competitive Advantage Approach Concepts and Cases 14th Edition David Solutions Manual instant download all chapterothmarmihay100% (3)
- Marina Carr Pastures of The Unknown 1St Ed Edition Melissa Sihra Full ChapterDocument67 pagesMarina Carr Pastures of The Unknown 1St Ed Edition Melissa Sihra Full Chapterzoe.boulton781100% (6)
- Textbook Portraits of Old Russia Imagined Lives of Ordinary People 1300 1725 1St Edition Donald G Ostrowski Ebook All Chapter PDFDocument42 pagesTextbook Portraits of Old Russia Imagined Lives of Ordinary People 1300 1725 1St Edition Donald G Ostrowski Ebook All Chapter PDFkenneth.nieves290100% (9)
- Lobotomy Nation: The History of Psychosurgery and Psychiatry in Denmark 1st Edition Jesper Vaczy Kragh full chapter instant downloadDocument45 pagesLobotomy Nation: The History of Psychosurgery and Psychiatry in Denmark 1st Edition Jesper Vaczy Kragh full chapter instant downloadranekgeilerNo ratings yet
- Lobotomy Nation The History of Psychosurgery and Psychiatry in Denmark 1St Edition Jesper Vaczy Kragh Full Chapter PDFDocument57 pagesLobotomy Nation The History of Psychosurgery and Psychiatry in Denmark 1St Edition Jesper Vaczy Kragh Full Chapter PDFinglezlusic100% (4)
- Dokumen - Tips Modern Trends in Hypnosis Springer 978-1-4684 4913 61pdf Modern Trends inDocument14 pagesDokumen - Tips Modern Trends in Hypnosis Springer 978-1-4684 4913 61pdf Modern Trends inHeyYouAreSmartNo ratings yet
- Local Invisibility Postcolonial Feminisms 1St Ed Edition Laura Fantone Full ChapterDocument67 pagesLocal Invisibility Postcolonial Feminisms 1St Ed Edition Laura Fantone Full Chapterdiane.jurado739100% (6)
- Lobstah Gahden Speak Out Against Pollution With A Wicked Awesome Boston Accent Alli Brydon Full ChapterDocument65 pagesLobstah Gahden Speak Out Against Pollution With A Wicked Awesome Boston Accent Alli Brydon Full Chapterdiane.jurado739100% (8)
- Lobola Bridewealth in Contemporary Southern Africa Implications For Gender Equality 1St Ed 2021 Edition Lovemore Togarasei Editor Full ChapterDocument68 pagesLobola Bridewealth in Contemporary Southern Africa Implications For Gender Equality 1St Ed 2021 Edition Lovemore Togarasei Editor Full Chapterdiane.jurado739100% (8)
- Local Integration of Migrants Policy European Experiences and Challenges Jochen Franzke Full ChapterDocument67 pagesLocal Integration of Migrants Policy European Experiences and Challenges Jochen Franzke Full Chapterdiane.jurado739100% (4)
- Local Integration of Migrants Policy European Experiences and Challenges 1St Ed Edition Jochen Franzke Full ChapterDocument67 pagesLocal Integration of Migrants Policy European Experiences and Challenges 1St Ed Edition Jochen Franzke Full Chapterdiane.jurado739100% (7)
- Advanced Accounting 6th EditionDocument61 pagesAdvanced Accounting 6th Editionmatthew.woodruff626100% (46)
- Advanced Health Assessment of Women Third Edition Clinical Skills and Procedures Advanced Health Assessment of Women Clinical Skills and Pro Ebook PDF VersionDocument62 pagesAdvanced Health Assessment of Women Third Edition Clinical Skills and Procedures Advanced Health Assessment of Women Clinical Skills and Pro Ebook PDF Versionalan.lewis489100% (44)
- Advanced Accounting 6th EditionDocument61 pagesAdvanced Accounting 6th Editionmatthew.woodruff626100% (46)
- Advanced Health Assessment of Women Third Edition Clinical Skills and Procedures Advanced Health Assessment of Women Clinical Skills and Pro Ebook PDF VersionDocument62 pagesAdvanced Health Assessment of Women Third Edition Clinical Skills and Procedures Advanced Health Assessment of Women Clinical Skills and Pro Ebook PDF Versionalan.lewis489100% (44)
- Activity 3 - GRPDocument4 pagesActivity 3 - GRPBianca BalmoresNo ratings yet
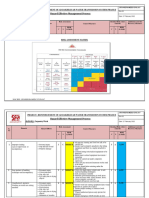
- Risk Assessment - Placing of Transformer - TTSDocument6 pagesRisk Assessment - Placing of Transformer - TTSnsadnan100% (2)
- ANCC NCPD ManualDocument58 pagesANCC NCPD Manualshadi alshadafanNo ratings yet
- Daycare Case ReportDocument45 pagesDaycare Case ReportApril ToweryNo ratings yet
- Learning Activity Sheet Quarter 2 - MELC 2: Discipline and Ideas in Applied Social SciencesDocument4 pagesLearning Activity Sheet Quarter 2 - MELC 2: Discipline and Ideas in Applied Social Sciencesgayle gallaza100% (1)
- 07 One Missing StrokeDocument10 pages07 One Missing StrokeMiura AngNo ratings yet
- HPV Amostras AlternativasDocument6 pagesHPV Amostras Alternativasnathaliasantosx3No ratings yet
- NSS - Ass 3 - 120ar0010Document3 pagesNSS - Ass 3 - 120ar0010Arpita SahooNo ratings yet
- PHD Thesis On Occupational StressDocument7 pagesPHD Thesis On Occupational Stresscindyturnertorrance100% (2)
- Swimmer Syndrome in WildlifeDocument2 pagesSwimmer Syndrome in WildlifeALicjaNo ratings yet
- Guidelines For Maternity Care 2016Document148 pagesGuidelines For Maternity Care 2016MjunjuNo ratings yet
- Jds Journal of Syiah Kuala Dentistry SocietyDocument5 pagesJds Journal of Syiah Kuala Dentistry SocietyDewa Ayu Kumara DewiNo ratings yet
- BLDG LAWS Pedro Assignment 7 RA9514Document16 pagesBLDG LAWS Pedro Assignment 7 RA9514Jofer PatenioNo ratings yet
- RISK ASSESSMENT - Carpentry WorkDocument6 pagesRISK ASSESSMENT - Carpentry WorkbalajiNo ratings yet
- Goals and Subgoals of The SurveyDocument18 pagesGoals and Subgoals of The SurveyUrja DhabardeNo ratings yet
- IMMUNIZATION (Health Education)Document33 pagesIMMUNIZATION (Health Education)Rozel Encarnacion100% (2)
- Opium: Retail and Wholesale Prices and Purity Levels: Breakdown by Drug, Region and Country or TerritoryDocument19 pagesOpium: Retail and Wholesale Prices and Purity Levels: Breakdown by Drug, Region and Country or TerritoryboombaNo ratings yet
- Lung Scan: Safuan Awang Nuclear MedicineDocument19 pagesLung Scan: Safuan Awang Nuclear MedicineVeraaaNo ratings yet
- Case History PresentationDocument64 pagesCase History PresentationNitin FatingNo ratings yet
- Research Paper - Negative Effects of Video Games On ChildrenDocument2 pagesResearch Paper - Negative Effects of Video Games On ChildrenNicole JimelgaNo ratings yet
- Topic 1.4 - User-Requirement and Perception of SpaceDocument8 pagesTopic 1.4 - User-Requirement and Perception of SpaceCarlo PascuaNo ratings yet
- New Era of Filipino Youth VolunteerismDocument11 pagesNew Era of Filipino Youth VolunteerismArvhie Santos100% (1)
- Reflection PaperDocument2 pagesReflection Paperapi-317274133No ratings yet
- Student Stress ChecklistDocument2 pagesStudent Stress ChecklistAlaiza Maas LanonNo ratings yet
- Safety Data Sheet: Section 1: Identification of The Substance/Mixture and of The Company/UndertakingDocument8 pagesSafety Data Sheet: Section 1: Identification of The Substance/Mixture and of The Company/UndertakingElizabeth Trejo MoralesNo ratings yet
- College Students Caffeine Intake Habitsand Their Perceptionof Its EffectsDocument11 pagesCollege Students Caffeine Intake Habitsand Their Perceptionof Its EffectsHannah TrishaNo ratings yet
- PB Mental Health Snapshot 4Document5 pagesPB Mental Health Snapshot 4amanda wuNo ratings yet
- ReseachDocument20 pagesReseachLila GrayNo ratings yet
- Editor Chefe,+32 38+gomezDocument7 pagesEditor Chefe,+32 38+gomezAlessandra Irene GingatanNo ratings yet