Download as pdf or txt
You might also like
- An Interview With Elon MuskDocument2 pagesAn Interview With Elon MuskGiselle Medina Maximiano67% (3)
- Caries and Quality of Life in Portuguese Adolescents: Impact of Diet and Behavioural Risk FactorsDocument6 pagesCaries and Quality of Life in Portuguese Adolescents: Impact of Diet and Behavioural Risk FactorsCristian OneaNo ratings yet
- 2019 54 Pboci SugarDocument8 pages2019 54 Pboci SugarAlverina Putri RiandaNo ratings yet
- Smits 2019Document7 pagesSmits 2019mariapazvazquez99No ratings yet
- The Impact of Orthodontic Appliances On Eating - Young People's Views and Experiences.Document26 pagesThe Impact of Orthodontic Appliances On Eating - Young People's Views and Experiences.Naliana LupascuNo ratings yet
- Research Article The Association Between Nutritional Alterations and Oral Lesions in A Pediatric Population: An Epidemiological StudyDocument10 pagesResearch Article The Association Between Nutritional Alterations and Oral Lesions in A Pediatric Population: An Epidemiological StudyLeila FrotaNo ratings yet
- Vegetarian Diet and Its Possible Influence On Dental Health: A Systematic Literature ReviewDocument7 pagesVegetarian Diet and Its Possible Influence On Dental Health: A Systematic Literature ReviewTudor DumitrascuNo ratings yet
- Title: Children's Oral Health Strategy in The UKDocument8 pagesTitle: Children's Oral Health Strategy in The UKshahryar eskandarzadeNo ratings yet
- Oge 2018Document8 pagesOge 2018Ezekwueme AugustineNo ratings yet
- Journal Homepage: - : IntroductionDocument6 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Articulo Variables 1Document10 pagesArticulo Variables 1Diego LemurNo ratings yet
- Article - Behaviour in Adults With CairiesDocument6 pagesArticle - Behaviour in Adults With CairiesAashiq AshrafNo ratings yet
- Paper I - Ijerph-20-02511Document13 pagesPaper I - Ijerph-20-02511ed_mariachiNo ratings yet
- Basto 2018Document6 pagesBasto 2018Marilia SoaresNo ratings yet
- Shah 2020Document8 pagesShah 202021701101006 Rosita SariNo ratings yet
- Cousson Et Al 2012 GerodontologyDocument8 pagesCousson Et Al 2012 Gerodontologywiena aviolitaNo ratings yet
- Hubungan Pola Makan Dan Kebiasaan Menyikat Gigi Dengan Kesehatan Gigi Dan Mulut Karies Di Indonesia-with-cover-page-V2Document10 pagesHubungan Pola Makan Dan Kebiasaan Menyikat Gigi Dengan Kesehatan Gigi Dan Mulut Karies Di Indonesia-with-cover-page-V2titin kustiniNo ratings yet
- Hubungan Pola Makan Dan Kebiasaan Menyikat Gigi Dengan Kesehatan Gigi Dan Mulut Karies Di Indonesia-with-cover-page-V2Document10 pagesHubungan Pola Makan Dan Kebiasaan Menyikat Gigi Dengan Kesehatan Gigi Dan Mulut Karies Di Indonesia-with-cover-page-V2Saidah HasyimNo ratings yet
- Prevention Perspective in Orthodontics and Dento-Facial OrthopedicsDocument6 pagesPrevention Perspective in Orthodontics and Dento-Facial OrthopedicsRalucaNo ratings yet
- Attitudes and Lifestyle Factors in Relation To Oral Health and Dental Care in Sweden A Cross Sectional StudyDocument9 pagesAttitudes and Lifestyle Factors in Relation To Oral Health and Dental Care in Sweden A Cross Sectional Studyasem sardyNo ratings yet
- Association of Obesity With Periodontitis, Tooth Loss and Oral Hygiene in Non-Smoking AdultsDocument6 pagesAssociation of Obesity With Periodontitis, Tooth Loss and Oral Hygiene in Non-Smoking AdultsNicolas YoungNo ratings yet
- 1 s2.0 S0020653921001350 MainDocument7 pages1 s2.0 S0020653921001350 Maindeni harunNo ratings yet
- Literature Review-Danielle LelandDocument6 pagesLiterature Review-Danielle Lelandapi-754128823No ratings yet
- Editorial June 2016Document3 pagesEditorial June 2016Risha faricha NabilaNo ratings yet
- 237 Sophia Gomes Literature Review PaperDocument8 pages237 Sophia Gomes Literature Review Paperapi-720120569No ratings yet
- Dentistry 12 00078Document11 pagesDentistry 12 00078adiNo ratings yet
- EdentulismoDocument7 pagesEdentulismoAMELIA PAZ LETELIER AGUIRRENo ratings yet
- Nutrition Awareness and Oral Health Among Dental Patients inDocument11 pagesNutrition Awareness and Oral Health Among Dental Patients intue minhNo ratings yet
- Grand Challenges in Community Oral HealthDocument2 pagesGrand Challenges in Community Oral HealthOfelia ReyesNo ratings yet
- Dissertation Topics in Community DentistryDocument7 pagesDissertation Topics in Community DentistryOnlinePaperWritingServiceCanada100% (1)
- 1-S2.0-S0002916522010693-Main InterDocument8 pages1-S2.0-S0002916522010693-Main InterAlimah PutriNo ratings yet
- ESMEILI Et Al Dentist Attitudes and Practice Related in The Dental SetingDocument7 pagesESMEILI Et Al Dentist Attitudes and Practice Related in The Dental SetingJardelSantosNo ratings yet
- Oral HygieneDocument9 pagesOral HygieneemeraldwxyzNo ratings yet
- Women'S: A Literature Review OnDocument14 pagesWomen'S: A Literature Review OnAudrey Kristina MaypaNo ratings yet
- Current Challenges On Diagnosis and Management of Dental Erosion Literature Update and Case ReportDocument10 pagesCurrent Challenges On Diagnosis and Management of Dental Erosion Literature Update and Case ReportStefani WijayaNo ratings yet
- Healthcare 10 00406Document12 pagesHealthcare 10 00406AamirNo ratings yet
- Article Numgggber 2Document6 pagesArticle Numgggber 2Hub SciNo ratings yet
- Ecc Lit Review - PDocument7 pagesEcc Lit Review - Papi-720438286No ratings yet
- Diabetes and Oral Health: A Case-Control Study: BackgroundDocument4 pagesDiabetes and Oral Health: A Case-Control Study: BackgroundazifattahNo ratings yet
- Role of Dietary Habits and Diet in CariesDocument6 pagesRole of Dietary Habits and Diet in CariesȘenchea Crina ElenaNo ratings yet
- Oral Health Knowledge and Behavior Among Adults With DiabetesDocument8 pagesOral Health Knowledge and Behavior Among Adults With DiabetesKarina HernandezNo ratings yet
- Dental Education: Oral Health Behaviour and Awareness of Young Population in TurkeyDocument7 pagesDental Education: Oral Health Behaviour and Awareness of Young Population in TurkeyGabriel LazarNo ratings yet
- The Global Burden of Oral Diseases and Risks To orDocument10 pagesThe Global Burden of Oral Diseases and Risks To orViviane GodoiNo ratings yet
- Ref - ECC RHS-Phase-2-articleDocument10 pagesRef - ECC RHS-Phase-2-articlePROF. ERWIN M. GLOBIO, MSITNo ratings yet
- Factors Associated To Oral Health Related Quality of Life in Patients With DiabetesDocument19 pagesFactors Associated To Oral Health Related Quality of Life in Patients With DiabeteseveliiiinNo ratings yet
- WHO Global Consultation On Public Health Intervention Against Early Childhood CariesDocument8 pagesWHO Global Consultation On Public Health Intervention Against Early Childhood CariesThaliaNo ratings yet
- Intl J Eating Disorders - 1998 - Milosevic - Dental Erosion Oral Hygiene and Nutrition in Eating DisordersDocument5 pagesIntl J Eating Disorders - 1998 - Milosevic - Dental Erosion Oral Hygiene and Nutrition in Eating DisordersNawaf RuwailiNo ratings yet
- Dentists and Preventive Oral Health Care: February 2012Document27 pagesDentists and Preventive Oral Health Care: February 2012Mike Lawrence CadizNo ratings yet
- Journal of Clinical Immunology & MicrobiologyDocument14 pagesJournal of Clinical Immunology & MicrobiologyAthenaeum Scientific PublishersNo ratings yet
- Prpic2012 PDFDocument6 pagesPrpic2012 PDFNicolas YoungNo ratings yet
- Obesity and Oral Health - Is There An Association?: Collegium Antropologicum September 2012Document6 pagesObesity and Oral Health - Is There An Association?: Collegium Antropologicum September 2012Nicolas YoungNo ratings yet
- Obesity and Oral Health - Is There An Association?: Collegium Antropologicum September 2012Document6 pagesObesity and Oral Health - Is There An Association?: Collegium Antropologicum September 2012Nicolas YoungNo ratings yet
- Prpic2012 PDFDocument6 pagesPrpic2012 PDFNicolas YoungNo ratings yet
- 1 s2.0 S2213398422000392 MainDocument9 pages1 s2.0 S2213398422000392 MainMoad RuzkiNo ratings yet
- Bab 1-5 Manajemen HcuDocument7 pagesBab 1-5 Manajemen Hcuretno indriyaniNo ratings yet
- Poor Oral HealthDocument10 pagesPoor Oral HealthAwais FaridiNo ratings yet
- Makalah BLM EditDocument26 pagesMakalah BLM EditnikolausNo ratings yet
- Makalah BLM EditDocument26 pagesMakalah BLM EditnikolausNo ratings yet
- Children: Dental Caries and Oral Health in Children-Special IssueDocument3 pagesChildren: Dental Caries and Oral Health in Children-Special IssuecareNo ratings yet
- Dental CariesDocument41 pagesDental Cariescopy smartNo ratings yet
- Eating - and Oral Health-Related Quality of Life in Patients Under Fixed Orthodontic TreatmentDocument10 pagesEating - and Oral Health-Related Quality of Life in Patients Under Fixed Orthodontic TreatmentNaliana LupascuNo ratings yet
- Adherence To Dietary Advice and Oral Hygiene Practices Among Orthodontic PatientsDocument10 pagesAdherence To Dietary Advice and Oral Hygiene Practices Among Orthodontic PatientsNaliana LupascuNo ratings yet
- Assessing Diets of Children and AdolescentsDocument7 pagesAssessing Diets of Children and AdolescentsNaliana LupascuNo ratings yet
- DiagnosticDocument7 pagesDiagnosticNaliana LupascuNo ratings yet
- Self-Reported Pain After Orthodontic Treatments - A Randomized Controlled Study On The Effects of Two Follow-Up ProceduresDocument6 pagesSelf-Reported Pain After Orthodontic Treatments - A Randomized Controlled Study On The Effects of Two Follow-Up ProceduresNaliana LupascuNo ratings yet
- Brushing Characteristics and Dietary Patterns of Orthodontic Patients With Fixed AppliancesDocument3 pagesBrushing Characteristics and Dietary Patterns of Orthodontic Patients With Fixed AppliancesNaliana LupascuNo ratings yet
- Research Article: Chemical Kinetic Study On Dual-Fuel Combustion: The Ignition Properties of n-Dodecane/Methane MixtureDocument17 pagesResearch Article: Chemical Kinetic Study On Dual-Fuel Combustion: The Ignition Properties of n-Dodecane/Methane MixtureNaliana LupascuNo ratings yet
- 2015 NullDocument8 pages2015 NullNaliana LupascuNo ratings yet
- Facial Harmony in Orthodontic Diagnosis and PlanningDocument6 pagesFacial Harmony in Orthodontic Diagnosis and PlanningNaliana LupascuNo ratings yet
- Chapter 02Document10 pagesChapter 02Naliana LupascuNo ratings yet
- Chem RevDocument21 pagesChem RevNaliana LupascuNo ratings yet
- Now Zari Jorgensen Dental Implant Maintenance PDFDocument23 pagesNow Zari Jorgensen Dental Implant Maintenance PDFNaliana LupascuNo ratings yet
- Recent Advances in Heterogeneous Catalysis For TheDocument17 pagesRecent Advances in Heterogeneous Catalysis For TheNaliana LupascuNo ratings yet
- Aquatic FinalDocument8 pagesAquatic FinalNaliana LupascuNo ratings yet
- Publication 12 18639 6095Document4 pagesPublication 12 18639 6095Naliana LupascuNo ratings yet
- Thermophysical Properties of Methane: Articles You May Be Interested inDocument57 pagesThermophysical Properties of Methane: Articles You May Be Interested inNaliana LupascuNo ratings yet
- Chemistry A European J - 2020 - Zheng - Importance of Methane Chemical Potential For Its Conversion To Methanol OnDocument6 pagesChemistry A European J - 2020 - Zheng - Importance of Methane Chemical Potential For Its Conversion To Methanol OnNaliana LupascuNo ratings yet
- The Evolution of Danube Delta After Black Sea Reconnection To World OceanDocument30 pagesThe Evolution of Danube Delta After Black Sea Reconnection To World OceanNaliana LupascuNo ratings yet
- l56249 Copy 151228151622Document8 pagesl56249 Copy 151228151622Naliana LupascuNo ratings yet
- Bio Methane Based Chemicals Bio Gas As A Feedstoc-Groen Kennisnet 176949Document15 pagesBio Methane Based Chemicals Bio Gas As A Feedstoc-Groen Kennisnet 176949Naliana LupascuNo ratings yet
- Research Article: Methane Activation and Transformation On PolyoxometalatesDocument10 pagesResearch Article: Methane Activation and Transformation On PolyoxometalatesNaliana LupascuNo ratings yet
- Department of Pedodontics and Preventive Dentistry: Ozone Therapy in Dentistry 38 'Document6 pagesDepartment of Pedodontics and Preventive Dentistry: Ozone Therapy in Dentistry 38 'Naliana LupascuNo ratings yet
- Computational Study of Influence of Inflow Port Channel Design On Spark-Ignition Natural Gas Engine ParametersDocument7 pagesComputational Study of Influence of Inflow Port Channel Design On Spark-Ignition Natural Gas Engine ParametersNaliana LupascuNo ratings yet
- Gallo 2021 IOP Conf. Ser. Earth Environ. Sci. 707 012001Document8 pagesGallo 2021 IOP Conf. Ser. Earth Environ. Sci. 707 012001Naliana LupascuNo ratings yet
- Water Pollution in The Southern Coastal Region of The Black SeaDocument12 pagesWater Pollution in The Southern Coastal Region of The Black SeaNaliana LupascuNo ratings yet
- The Formula 1 Hybrid Power Units 2014-2015 PDFDocument161 pagesThe Formula 1 Hybrid Power Units 2014-2015 PDFNaliana LupascuNo ratings yet
- Finite Element Method (FEM) Modeling of The Powder Compaction of Cosmetic Products: Comparison Between Simulated and Experimental ResultsDocument2 pagesFinite Element Method (FEM) Modeling of The Powder Compaction of Cosmetic Products: Comparison Between Simulated and Experimental ResultsNaliana LupascuNo ratings yet
- Reducing Diesel EngineDocument10 pagesReducing Diesel EngineNaliana LupascuNo ratings yet
- FractureDocument16 pagesFractureps4haris.ch3534No ratings yet
- Abb 1677859211Document43 pagesAbb 1677859211Mohamed ElsayedNo ratings yet
- NPN TransistorDocument1 pageNPN TransistorsphinxNo ratings yet
- Age of Child Vaccines Needed How and Where It Is GivenDocument1 pageAge of Child Vaccines Needed How and Where It Is GivenKwenaNo ratings yet
- Comprehensive Operations Planning Directive (COPD) IntroductionDocument4 pagesComprehensive Operations Planning Directive (COPD) Introductionstlpts75100% (1)
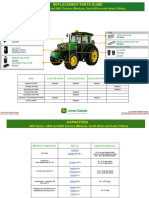
- 6003 Series 6403 and 6603 Tractors Mexico South Africa and Asian Edition Replacement Parts GuideDocument3 pages6003 Series 6403 and 6603 Tractors Mexico South Africa and Asian Edition Replacement Parts GuidePedro ValerioNo ratings yet
- The Legend of Lake TobaDocument2 pagesThe Legend of Lake Tobamesin cuci15No ratings yet
- Electricity Worksheet Physics GcseDocument5 pagesElectricity Worksheet Physics Gcsetun1123tNo ratings yet
- 14386l Camu 11670 Rev34 IngleseDocument253 pages14386l Camu 11670 Rev34 Inglesejohnysonycum0% (1)
- PE PipesDocument28 pagesPE Pipesmanar rafikNo ratings yet
- Worksheet 1Document7 pagesWorksheet 1ndtitcNo ratings yet
- Governing System of 210mw KwuDocument21 pagesGoverning System of 210mw KwuNitesh Rasekar100% (5)
- Diet Dan Olahraga Sebagai Upaya Pengendalian Kadar Gula Darah Pada Pasien Diabetes Melitus Tipe 2 Di Poliklinik Penyakit Dalam RSUD Ulin Banjarmasin Tahun 2015Document10 pagesDiet Dan Olahraga Sebagai Upaya Pengendalian Kadar Gula Darah Pada Pasien Diabetes Melitus Tipe 2 Di Poliklinik Penyakit Dalam RSUD Ulin Banjarmasin Tahun 2015Haifatul AlimahNo ratings yet
- A 304 - 11 Aceros Tipo HDocument48 pagesA 304 - 11 Aceros Tipo Halucard375No ratings yet
- CH 02Document48 pagesCH 02miathegirl9No ratings yet
- General Pre Stress and ElasticDocument28 pagesGeneral Pre Stress and ElasticJorge Nickolai NavalesNo ratings yet
- 1.a Form Heavy ElementsDocument6 pages1.a Form Heavy ElementsJoshua BermoyNo ratings yet
- Inteligent Street LightingDocument14 pagesInteligent Street LightingMariana PereiraNo ratings yet
- The Wheel and The BobsleighDocument2 pagesThe Wheel and The BobsleighHarisNo ratings yet
- Industrial PaintingDocument312 pagesIndustrial Paintingyoners1691No ratings yet
- 1st Grade VocabularyDocument1 page1st Grade VocabularyamirNo ratings yet
- Additional Charges of Daos in Agt 2019Document17 pagesAdditional Charges of Daos in Agt 2019heraldNo ratings yet
- Review of Pipeline Integrity ManagementDocument8 pagesReview of Pipeline Integrity ManagementTaib Anwar100% (2)
- Operating Instruction Analytical Balance: Kern AbtDocument71 pagesOperating Instruction Analytical Balance: Kern AbtdexterpoliNo ratings yet
- Exp9 1Document3 pagesExp9 1Ashley De LeonNo ratings yet
- Expt - 11: JFET CharacteristicsDocument8 pagesExpt - 11: JFET CharacteristicssamarthNo ratings yet
- LabVentMgmt RPDocument100 pagesLabVentMgmt RPGanesh.MahendraNo ratings yet
- Full Metal Crown ConstructionDocument48 pagesFull Metal Crown ConstructionAnonymous k8rDEsJsU1100% (1)
- Jacaratia Mexicana Edible and Medicinal Plant Uses of Tropical Deciduous Forest Species Yucatecan Maya 1991Document13 pagesJacaratia Mexicana Edible and Medicinal Plant Uses of Tropical Deciduous Forest Species Yucatecan Maya 1991María José TorallaNo ratings yet