Download as docx, pdf, or txt
You might also like
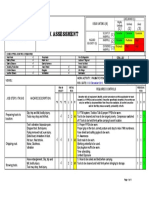
- Risk Assessment & Control Register - Grease Trap CleaningDocument7 pagesRisk Assessment & Control Register - Grease Trap CleaningAbdul RahmanNo ratings yet
- HOMOEOPATHY (H) EARS HIM OUT! Homoeopathic Cure of A Boy With Atticoantral CSOMDocument5 pagesHOMOEOPATHY (H) EARS HIM OUT! Homoeopathic Cure of A Boy With Atticoantral CSOMHomoeopathic PulseNo ratings yet
- Nursing Home Lesson PlanDocument13 pagesNursing Home Lesson Planapi-353466401100% (1)
- Questions&Answers: Meniere's Disease PresentationDocument55 pagesQuestions&Answers: Meniere's Disease Presentationimran qazi100% (1)
- Amref Directorate of Learning Systems: Distance Education CoursesDocument27 pagesAmref Directorate of Learning Systems: Distance Education CoursesOlya KunytskaNo ratings yet
- TLC Noah HeerDocument3 pagesTLC Noah HeerAlain SalsaMan BazilNo ratings yet
- AOEGuidelinePatientFAQFinal 0 PDFDocument2 pagesAOEGuidelinePatientFAQFinal 0 PDFMohamed JubranNo ratings yet
- On Ect: Can You Hear Me Now? GoodDocument5 pagesOn Ect: Can You Hear Me Now? Goodabrook8877No ratings yet
- Children Tonsil SurgeryDocument2 pagesChildren Tonsil SurgeryzulfanizaarNo ratings yet
- Om 3Document10 pagesOm 3Ma.rose AndresNo ratings yet
- Cleveland Clinic Journal of Medicine-2004-Sabella-S10Document9 pagesCleveland Clinic Journal of Medicine-2004-Sabella-S10farel@No ratings yet
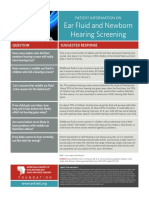
- Ear Fluid and Newborn Hearing Screening: Patient Information OnDocument1 pageEar Fluid and Newborn Hearing Screening: Patient Information OnMerlin NoronhaNo ratings yet
- AntibioticDocument5 pagesAntibioticTumon HazarikaNo ratings yet
- Ear Infection With Discharge: Patient Information From The BMJ GroupDocument3 pagesEar Infection With Discharge: Patient Information From The BMJ GroupHajamohamedNo ratings yet
- New Born Hearing FactsDocument8 pagesNew Born Hearing FactsAhiawortor Kplorla100% (1)
- Your Baby's Hearing Screening and Next StepsDocument6 pagesYour Baby's Hearing Screening and Next Stepsrameezchaudhary964No ratings yet
- Condition 136 Fever, Irritability, Ear Discharge: TasksDocument2 pagesCondition 136 Fever, Irritability, Ear Discharge: Tasksmohamed aissaNo ratings yet
- Anatomy of The EarDocument22 pagesAnatomy of The EarAnnalisa TellesNo ratings yet
- Explanation StationDocument4 pagesExplanation StationjsdlzjNo ratings yet
- Lesson 7 en LuanaDocument3 pagesLesson 7 en LuanaThor Batista AvengersNo ratings yet
- CHNDocument34 pagesCHNCatherine RomeroNo ratings yet
- CASE SIMUlation 112Document6 pagesCASE SIMUlation 112Princess Levie CenizaNo ratings yet
- Adenoidectomy - NHSDocument1 pageAdenoidectomy - NHSliammugwidiNo ratings yet
- Alt To Ear Pain-1Document5 pagesAlt To Ear Pain-1nonoNo ratings yet
- Contributing To Achieve The Goal of VISION 2020Document5 pagesContributing To Achieve The Goal of VISION 2020Michelle EchavezNo ratings yet
- Mobile Phones - Know Their Impact On Speech & Communication! - by Dr. Farheen Saif - LybrateDocument48 pagesMobile Phones - Know Their Impact On Speech & Communication! - by Dr. Farheen Saif - LybrateJayesh IsamaliyaNo ratings yet
- Hearing Tests For Babies and Young ChildrenDocument6 pagesHearing Tests For Babies and Young Childrengwenkz011No ratings yet
- Managing Otitis Media With Effusion in Young Children: Practice GuidelineDocument11 pagesManaging Otitis Media With Effusion in Young Children: Practice GuidelineJohn ThunderNo ratings yet
- What Is OtolaryngologyDocument37 pagesWhat Is OtolaryngologyPhạm Văn HiệpNo ratings yet
- CHN Prelim QuizDocument5 pagesCHN Prelim QuizVanessa Mae Rara100% (1)
- B 5Document2 pagesB 5menreethendy19No ratings yet
- Periodontal Care Plan - Thai HoangDocument21 pagesPeriodontal Care Plan - Thai Hoangapi-643588876No ratings yet
- Simulation Day WorksheetDocument3 pagesSimulation Day Worksheetapi-741208262No ratings yet
- Anotia/Microtia: Minnesota Department of Health Fact Sheet November 2005Document3 pagesAnotia/Microtia: Minnesota Department of Health Fact Sheet November 2005Carlos Santiago VivenzaNo ratings yet
- The 4 Most Common ENT Problems and How To Combat ThemDocument3 pagesThe 4 Most Common ENT Problems and How To Combat ThemFaizan ShahNo ratings yet
- HEENT Case Study 2Document5 pagesHEENT Case Study 2AlexanderWarrenNo ratings yet
- Aoe Guideline Pls FinalDocument2 pagesAoe Guideline Pls FinalJeffly Varro GilbertNo ratings yet
- Chrisanthopoulos Marika 300453 Cleft Lip and PalateDocument14 pagesChrisanthopoulos Marika 300453 Cleft Lip and PalateCharles IppolitoNo ratings yet
- O To SclerosisDocument4 pagesO To SclerosisDiah HayustiningsihNo ratings yet
- Otitis MediaDocument7 pagesOtitis MediaNader Smadi67% (3)
- Maximizing Auditory SlidesDocument18 pagesMaximizing Auditory SlidesARUNGREESMANo ratings yet
- Partial Glossectomy: Oxford Centre For Head and Neck OncologyDocument4 pagesPartial Glossectomy: Oxford Centre For Head and Neck OncologyromzikerenzNo ratings yet
- Otitis MediaDocument18 pagesOtitis Mediaapi-284314498No ratings yet
- Pediatric DentistryDocument8 pagesPediatric DentistryPavleta RashkovaNo ratings yet
- Chapter 64Document20 pagesChapter 64Prince K. TaileyNo ratings yet
- 4 Steps To Severe Hearing Loss TreatmentDocument8 pages4 Steps To Severe Hearing Loss TreatmentTon SawyerNo ratings yet
- Lisa Jordon Edited-1Document146 pagesLisa Jordon Edited-1Manthu BNo ratings yet
- Meningitis and Childhood Deafness: A Guide For FamiliesDocument36 pagesMeningitis and Childhood Deafness: A Guide For FamiliesNguyễn YếnNo ratings yet
- Managing Common Aches and Pains in Kids: A Parent's Handbook: Health, #9From EverandManaging Common Aches and Pains in Kids: A Parent's Handbook: Health, #9No ratings yet
- Vocal Health Notes 2020Document8 pagesVocal Health Notes 2020Joel LowNo ratings yet
- Hearing Problems - Hyperacusis: (HTTP://WWW - Betterhealth.vic - Gov.au/health/conditionsandtreatments/tinnitus)Document6 pagesHearing Problems - Hyperacusis: (HTTP://WWW - Betterhealth.vic - Gov.au/health/conditionsandtreatments/tinnitus)Sanath KumarNo ratings yet
- Biology Project ORAL CANCERDocument39 pagesBiology Project ORAL CANCERKashvi DevNo ratings yet
- A Simple Guide to Pre-auricular Pit, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Pre-auricular Pit, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Otitis MediaDocument9 pagesOtitis MediaMona Santi NainggolanNo ratings yet
- Cleft Lip or Cleft PalateDocument2 pagesCleft Lip or Cleft PalateKueenmae Unza SolivenNo ratings yet
- Children With Achondroplasia Guidance For Parents and Health Care ProfessionalsDocument22 pagesChildren With Achondroplasia Guidance For Parents and Health Care Professionalshorace35No ratings yet
- HSC 430 Childhood Disease PaperDocument10 pagesHSC 430 Childhood Disease Paperapi-502687231No ratings yet
- How - . - I Manage Deafness in Children and Young People.Document4 pagesHow - . - I Manage Deafness in Children and Young People.Speech & Language Therapy in PracticeNo ratings yet
- Health Condition1Document22 pagesHealth Condition1Barrack koderaNo ratings yet
- Nine Effective Home Remedies For EaracheDocument1 pageNine Effective Home Remedies For EarachekaralyntNo ratings yet
- Australian PRDocument1 pageAustralian PRaravindNo ratings yet
- Child With Poor Academic PerformanceDocument4 pagesChild With Poor Academic PerformancearavindNo ratings yet
- Chronic Heart FailureDocument3 pagesChronic Heart FailurearavindNo ratings yet
- Q2.Dizziness and FallsDocument5 pagesQ2.Dizziness and FallsaravindNo ratings yet
- Mu 06Document5 pagesMu 06aravindNo ratings yet
- Reference Values For and Interpretation of The Singapore Caregiver Quality of Life Scale: A Quantile Regression ApproachDocument10 pagesReference Values For and Interpretation of The Singapore Caregiver Quality of Life Scale: A Quantile Regression ApproacharavindNo ratings yet
- Module 1Document53 pagesModule 1aravindNo ratings yet
- Mbazc416 - M3Document99 pagesMbazc416 - M3aravindNo ratings yet
- Organizational Behavior (What's New in Management) - Stephen P. Robbins & TimotDocument1 pageOrganizational Behavior (What's New in Management) - Stephen P. Robbins & TimotaravindNo ratings yet
- Module 2Document68 pagesModule 2aravindNo ratings yet
- Mba Zc416 Ec-3r First Sem 2023-2024Document5 pagesMba Zc416 Ec-3r First Sem 2023-2024aravindNo ratings yet
- DiabetesDocument14 pagesDiabetesaravindNo ratings yet
- Risk Assessment No. 27 PNEUMATIC POWER TOOL Rev 0Document1 pageRisk Assessment No. 27 PNEUMATIC POWER TOOL Rev 0Lalit ChoudharyNo ratings yet
- Eucare Pharmaceuticals Private Limited Chennai IndiaDocument10 pagesEucare Pharmaceuticals Private Limited Chennai IndiaEucare Pharmaceuticals Private LimitedNo ratings yet
- Research Essay 1Document10 pagesResearch Essay 1api-582788002No ratings yet
- Q2 Module 6 DIASSDocument15 pagesQ2 Module 6 DIASSLearniedevy MitchNo ratings yet
- Mario Madridejos v. NYK Fil Shipmanagement, G.R. No. 204262, 07 June 2017Document3 pagesMario Madridejos v. NYK Fil Shipmanagement, G.R. No. 204262, 07 June 2017Cathy GabroninoNo ratings yet
- Medi 99 E20541Document3 pagesMedi 99 E20541wlNo ratings yet
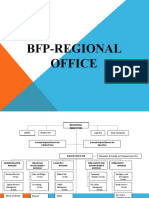
- OS For BFP Regional OfficeDocument23 pagesOS For BFP Regional OfficeJustine Paulo ManuelNo ratings yet
- New Thesis Topics in OrthopedicDocument8 pagesNew Thesis Topics in OrthopedicKarla Adamson100% (2)
- Report-Slaughter Workshop - Richard - Klottey - BotchwayDocument11 pagesReport-Slaughter Workshop - Richard - Klottey - BotchwayRichard Klottey BotchwayNo ratings yet
- Hand DhejeDocument21 pagesHand Dheje1bookwork1No ratings yet
- Unit 0 - Prioritize - Reasonable Adjustments and Special Considerations PolicyDocument4 pagesUnit 0 - Prioritize - Reasonable Adjustments and Special Considerations PolicyChloe ReyesNo ratings yet
- Ebook Ebook PDF Principles of Management v4 0 4th Edition by Talya Bauer PDFDocument41 pagesEbook Ebook PDF Principles of Management v4 0 4th Edition by Talya Bauer PDFrosalie.ashworth789100% (38)
- Literature Review - Annie MillsDocument5 pagesLiterature Review - Annie Millsapi-549219461No ratings yet
- IA1 - Mock AssessmentDocument3 pagesIA1 - Mock AssessmentMohammad Mokhtarul HaqueNo ratings yet
- ჟურნალი სრულიDocument113 pagesჟურნალი სრულიTengiz VerulavaNo ratings yet
- IM-CAP Concept MapDocument1 pageIM-CAP Concept MapTrisNo ratings yet
- PDF An Introduction To Orthodontics Simon J Littlewood Ebook Full ChapterDocument53 pagesPDF An Introduction To Orthodontics Simon J Littlewood Ebook Full Chapterandrea.buss250100% (7)
- Kennesaw State DissertationDocument6 pagesKennesaw State DissertationOnlinePaperWriterFargo100% (1)
- Laminar AirflowDocument15 pagesLaminar AirflowKamran AshrafNo ratings yet
- Safety Data Sheet: Section 1. IdentificationDocument12 pagesSafety Data Sheet: Section 1. Identificationraja duraiNo ratings yet
- Job Hazard AnalysisDocument9 pagesJob Hazard AnalysisMohammad HadoumiNo ratings yet
- Qualification Handbook v1-1Document92 pagesQualification Handbook v1-1rafael espinosa semperNo ratings yet
- كتالوج الأجهزة الطبيةDocument8 pagesكتالوج الأجهزة الطبيةIslam HosniNo ratings yet
- ENG 110-Task 4 (Unintended Messages)Document2 pagesENG 110-Task 4 (Unintended Messages)Erika Noreen Dela RosaNo ratings yet
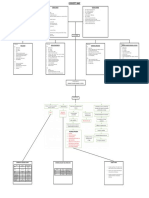
- LAB 2 LAB 3 Creating A Simple Patient Database RecordDocument10 pagesLAB 2 LAB 3 Creating A Simple Patient Database RecordIsabelle Hazel BenemileNo ratings yet
- AMBOSSDocument42 pagesAMBOSSlaralala562No ratings yet
- Internet Addiction TG UpdatedDocument12 pagesInternet Addiction TG UpdatedLamberto Pilatan Jr.No ratings yet
- Erikson's Psychosocial Stages of Development: By: Sean Sanko T/TH 11:00-12:15Document15 pagesErikson's Psychosocial Stages of Development: By: Sean Sanko T/TH 11:00-12:15sivakumarNo ratings yet
- IOGP Recommended PracticeDocument18 pagesIOGP Recommended Practiceivan rocoNo ratings yet