Download as pdf or txt
You might also like
- F U N W I S E: Know Your Symptom Severity Score!Document2 pagesF U N W I S E: Know Your Symptom Severity Score!Jamie Sebastian50% (2)
- Trigger Point Therapy for Myofascial Pain: The Practice of Informed TouchFrom EverandTrigger Point Therapy for Myofascial Pain: The Practice of Informed TouchRating: 4 out of 5 stars4/5 (5)
- Hygiene (NCLEX) Flashcards - QuizletDocument5 pagesHygiene (NCLEX) Flashcards - QuizletA.No ratings yet
- Chronic Pelvic Pain and Dysfunction: Practical Physical Medicine - Leon ChaitowDocument5 pagesChronic Pelvic Pain and Dysfunction: Practical Physical Medicine - Leon ChaitowrikadetiNo ratings yet
- 1 s2.0 S2590109523000058 MainDocument9 pages1 s2.0 S2590109523000058 MainJonathan IbañezNo ratings yet
- Percepciones FisioterapeutasDocument12 pagesPercepciones FisioterapeutasAleja VillacresNo ratings yet
- 201705gillespie 1Document9 pages201705gillespie 1Jose PerezNo ratings yet
- RiceetalJPain2019EIH ReviewDocument19 pagesRiceetalJPain2019EIH ReviewVictorNo ratings yet
- Physiotherapists Perceptions of Learning And.5Document19 pagesPhysiotherapists Perceptions of Learning And.5Doctor MemiNo ratings yet
- Manuscript Phys TherapyDocument8 pagesManuscript Phys TherapyJaviMéndezNo ratings yet
- British Pain ClinicDocument11 pagesBritish Pain ClinicdanaNo ratings yet
- Physical Therapy Research in Professional Clinical PracticeDocument5 pagesPhysical Therapy Research in Professional Clinical PracticeProductivity 100No ratings yet
- Orthopedic Manual Therapy 2nd Edition 2nd EditionDocument61 pagesOrthopedic Manual Therapy 2nd Edition 2nd Editionkevin.smart540100% (43)
- Operant Learning Theory in Pain and Chronic Pain RDocument11 pagesOperant Learning Theory in Pain and Chronic Pain RRhea AquinoNo ratings yet
- Manual Therapy: Neil Langridge, Lisa Roberts, Catherine PopeDocument6 pagesManual Therapy: Neil Langridge, Lisa Roberts, Catherine PopeVizaNo ratings yet
- Case StudyDocument4 pagesCase StudyArdhyan ArdhyanNo ratings yet
- Improving The Multidisciplinary Treatment of Chronic Pain by StimulatingDocument11 pagesImproving The Multidisciplinary Treatment of Chronic Pain by StimulatinginxaccccNo ratings yet
- Fifteen Years of Explaining Pain, The Past, Present, and Future 2016Document7 pagesFifteen Years of Explaining Pain, The Past, Present, and Future 2016Gilbert ThierryNo ratings yet
- Preview 15031 Greene Treatment of TmdsDocument24 pagesPreview 15031 Greene Treatment of TmdsManuel CastilloNo ratings yet
- How Do Physiotherapists Explain Influencing Factors To Chronic Low Back Pain? A Qualitative Study Using A Fictive Case of Chronic Non-Specific Low Back PainDocument13 pagesHow Do Physiotherapists Explain Influencing Factors To Chronic Low Back Pain? A Qualitative Study Using A Fictive Case of Chronic Non-Specific Low Back PainRoberto Kevin Nieto CovarrubiasNo ratings yet
- Effectiveness of Isometric Neck Exercises, Stretching and Ergonomics Over Ergonomic Alone For Neck Pain in PhysiotherapistsDocument6 pagesEffectiveness of Isometric Neck Exercises, Stretching and Ergonomics Over Ergonomic Alone For Neck Pain in PhysiotherapistsAndi Riska AmirullahNo ratings yet
- ACT For Chronic Pain For Groups HandbookDocument71 pagesACT For Chronic Pain For Groups HandbookLydia Collins100% (4)
- Consensus For Physiotherapy For Shoulder Pain: International Orthopaedics December 2014Document7 pagesConsensus For Physiotherapy For Shoulder Pain: International Orthopaedics December 2014LucyFloresNo ratings yet
- Patient Centerdness in Physiotherapy WhaDocument2 pagesPatient Centerdness in Physiotherapy Whapedroperestrelo96No ratings yet
- Harvey Overview PT JOP 2016Document9 pagesHarvey Overview PT JOP 2016Julenda CintarinovaNo ratings yet
- Exercise Altering Pain MemoriesDocument6 pagesExercise Altering Pain MemoriesCelia CaballeroNo ratings yet
- Estudio Efectividad Tto en Primaria Dolor CronicoDocument18 pagesEstudio Efectividad Tto en Primaria Dolor CronicoMaría José LópezNo ratings yet
- 1 s2.0 S0049017223000458 MainDocument17 pages1 s2.0 S0049017223000458 Main18. Lusiana Aprilia SariNo ratings yet
- Comsenço e Alogoritmo Reabilitacao Ombrto Klintberg2014Document6 pagesComsenço e Alogoritmo Reabilitacao Ombrto Klintberg2014Sandro PerilloNo ratings yet
- Orthopedic Manual Therapy 2Nd Edition 2Nd Edition Full Chapter PDFDocument53 pagesOrthopedic Manual Therapy 2Nd Edition 2Nd Edition Full Chapter PDFottohnabir100% (5)
- Coppieters IDocument15 pagesCoppieters Ihelenlamlam200011No ratings yet
- The Clinical Application of The Biopsychosocial ModelDocument24 pagesThe Clinical Application of The Biopsychosocial ModelLuis Alberto González SalomónNo ratings yet
- Lifestyle and Chronic PainDocument250 pagesLifestyle and Chronic PainStanley Wu TaiNo ratings yet
- Low Back Pain Literature ReviewDocument6 pagesLow Back Pain Literature Reviewafmzzulfmzbxet100% (1)
- Article OsteoDocument4 pagesArticle OsteorefNo ratings yet
- Consensus For Physiotherapy For Shoulder PainDocument7 pagesConsensus For Physiotherapy For Shoulder Painbian coniglioNo ratings yet
- vanderMeeretal2017HSQ DVDocument11 pagesvanderMeeretal2017HSQ DVThe AzmodeusNo ratings yet
- Physiotherapy Rehabilitation For People With Spinal Cord InjuriesDocument8 pagesPhysiotherapy Rehabilitation For People With Spinal Cord InjuriesAna Corina LopezNo ratings yet
- Physiotherapy: JournalofDocument3 pagesPhysiotherapy: JournalofFitriana Laela RahmawatiNo ratings yet
- Understanding Clinical Reasoning A Phenomenographic Study With Entry Level Physiotherapy StudentsDocument11 pagesUnderstanding Clinical Reasoning A Phenomenographic Study With Entry Level Physiotherapy StudentsVíctor Saul Sandoval SanchezNo ratings yet
- 1 s2.0 S1356689X01904266 MainDocument8 pages1 s2.0 S1356689X01904266 MainaramNo ratings yet
- How To Explain Central Sensitization To PatientsDocument6 pagesHow To Explain Central Sensitization To PatientsrameshkulkarNo ratings yet
- Jurnal FisioDocument2 pagesJurnal FisioNarul Nadzirah Binti Abdul MalekNo ratings yet
- Prof. DR - Manal Hamed: Prepared byDocument26 pagesProf. DR - Manal Hamed: Prepared byM EhabNo ratings yet
- Diploma in Osteopathic MedicineDocument15 pagesDiploma in Osteopathic MedicineSachin GoyalNo ratings yet
- Brazilian Journal of Physical TherapyDocument14 pagesBrazilian Journal of Physical TherapyxurraNo ratings yet
- Dekker Stauder Penedo Proposal Def BMparta 2017Document5 pagesDekker Stauder Penedo Proposal Def BMparta 2017Akshay BadoreNo ratings yet
- Pain Thesis StatementDocument5 pagesPain Thesis Statementmmwsmltgg100% (2)
- It Is Time To Move Beyond Body Region Silos' To Manage Musculoskeletal Pain - Five Actions To Change Clinical PracticeDocument3 pagesIt Is Time To Move Beyond Body Region Silos' To Manage Musculoskeletal Pain - Five Actions To Change Clinical PracticeTyler Latu'ilaNo ratings yet
- Musculoskeletal Care - 2024 - Powell - Is Exercise Therapy The Right Treatment For Rotator Cuff Related Shoulder PainDocument12 pagesMusculoskeletal Care - 2024 - Powell - Is Exercise Therapy The Right Treatment For Rotator Cuff Related Shoulder PainxurraNo ratings yet
- PIIS1526590018304565Document18 pagesPIIS1526590018304565gguida0No ratings yet
- Vlaeyen 2021 Low Back PainDocument16 pagesVlaeyen 2021 Low Back PainThawanny de CarvalhoNo ratings yet
- Work Related Musculoskeletal Disorders in Physiotherapists Challenges and Coping Strategies WRMSDs in PhysiotherapistsDocument5 pagesWork Related Musculoskeletal Disorders in Physiotherapists Challenges and Coping Strategies WRMSDs in PhysiotherapistsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Mechanical Neck 2021Document12 pagesMechanical Neck 2021andressareis066No ratings yet
- Wilson 2015Document2 pagesWilson 2015Ricardo Peraza RiveroNo ratings yet
- 1 s2.0 S0894113016300114 MainDocument13 pages1 s2.0 S0894113016300114 Mainwengi yipNo ratings yet
- Pain Measurement in Patients With Low Back PainDocument9 pagesPain Measurement in Patients With Low Back PainAnakagung Vinna ParamitaNo ratings yet
- Massage Therapist'Document207 pagesMassage Therapist'omar alaa kaiokenNo ratings yet
- Lisa 2016Document8 pagesLisa 2016druketo vndmatNo ratings yet
- Effective Treatment Options For Musculoskeletal Pain in Primary Care: A Systematic Overview of Current EvidenceDocument30 pagesEffective Treatment Options For Musculoskeletal Pain in Primary Care: A Systematic Overview of Current EvidenceAndrewL91No ratings yet
- Pain Research PaperDocument5 pagesPain Research Paperuwtsmecnd100% (1)
- Evidence-Based Evaluation & Management of Common Spinal Conditions: A Guide for the Manual PractitionerFrom EverandEvidence-Based Evaluation & Management of Common Spinal Conditions: A Guide for the Manual PractitionerRating: 5 out of 5 stars5/5 (1)
- Lo PsDocument21 pagesLo Psloveth konniaNo ratings yet
- Design For Elderly Drivers and Signal TimingDocument19 pagesDesign For Elderly Drivers and Signal TimingMigz EscutinNo ratings yet
- Child Development Stages Matrix: 0-3 Months 3-6 MonthsDocument6 pagesChild Development Stages Matrix: 0-3 Months 3-6 MonthsJoenard Sadorra CabaelNo ratings yet
- Cofton Prospectus 2020-21 FINALDocument19 pagesCofton Prospectus 2020-21 FINALtheehengNo ratings yet
- Emergency Department PolicyDocument18 pagesEmergency Department PolicyKumar Gavali Suryanarayana100% (1)
- QC How To Make A Good Method StatementDocument3 pagesQC How To Make A Good Method StatementRsjBugtongNo ratings yet
- Tr. Iridodialysis With HyphaemaDocument21 pagesTr. Iridodialysis With HyphaemaSyed NabilNo ratings yet
- Mortality July 2023Document40 pagesMortality July 2023Tazin Ahmed AdnanNo ratings yet
- English For NursesDocument137 pagesEnglish For NursesLIDYANo ratings yet
- Marketing Strategies of ColgateDocument19 pagesMarketing Strategies of Colgateshirley shekharan86% (14)
- Konru 3 Sep 2022Document24 pagesKonru 3 Sep 2022sibbNo ratings yet
- Bioenergetics of Exercising HumansDocument26 pagesBioenergetics of Exercising HumansMasajes A DomicilioNo ratings yet
- Womans World USA - October 24 2022Document56 pagesWomans World USA - October 24 2022Cristina Popescu100% (1)
- Theories of AgingDocument8 pagesTheories of Agingcatsteven castillo100% (1)
- JasperDocument9 pagesJasperkrisha mandriqueNo ratings yet
- Report No. 11 of 2023 - PA On PMJAY - English PDF A 064d22bab2b83b5.38721048Document168 pagesReport No. 11 of 2023 - PA On PMJAY - English PDF A 064d22bab2b83b5.38721048arish.khanNo ratings yet
- Pedialyte For Kids - Google SearchDocument1 pagePedialyte For Kids - Google SearchJethea NaguitNo ratings yet
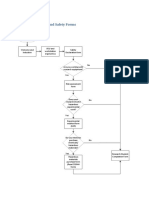
- Flow Chart: Health and Safety FormsDocument2 pagesFlow Chart: Health and Safety FormsBenouna FertNo ratings yet
- Artefacts: How Human Trafficking Impacts Its Victims and What Type of Support They NeedDocument11 pagesArtefacts: How Human Trafficking Impacts Its Victims and What Type of Support They NeedKendra GayleNo ratings yet
- 1119GB en Tip Top Heating Solution STL-RF4 Free of 0056Document7 pages1119GB en Tip Top Heating Solution STL-RF4 Free of 0056Guang ChenzNo ratings yet
- Death Investigation:: A Guide For The Scene InvestigatorDocument72 pagesDeath Investigation:: A Guide For The Scene Investigatorraul contreNo ratings yet
- ALIGN Certificacion ISO 9001Document1 pageALIGN Certificacion ISO 9001Kendall ArayaNo ratings yet
- Alpesh Patel: Sam's Club Pharmacy: (2011-Current) Wal-Mart Pharmacy: (September 2005-2011)Document2 pagesAlpesh Patel: Sam's Club Pharmacy: (2011-Current) Wal-Mart Pharmacy: (September 2005-2011)Hani EsmaelNo ratings yet
- RWS Q4 Module5Document22 pagesRWS Q4 Module5Romeo GasparNo ratings yet
- OCD in ChildrenDocument10 pagesOCD in ChildrenKreshnik IdrizajNo ratings yet
- Diabetes Medications Chart PDFDocument1 pageDiabetes Medications Chart PDFRachel Lalaine Marie SialanaNo ratings yet
- Mona NasrallahDocument1 pageMona NasrallahWa3d HalabiNo ratings yet
- SDO Navotas Health9 Q2 Lumped - FVDocument50 pagesSDO Navotas Health9 Q2 Lumped - FVMarie TiffanyNo ratings yet