Download as docx, pdf, or txt
You might also like
- Discharge PlanDocument5 pagesDischarge PlanYoshimi Salazar Sasaki100% (1)
- NCP Ineffective Cerebral Tissue PerfusionDocument2 pagesNCP Ineffective Cerebral Tissue PerfusionAngelo ︻╦̵̵͇̿̿̿̿╤── Bulacan50% (6)
- JOURNAL CLUB Jaswanth 105220 Am - 796a31Document26 pagesJOURNAL CLUB Jaswanth 105220 Am - 796a31pradeepgullipalli.1089No ratings yet
- As ResearcDocument6 pagesAs ResearcANITTA SNo ratings yet
- kkk1471 2458 14 395 PDFDocument6 pageskkk1471 2458 14 395 PDFyuusuf cali RoobleNo ratings yet
- Research ArticleDocument13 pagesResearch ArticleDENNYNo ratings yet
- Research Revised March 22 2024Document39 pagesResearch Revised March 22 2024amandigNo ratings yet
- June 04, 2010: Predisposing Factors of Pneumonia in Pediatric WardDocument5 pagesJune 04, 2010: Predisposing Factors of Pneumonia in Pediatric WardJanry ╭∩∩╮⎛⏜⏟〤 ⎞╭∩∩╮ ClementNo ratings yet
- Alalag, Elsie: "The Impact of Access To Immunization Information On Vaccine Acceptance in Three Countries"Document4 pagesAlalag, Elsie: "The Impact of Access To Immunization Information On Vaccine Acceptance in Three Countries"Basema HashhashNo ratings yet
- ROL FinalDocument28 pagesROL FinalSiyona BansodeNo ratings yet
- Environmental Factors Associated With Acute Diarrhea Among Children Under Five Years of Age in Derashe District, Southern EthiopiaDocument10 pagesEnvironmental Factors Associated With Acute Diarrhea Among Children Under Five Years of Age in Derashe District, Southern Ethiopiadefitri sariningtyasNo ratings yet
- Hinsarmu Published ThesisDocument14 pagesHinsarmu Published ThesisHinsarmu AmanoNo ratings yet
- Research TitilDocument6 pagesResearch Titilhaimanotgedlu11No ratings yet
- A Study On Knowledge and Practice of Mothers of Under-Five ChildrenDocument6 pagesA Study On Knowledge and Practice of Mothers of Under-Five ChildrenRirin PurbaNo ratings yet
- A Study of Acute Malnutrition Among Children in NRCDocument11 pagesA Study of Acute Malnutrition Among Children in NRCkharemixNo ratings yet
- Systematic Literature Review of Oral HygieneDocument52 pagesSystematic Literature Review of Oral HygieneAnkit Kothiyal0% (1)
- Dialnet DemographicCharacteristicsNutritionalStatusDietary 7133937 PDFDocument10 pagesDialnet DemographicCharacteristicsNutritionalStatusDietary 7133937 PDFHighlander Emmanuel Fuentes BeltránNo ratings yet
- Diarrhea Prevention Through Food Safety EducationDocument4 pagesDiarrhea Prevention Through Food Safety Educationceking99No ratings yet
- OB Journal AppraisalDocument2 pagesOB Journal AppraisalAlloiBialbaNo ratings yet
- Asma 4Document4 pagesAsma 4chintya maretaNo ratings yet
- The Problem and Its BackgroundDocument11 pagesThe Problem and Its BackgroundAlicetair Buncad LopezNo ratings yet
- Jurnal Home VisitDocument7 pagesJurnal Home VisitNikchrisstal Queenlover'sNo ratings yet
- Thyroid ReviewDocument45 pagesThyroid ReviewSharin K VargheseNo ratings yet
- Unhealthy Food Consumption in Adolescence: Role of Sedentary Behaviours and Modifiers in 11-, 13-And 15-Year-Old ItaliansDocument7 pagesUnhealthy Food Consumption in Adolescence: Role of Sedentary Behaviours and Modifiers in 11-, 13-And 15-Year-Old ItaliansJason DenostaNo ratings yet
- Role of Social Class in Caries Occurrence in 12 Year Olds in Turin, ItalyDocument5 pagesRole of Social Class in Caries Occurrence in 12 Year Olds in Turin, ItalyEugeniaFerdohlebNo ratings yet
- Research PaperDocument19 pagesResearch PaperDearlyne AlmazanNo ratings yet
- INFANT AND YOUNG CHILD FEEDING AND CARE PRACTICES OF CAREGIVERS IN ALBAY PHILIPPINES - Journal ArticleDocument27 pagesINFANT AND YOUNG CHILD FEEDING AND CARE PRACTICES OF CAREGIVERS IN ALBAY PHILIPPINES - Journal ArticleEmilee Joice Rochelle MalutoNo ratings yet
- Factors Influencing Malnutrition Among Under Five Children at Kitwe Teaching Hospital, ZambiaDocument10 pagesFactors Influencing Malnutrition Among Under Five Children at Kitwe Teaching Hospital, ZambiaInternational Journal of Current Innovations in Advanced Research100% (1)
- Article: N M Nsele, MB CHB, FC Paed (Sa) N H MckerrowDocument4 pagesArticle: N M Nsele, MB CHB, FC Paed (Sa) N H MckerrowyutefupNo ratings yet
- Hospital Outcomes For Paediatric Pneumonia and Diarrhoea Patients Admitted in A Tertiary Hospital On Weekdays Versus Weekends: A Retrospective StudyDocument9 pagesHospital Outcomes For Paediatric Pneumonia and Diarrhoea Patients Admitted in A Tertiary Hospital On Weekdays Versus Weekends: A Retrospective StudyZidni Arifa LuthfiNo ratings yet
- A Randomized, Community-Based Trial of Home Visiting To Reduce Blood Lead Levels in ChildrenDocument9 pagesA Randomized, Community-Based Trial of Home Visiting To Reduce Blood Lead Levels in ChildrenFitriatun NisaNo ratings yet
- Action Plan: College of NursingDocument5 pagesAction Plan: College of NursingErika MarieNo ratings yet
- Effectiveness of Integrated NuDocument9 pagesEffectiveness of Integrated NuPuspita GasaliNo ratings yet
- Research StudyDocument2 pagesResearch StudyHadaza LanaNo ratings yet
- Identifying Impacts On Education and Health in The Presence of Treatment ExternalitiesDocument59 pagesIdentifying Impacts On Education and Health in The Presence of Treatment ExternalitiesStéphane KedieNo ratings yet
- Early Childhood Caries and Body Mass Index in Young Children From Low Income FamiliesDocument12 pagesEarly Childhood Caries and Body Mass Index in Young Children From Low Income FamiliesAmandeep ChopraNo ratings yet
- Ijerph 17 04664 v2Document21 pagesIjerph 17 04664 v2vijay dagdiNo ratings yet
- Maternal Knowledge, Attitudes and Practices Towards Prevention and Management of Child Diarrhoea in Urban and Rural Maseru, LesothoDocument20 pagesMaternal Knowledge, Attitudes and Practices Towards Prevention and Management of Child Diarrhoea in Urban and Rural Maseru, LesothoAnisa SafutriNo ratings yet
- Article SssssssssssssssssssDocument7 pagesArticle SssssssssssssssssssBULAN IFTINAZHIFANo ratings yet
- Jurnal GadarDocument10 pagesJurnal GadarRiandini PandansariNo ratings yet
- Research ArticleDocument10 pagesResearch ArticlealpahchichupsNo ratings yet
- Soil-Transmitted Helminths Infection Among Primary School Students: Which Policy Should Be Emphasized?Document7 pagesSoil-Transmitted Helminths Infection Among Primary School Students: Which Policy Should Be Emphasized?IJPHSNo ratings yet
- The Long Run Effects of Early Childhood Deworming On Literacy and Numeracy: Evidence From UgandaDocument25 pagesThe Long Run Effects of Early Childhood Deworming On Literacy and Numeracy: Evidence From UgandaElijah GracillaNo ratings yet
- HelminthDocument27 pagesHelminthHelsie DahokloryNo ratings yet
- IIN RobertRCetal - healthEducationResearch.vol22.No.3Document14 pagesIIN RobertRCetal - healthEducationResearch.vol22.No.3Iniciativa Contra la Desnutrición Infantil - IDINo ratings yet
- Factors Constraining Adherence SDocument20 pagesFactors Constraining Adherence SayangsarulNo ratings yet
- Does A Clinical Guideline Change Chlamydia Testing?Document7 pagesDoes A Clinical Guideline Change Chlamydia Testing?gt_shadowNo ratings yet
- Why Caretakers Bypass Primary Health Care Facilities For Child Care - A Case From Rural TanzaniaDocument10 pagesWhy Caretakers Bypass Primary Health Care Facilities For Child Care - A Case From Rural TanzaniajlventiganNo ratings yet
- Final PDFDocument19 pagesFinal PDFAnne BaltazarNo ratings yet
- Incidence and Risk Factors of Childhood Pneumonia-Like Episodes in Biliran Island, Philippines-A Community-Based StudyDocument3 pagesIncidence and Risk Factors of Childhood Pneumonia-Like Episodes in Biliran Island, Philippines-A Community-Based Studymegreen GamingNo ratings yet
- Dr. Piyush Ranjan, Department of Medicine, AIIMS, January (2019)Document21 pagesDr. Piyush Ranjan, Department of Medicine, AIIMS, January (2019)Sree LathaNo ratings yet
- Stunting GDocument3 pagesStunting GidahNo ratings yet
- Review Article: Impact of Water, Sanitation, and Hygiene Interventions On Improving Health Outcomes Among School ChildrenDocument11 pagesReview Article: Impact of Water, Sanitation, and Hygiene Interventions On Improving Health Outcomes Among School ChildrenArum FibriantiNo ratings yet
- 126 Sup1-5 14-26Document13 pages126 Sup1-5 14-26Affrida Nurlily Chintya WidariNo ratings yet
- Investigating Key Determinants of Childhood Diarrheal Incidence Among Patients at Hoima Regional Referral Hospital, Western UgandaDocument14 pagesInvestigating Key Determinants of Childhood Diarrheal Incidence Among Patients at Hoima Regional Referral Hospital, Western UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Significant Oral Cancer Risk Associated With Low Socioeconomic StatusDocument2 pagesSignificant Oral Cancer Risk Associated With Low Socioeconomic StatusWJNo ratings yet
- Management of Childhood Diarrhea by Healthcare Professionals in Low Income CountriesDocument40 pagesManagement of Childhood Diarrhea by Healthcare Professionals in Low Income CountriesrafaNo ratings yet
- Attitude Towards Infant Feeding Among Health Workers in Calabar, NigeriaDocument5 pagesAttitude Towards Infant Feeding Among Health Workers in Calabar, NigeriaogbanNo ratings yet
- International Journal of Nursing Studies: Tze-Fang Wang, Chiu-Mieh Huang, Chyuan Chou, Shu YuDocument7 pagesInternational Journal of Nursing Studies: Tze-Fang Wang, Chiu-Mieh Huang, Chyuan Chou, Shu YuRob21aNo ratings yet
- Optimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsFrom EverandOptimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsNo ratings yet
- Research Presentations of Dietetic Internship Participants: Research Proceedings - Nutrition and Food SectionFrom EverandResearch Presentations of Dietetic Internship Participants: Research Proceedings - Nutrition and Food SectionNo ratings yet
- Reducing Racial/Ethnic Disparities in Reproductive and Perinatal Outcomes: The Evidence from Population-Based InterventionsFrom EverandReducing Racial/Ethnic Disparities in Reproductive and Perinatal Outcomes: The Evidence from Population-Based InterventionsArden HandlerNo ratings yet
- Regulatory Alert Unbranded Enforcement - Digitas Health - May 2010Document2 pagesRegulatory Alert Unbranded Enforcement - Digitas Health - May 2010Dale CookeNo ratings yet
- National Leprosy Eradication Programme (Nlep)Document34 pagesNational Leprosy Eradication Programme (Nlep)Balaji KrishnanNo ratings yet
- Amphotericin B NephrotoxicityDocument30 pagesAmphotericin B Nephrotoxicitykhangsiean89No ratings yet
- Sustainable Development Is To Make A World A Better Place For Everyone Now Without Destroying The Possibilities For The Next Generations.Document3 pagesSustainable Development Is To Make A World A Better Place For Everyone Now Without Destroying The Possibilities For The Next Generations.rico molNo ratings yet
- Hospital AdministrationDocument39 pagesHospital AdministrationApriyanNo ratings yet
- Development of A Duplex Real-Time RT-PCR Assay For The Detection and Identification of Two Subgroups of Human Metapneumovirus in A Single TubeDocument7 pagesDevelopment of A Duplex Real-Time RT-PCR Assay For The Detection and Identification of Two Subgroups of Human Metapneumovirus in A Single Tubejan yerenaNo ratings yet
- Update Committee of The Whole CWD Ai 6-10-15 500373 7Document17 pagesUpdate Committee of The Whole CWD Ai 6-10-15 500373 7api-301405122No ratings yet
- PR Truenat WHO Endorsement 02072020Document4 pagesPR Truenat WHO Endorsement 02072020KantiNareshNo ratings yet
- Case StudyDocument7 pagesCase StudyElizabeth DaligdigNo ratings yet
- Assessment Nursing Diagnosis Goal Planning Implementation Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Goal Planning Implementation Rationale EvaluationRenju ThapaNo ratings yet
- 21 Test BankDocument17 pages21 Test BankNaNo ratings yet
- Theatre Operational PolicyDocument26 pagesTheatre Operational PolicyEmma Sunday OdyenyNo ratings yet
- Life Straw Community OverviewDocument19 pagesLife Straw Community OverviewMarton Gergely NagyNo ratings yet
- Colorectal CancerDocument23 pagesColorectal Cancerralph_gail100% (1)
- Prayer Is Essential and Integral To Rural Life and Its Approach To Health and IllnessDocument4 pagesPrayer Is Essential and Integral To Rural Life and Its Approach To Health and IllnessGasNo ratings yet
- Hernia: Information For PatientsDocument2 pagesHernia: Information For Patientsrianrifaldi123_98497No ratings yet
- Hemophilia: Supervisor: Dr. H. Hakimi, Sp.A (K)Document46 pagesHemophilia: Supervisor: Dr. H. Hakimi, Sp.A (K)Bima DwiNo ratings yet
- Chapter 12 Module AbuseDocument3 pagesChapter 12 Module AbuseCheetah Gemma0% (1)
- Chapter 103 PHCDocument47 pagesChapter 103 PHCYassir OunsaNo ratings yet
- Medtronic Gi Portfolio BrochureDocument10 pagesMedtronic Gi Portfolio BrochuremubaraknlhddNo ratings yet
- Nurses and ContractsDocument97 pagesNurses and ContractsJawadRasheedNo ratings yet
- Classification and Diagnosis of Hypertensive Disorders of PregnancyDocument6 pagesClassification and Diagnosis of Hypertensive Disorders of PregnancyZAHID AHMED KHANNo ratings yet
- Steps of Research ProcessDocument4 pagesSteps of Research ProcessSudeep SantraNo ratings yet
- The LDN Book, Volume Two - PrefaceDocument2 pagesThe LDN Book, Volume Two - PrefaceChelsea Green Publishing0% (1)
- UntitledDocument485 pagesUntitledsanthoshini b.sNo ratings yet
- Hospital Training ReportDocument27 pagesHospital Training ReportAdnan RAHAT50% (2)
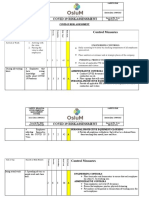
- COVID 19 Risk AssessmentDocument3 pagesCOVID 19 Risk AssessmentMajaga MabhenaNo ratings yet
- Msds Kaporit LiquidDocument3 pagesMsds Kaporit Liquidlius talithaNo ratings yet