
Log Sheet 2
Log Sheet 2
You might also like
- A Research Study On Attitude of Nurses Towards Relapse Prevention Among Psychiatric Patients in Federal Neuropsychiatric HospitalDocument66 pagesA Research Study On Attitude of Nurses Towards Relapse Prevention Among Psychiatric Patients in Federal Neuropsychiatric HospitalUsman Ahmad Tijjani100% (2)
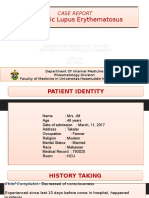
- Case Report SleDocument37 pagesCase Report SleUswah SudirmanNo ratings yet
- Dietetic Internship - Mini Case Study PowerpointDocument21 pagesDietetic Internship - Mini Case Study Powerpointapi-535934790No ratings yet
- Log Sheet 1Document4 pagesLog Sheet 1SHAFIQNo ratings yet
- Log Sheet 3Document4 pagesLog Sheet 3SHAFIQNo ratings yet
- Log Sheet 4Document4 pagesLog Sheet 4SHAFIQNo ratings yet
- Gross Painless Hematuria Bladder Irritability With Dysuria Frequency UrgencyDocument15 pagesGross Painless Hematuria Bladder Irritability With Dysuria Frequency UrgencyBrett FisherNo ratings yet
- Case 056: Common Bile Duct Stones (Choledocholithiasis)Document5 pagesCase 056: Common Bile Duct Stones (Choledocholithiasis)ZauzaNo ratings yet
- Pedia CPC For 2023Document3 pagesPedia CPC For 2023Parth VinaypatilNo ratings yet
- DK Endokrin 1 - Thyroid StormDocument37 pagesDK Endokrin 1 - Thyroid StormlaurachristianiNo ratings yet
- Patient Summary (A Case of Thyroid Storm) : by DR Adeyemo H.ADocument17 pagesPatient Summary (A Case of Thyroid Storm) : by DR Adeyemo H.AAdeyemoNo ratings yet
- MR - Suardi Tumor Paru + Efusi Pleura KiriDocument14 pagesMR - Suardi Tumor Paru + Efusi Pleura KiritiarapolarisiriuzNo ratings yet
- Sustained Tubulointerstitial Inflammation in Kidney With Severe LeptospirosisDocument6 pagesSustained Tubulointerstitial Inflammation in Kidney With Severe LeptospirosisKukuh WardahNo ratings yet
- PB Per Tanggal 3 November 2023Document2 pagesPB Per Tanggal 3 November 2023masitha yusmarNo ratings yet
- Problem Case: DR Bakhtawar Chandio Unit 1Document34 pagesProblem Case: DR Bakhtawar Chandio Unit 1Aijaz TalaniNo ratings yet
- Rahmatia Efusi PleuraDocument14 pagesRahmatia Efusi PleuraJuli2022 Semnol-SemsaNo ratings yet
- Mapping Aqsha 3 Senin, 08 November 2021Document10 pagesMapping Aqsha 3 Senin, 08 November 2021Febbby Mutia SafiraNo ratings yet
- Grand RoundDocument90 pagesGrand RoundMuhammad TalhahNo ratings yet
- DK IKA-5 Raymond - Intra Abdominal Tumor in 7-Y.o-Boy With Renal FailureDocument45 pagesDK IKA-5 Raymond - Intra Abdominal Tumor in 7-Y.o-Boy With Renal FailurepudjoNo ratings yet
- ErnawatiDocument13 pagesErnawatiSarahNo ratings yet
- Pomr Alul CKD SobDocument20 pagesPomr Alul CKD SobSeptabian IskandarNo ratings yet
- Liver Abscess Caused by Foreign BodyDocument5 pagesLiver Abscess Caused by Foreign BodyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Morbidity Meeting CT Icu (1) (1) - 2 3Document33 pagesMorbidity Meeting CT Icu (1) (1) - 2 3evaNo ratings yet
- Mortality-conference-2022.03.24 FINAL (自動儲存)Document51 pagesMortality-conference-2022.03.24 FINAL (自動儲存)許誌元No ratings yet
- DK Gastro KonsulDocument56 pagesDK Gastro Konsuldenina setyaNo ratings yet
- Intern ReportDocument7 pagesIntern ReportDLNo ratings yet
- Amprahan HCU Senin Sore, 27 November 2023Document8 pagesAmprahan HCU Senin Sore, 27 November 2023alfaz zamzamiNo ratings yet
- Complex Care Plan 1Document12 pagesComplex Care Plan 1api-496883420No ratings yet
- Duty Report Fanus CKDDocument5 pagesDuty Report Fanus CKDadelia putri wirandaniNo ratings yet
- Case Scenario Osteoarthritis Week 16 GerontologDocument5 pagesCase Scenario Osteoarthritis Week 16 GerontologMary Josette NavarraNo ratings yet
- Grand Round Final DraftDocument80 pagesGrand Round Final DraftBol Dhalbeny MalualNo ratings yet
- MR Arham EpgDocument12 pagesMR Arham Epgazraeni_629166196No ratings yet
- LAPHAR NEFRO 1 November 2022Document5 pagesLAPHAR NEFRO 1 November 2022dryubyNo ratings yet
- Nephrorounds3 2015final 150907110921 Lva1 App6892 PDFDocument133 pagesNephrorounds3 2015final 150907110921 Lva1 App6892 PDFTabada NickyNo ratings yet
- Parade Bedah SarafDocument15 pagesParade Bedah SarafStevent RichardoNo ratings yet
- Slide Ercp 29 MARET 2019Document92 pagesSlide Ercp 29 MARET 2019ariceghaNo ratings yet
- DK Gastro 2 - CA PankreasDocument111 pagesDK Gastro 2 - CA Pankreasdenina setyaNo ratings yet
- Alesha Potensial Respirator FailureDocument12 pagesAlesha Potensial Respirator FailureNina KristianiNo ratings yet
- DK Gastro EditDocument65 pagesDK Gastro Editdenina setyaNo ratings yet
- Morpot 21 April 2021 1Document11 pagesMorpot 21 April 2021 1pulmo unandNo ratings yet
- Final Myocarditis Associated With Influenzae A h1n1Document7 pagesFinal Myocarditis Associated With Influenzae A h1n1Dr Gaurav SinghNo ratings yet
- DK GastroDocument79 pagesDK Gastrodenina setyaNo ratings yet
- Case Presentation - Visceral LeishmaniaDocument18 pagesCase Presentation - Visceral LeishmaniaAAANo ratings yet
- Lung Lobe Torsion in Seven Juvenile DogsDocument7 pagesLung Lobe Torsion in Seven Juvenile DogsKelvinSueyzyNo ratings yet
- Case Protocol: General DataDocument3 pagesCase Protocol: General DataBryan GarmaNo ratings yet
- Multiple System Organ Failure/Multiple Organ Dysfunction SyndromeDocument14 pagesMultiple System Organ Failure/Multiple Organ Dysfunction SyndromemalathiNo ratings yet
- Multiple System Organ FailureDocument16 pagesMultiple System Organ Failurerefika rahmiNo ratings yet
- Er Morning Report Friday, March 8 2019 Er Morning Report Friday, March 8 2019Document12 pagesEr Morning Report Friday, March 8 2019 Er Morning Report Friday, March 8 2019Evan AninditoNo ratings yet
- Its Just HoaxDocument10 pagesIts Just HoaxArkhan HanafiNo ratings yet
- MR Drs Mustaking - Destroyed LungDocument16 pagesMR Drs Mustaking - Destroyed LungAFifah THamrinNo ratings yet
- Amprahan PICU Sabtu, 20 Feb 2021Document6 pagesAmprahan PICU Sabtu, 20 Feb 2021muhammadrikiNo ratings yet
- Case ScenariosDocument9 pagesCase ScenariosSophia IbuyanNo ratings yet
- Eu6690537362 35DD22C6Document3 pagesEu6690537362 35DD22C6avenger666666No ratings yet
- CLD With MeningitisDocument18 pagesCLD With MeningitisMhd AloofNo ratings yet
- MR Andi Maulida Timoma EditedDocument21 pagesMR Andi Maulida Timoma Editedazraeni_629166196No ratings yet
- CIS - Assignment 2Document3 pagesCIS - Assignment 2Crystal BNo ratings yet
- Nursing Care Plan: Student: PhạM Thu QuỳNh Group: 41 Class: Y4QDocument14 pagesNursing Care Plan: Student: PhạM Thu QuỳNh Group: 41 Class: Y4QThảo LÊNo ratings yet
- Acute AppendicitisDocument6 pagesAcute Appendicitiscuka suka jerpNo ratings yet
- Parade Plastik ReyDocument16 pagesParade Plastik ReyRano Digdayan MNo ratings yet
- PID L4-L5 (Case Study)Document67 pagesPID L4-L5 (Case Study)NannieNo ratings yet
- Log Sheet 4Document4 pagesLog Sheet 4SHAFIQNo ratings yet
- ENT Clinic SOAP NotesDocument3 pagesENT Clinic SOAP NotesSHAFIQNo ratings yet
- Log Sheet 3Document4 pagesLog Sheet 3SHAFIQNo ratings yet
- Pathophysiology For Adv Practice Course Grid August 2023Document13 pagesPathophysiology For Adv Practice Course Grid August 2023SHAFIQNo ratings yet
- Clinical Competency ChecklistDocument9 pagesClinical Competency ChecklistSHAFIQNo ratings yet
- Orthopedic SOAPDocument3 pagesOrthopedic SOAPSHAFIQNo ratings yet
- DRC Approval ProcessDocument1 pageDRC Approval ProcessSHAFIQNo ratings yet
- Thesis Award Flyer FinalDocument1 pageThesis Award Flyer FinalSHAFIQNo ratings yet
- Log Sheet 1Document4 pagesLog Sheet 1SHAFIQNo ratings yet
- Sorah Fatiha TarjumaDocument1 pageSorah Fatiha TarjumaSHAFIQNo ratings yet
- University of Health Sciences Lahore: Postgraduate Entrance Test 2020Document1 pageUniversity of Health Sciences Lahore: Postgraduate Entrance Test 2020SHAFIQNo ratings yet
- Assessment of Neoborn FinalDocument91 pagesAssessment of Neoborn FinalSHAFIQNo ratings yet
- DAS AppFormDocument5 pagesDAS AppFormSHAFIQNo ratings yet
- Ubaid Khan KmuDocument11 pagesUbaid Khan KmuSHAFIQNo ratings yet
- Musculoskeletal Disorders KMUDocument18 pagesMusculoskeletal Disorders KMUSHAFIQNo ratings yet
- Unit II Management Functions: by Group: 2 Sana Saleem Abrar Tariq Jamil Institute of Nursing Sciences, KMUDocument45 pagesUnit II Management Functions: by Group: 2 Sana Saleem Abrar Tariq Jamil Institute of Nursing Sciences, KMUSHAFIQNo ratings yet
- Antenatal Care: Presented byDocument36 pagesAntenatal Care: Presented bySHAFIQNo ratings yet
- Care of Child With Head InjuryDocument34 pagesCare of Child With Head InjurySHAFIQNo ratings yet
- Fluids & Electrolytes Imbalance KMUDocument37 pagesFluids & Electrolytes Imbalance KMUSHAFIQNo ratings yet
- Pediatric Health Nursing Unit I BSN Year III, Semester V: by Hidayatullah Khan BSN, DPN & MSN Kmu-InsDocument59 pagesPediatric Health Nursing Unit I BSN Year III, Semester V: by Hidayatullah Khan BSN, DPN & MSN Kmu-InsSHAFIQNo ratings yet
- Kmu Therapeutic Play & CommunicationDocument26 pagesKmu Therapeutic Play & CommunicationSHAFIQNo ratings yet
- KMU Blood DisorderDocument43 pagesKMU Blood DisorderSHAFIQNo ratings yet
- Unit IV Power & Politics in NursingDocument18 pagesUnit IV Power & Politics in NursingSHAFIQNo ratings yet
- Unit II Pathophysiology of CVS: by Hidayat Khan KMUDocument17 pagesUnit II Pathophysiology of CVS: by Hidayat Khan KMUSHAFIQNo ratings yet
- Health Management Information SystemDocument7 pagesHealth Management Information SystemSHAFIQNo ratings yet
- Environmental Health: by Mr. Imran Yousafzai BSN (Pak), MSPH (Pak), PGHRHM (UK), MHPE (Pak)Document43 pagesEnvironmental Health: by Mr. Imran Yousafzai BSN (Pak), MSPH (Pak), PGHRHM (UK), MHPE (Pak)SHAFIQNo ratings yet
- Haider Ali CHN PaperDocument9 pagesHaider Ali CHN PaperSHAFIQ0% (2)
- Demography/Global Health & Health TransitionDocument22 pagesDemography/Global Health & Health TransitionSHAFIQNo ratings yet
- Community Health Nurseing Unit1Document34 pagesCommunity Health Nurseing Unit1SHAFIQ100% (1)
- HashmatDocument9 pagesHashmatSHAFIQNo ratings yet
- Unit 7 ListeningDocument41 pagesUnit 7 ListeningHo NgocthuNo ratings yet
- Atharva Dilip Chandurkar Birth CertifDocument1 pageAtharva Dilip Chandurkar Birth CertifMd Usman KhanNo ratings yet
- Florin Bzovii Abstract enDocument38 pagesFlorin Bzovii Abstract enVasile Pogor ISNo ratings yet
- Ethical Issues Involved in Online Counseling: Practitioners' CornerDocument13 pagesEthical Issues Involved in Online Counseling: Practitioners' CornerabcdNo ratings yet
- Physical Fitness Tulad NG NatukoyDocument5 pagesPhysical Fitness Tulad NG NatukoyElma SilvestreNo ratings yet
- School-Life Balance The Aftermath of Teenage Pregnancy PhenomenonDocument15 pagesSchool-Life Balance The Aftermath of Teenage Pregnancy PhenomenonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Sex EducationDocument2 pagesSex EducationsumitchaudharydungerNo ratings yet
- Herd Health ManagementDocument4 pagesHerd Health Managementdennis jay paglinawanNo ratings yet
- Introduction To Operations Management: Utdallas - Edu/ MetinDocument28 pagesIntroduction To Operations Management: Utdallas - Edu/ Metinalisnowkiss6570No ratings yet
- Inventory FormDocument1 pageInventory FormYanexAlfzNo ratings yet
- TestoriDocument7 pagesTestoriGgNo ratings yet
- FC6W51 Work Related Learning (WRL) Form: StudentDocument4 pagesFC6W51 Work Related Learning (WRL) Form: StudentSanjog ChoudharyNo ratings yet
- Inclusion Self Assessment - Plan InternationalDocument6 pagesInclusion Self Assessment - Plan InternationalFatima RifaiNo ratings yet
- Week-1-7 CM MDL SSC111Document50 pagesWeek-1-7 CM MDL SSC111Eric DeocampoNo ratings yet
- ID Pengaruh Terapi Antituberkulosis TerhadaDocument11 pagesID Pengaruh Terapi Antituberkulosis TerhadaFarraNo ratings yet
- Occurrence and Factors Predisposing To Under Nutrition Among Children Under Five Years Attending KIUTH Bushenyi District, UgandaDocument10 pagesOccurrence and Factors Predisposing To Under Nutrition Among Children Under Five Years Attending KIUTH Bushenyi District, UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Sample College Personal Statement EssaysDocument9 pagesSample College Personal Statement Essaysafabkgddu100% (2)
- Calgo Renzel NCPDocument1 pageCalgo Renzel NCPRenzel Ross CalgoNo ratings yet
- 2016 Ashby PTSD After Sexual Abuse in Adolescent GirlsDocument6 pages2016 Ashby PTSD After Sexual Abuse in Adolescent GirlsNoelia González CousidoNo ratings yet
- Adult and Elder I. Nursing Care PlanDocument6 pagesAdult and Elder I. Nursing Care PlanteresapazNo ratings yet
- Automatic Segmentation of Cervical Cells in Pap Smear ImagesDocument7 pagesAutomatic Segmentation of Cervical Cells in Pap Smear ImagesSàkâtã ÁbéŕàNo ratings yet
- IPD - KardiologiDocument124 pagesIPD - KardiologiAnis BonitaNo ratings yet
- PSC Reopening and Recovery Back To Work Checklist (Final - April 20, 2020)Document6 pagesPSC Reopening and Recovery Back To Work Checklist (Final - April 20, 2020)WWMT100% (1)
- HMD Kojak SelingeDocument2 pagesHMD Kojak SelingeHMD Healthcare100% (1)
- Department of Education: Action Plan On Ok Sa DepedDocument11 pagesDepartment of Education: Action Plan On Ok Sa DepedCharry Mae CacabanNo ratings yet
- 2567-Article Text-15164-1-10-20230808Document14 pages2567-Article Text-15164-1-10-20230808reyhanfabian268No ratings yet
- Fire Safety Management Strategy in Nigeria Public BuildingsDocument9 pagesFire Safety Management Strategy in Nigeria Public BuildingsWaskita Paspro Seksi 4No ratings yet
- Docu Intro. Table Ppprobgroup1Document50 pagesDocu Intro. Table Ppprobgroup1Abegail PolicarpioNo ratings yet
- Confounding VariableDocument3 pagesConfounding VariableTefera AsresNo ratings yet


















































































































Download as docx, pdf, or txt
You might also like
- A Research Study On Attitude of Nurses Towards Relapse Prevention Among Psychiatric Patients in Federal Neuropsychiatric HospitalDocument66 pagesA Research Study On Attitude of Nurses Towards Relapse Prevention Among Psychiatric Patients in Federal Neuropsychiatric HospitalUsman Ahmad Tijjani100% (2)
- Case Report SleDocument37 pagesCase Report SleUswah SudirmanNo ratings yet
- Dietetic Internship - Mini Case Study PowerpointDocument21 pagesDietetic Internship - Mini Case Study Powerpointapi-535934790No ratings yet
- Log Sheet 1Document4 pagesLog Sheet 1SHAFIQNo ratings yet
- Log Sheet 3Document4 pagesLog Sheet 3SHAFIQNo ratings yet
- Log Sheet 4Document4 pagesLog Sheet 4SHAFIQNo ratings yet
- Gross Painless Hematuria Bladder Irritability With Dysuria Frequency UrgencyDocument15 pagesGross Painless Hematuria Bladder Irritability With Dysuria Frequency UrgencyBrett FisherNo ratings yet
- Case 056: Common Bile Duct Stones (Choledocholithiasis)Document5 pagesCase 056: Common Bile Duct Stones (Choledocholithiasis)ZauzaNo ratings yet
- Pedia CPC For 2023Document3 pagesPedia CPC For 2023Parth VinaypatilNo ratings yet
- DK Endokrin 1 - Thyroid StormDocument37 pagesDK Endokrin 1 - Thyroid StormlaurachristianiNo ratings yet
- Patient Summary (A Case of Thyroid Storm) : by DR Adeyemo H.ADocument17 pagesPatient Summary (A Case of Thyroid Storm) : by DR Adeyemo H.AAdeyemoNo ratings yet
- MR - Suardi Tumor Paru + Efusi Pleura KiriDocument14 pagesMR - Suardi Tumor Paru + Efusi Pleura KiritiarapolarisiriuzNo ratings yet
- Sustained Tubulointerstitial Inflammation in Kidney With Severe LeptospirosisDocument6 pagesSustained Tubulointerstitial Inflammation in Kidney With Severe LeptospirosisKukuh WardahNo ratings yet
- PB Per Tanggal 3 November 2023Document2 pagesPB Per Tanggal 3 November 2023masitha yusmarNo ratings yet
- Problem Case: DR Bakhtawar Chandio Unit 1Document34 pagesProblem Case: DR Bakhtawar Chandio Unit 1Aijaz TalaniNo ratings yet
- Rahmatia Efusi PleuraDocument14 pagesRahmatia Efusi PleuraJuli2022 Semnol-SemsaNo ratings yet
- Mapping Aqsha 3 Senin, 08 November 2021Document10 pagesMapping Aqsha 3 Senin, 08 November 2021Febbby Mutia SafiraNo ratings yet
- Grand RoundDocument90 pagesGrand RoundMuhammad TalhahNo ratings yet
- DK IKA-5 Raymond - Intra Abdominal Tumor in 7-Y.o-Boy With Renal FailureDocument45 pagesDK IKA-5 Raymond - Intra Abdominal Tumor in 7-Y.o-Boy With Renal FailurepudjoNo ratings yet
- ErnawatiDocument13 pagesErnawatiSarahNo ratings yet
- Pomr Alul CKD SobDocument20 pagesPomr Alul CKD SobSeptabian IskandarNo ratings yet
- Liver Abscess Caused by Foreign BodyDocument5 pagesLiver Abscess Caused by Foreign BodyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Morbidity Meeting CT Icu (1) (1) - 2 3Document33 pagesMorbidity Meeting CT Icu (1) (1) - 2 3evaNo ratings yet
- Mortality-conference-2022.03.24 FINAL (自動儲存)Document51 pagesMortality-conference-2022.03.24 FINAL (自動儲存)許誌元No ratings yet
- DK Gastro KonsulDocument56 pagesDK Gastro Konsuldenina setyaNo ratings yet
- Intern ReportDocument7 pagesIntern ReportDLNo ratings yet
- Amprahan HCU Senin Sore, 27 November 2023Document8 pagesAmprahan HCU Senin Sore, 27 November 2023alfaz zamzamiNo ratings yet
- Complex Care Plan 1Document12 pagesComplex Care Plan 1api-496883420No ratings yet
- Duty Report Fanus CKDDocument5 pagesDuty Report Fanus CKDadelia putri wirandaniNo ratings yet
- Case Scenario Osteoarthritis Week 16 GerontologDocument5 pagesCase Scenario Osteoarthritis Week 16 GerontologMary Josette NavarraNo ratings yet
- Grand Round Final DraftDocument80 pagesGrand Round Final DraftBol Dhalbeny MalualNo ratings yet
- MR Arham EpgDocument12 pagesMR Arham Epgazraeni_629166196No ratings yet
- LAPHAR NEFRO 1 November 2022Document5 pagesLAPHAR NEFRO 1 November 2022dryubyNo ratings yet
- Nephrorounds3 2015final 150907110921 Lva1 App6892 PDFDocument133 pagesNephrorounds3 2015final 150907110921 Lva1 App6892 PDFTabada NickyNo ratings yet
- Parade Bedah SarafDocument15 pagesParade Bedah SarafStevent RichardoNo ratings yet
- Slide Ercp 29 MARET 2019Document92 pagesSlide Ercp 29 MARET 2019ariceghaNo ratings yet
- DK Gastro 2 - CA PankreasDocument111 pagesDK Gastro 2 - CA Pankreasdenina setyaNo ratings yet
- Alesha Potensial Respirator FailureDocument12 pagesAlesha Potensial Respirator FailureNina KristianiNo ratings yet
- DK Gastro EditDocument65 pagesDK Gastro Editdenina setyaNo ratings yet
- Morpot 21 April 2021 1Document11 pagesMorpot 21 April 2021 1pulmo unandNo ratings yet
- Final Myocarditis Associated With Influenzae A h1n1Document7 pagesFinal Myocarditis Associated With Influenzae A h1n1Dr Gaurav SinghNo ratings yet
- DK GastroDocument79 pagesDK Gastrodenina setyaNo ratings yet
- Case Presentation - Visceral LeishmaniaDocument18 pagesCase Presentation - Visceral LeishmaniaAAANo ratings yet
- Lung Lobe Torsion in Seven Juvenile DogsDocument7 pagesLung Lobe Torsion in Seven Juvenile DogsKelvinSueyzyNo ratings yet
- Case Protocol: General DataDocument3 pagesCase Protocol: General DataBryan GarmaNo ratings yet
- Multiple System Organ Failure/Multiple Organ Dysfunction SyndromeDocument14 pagesMultiple System Organ Failure/Multiple Organ Dysfunction SyndromemalathiNo ratings yet
- Multiple System Organ FailureDocument16 pagesMultiple System Organ Failurerefika rahmiNo ratings yet
- Er Morning Report Friday, March 8 2019 Er Morning Report Friday, March 8 2019Document12 pagesEr Morning Report Friday, March 8 2019 Er Morning Report Friday, March 8 2019Evan AninditoNo ratings yet
- Its Just HoaxDocument10 pagesIts Just HoaxArkhan HanafiNo ratings yet
- MR Drs Mustaking - Destroyed LungDocument16 pagesMR Drs Mustaking - Destroyed LungAFifah THamrinNo ratings yet
- Amprahan PICU Sabtu, 20 Feb 2021Document6 pagesAmprahan PICU Sabtu, 20 Feb 2021muhammadrikiNo ratings yet
- Case ScenariosDocument9 pagesCase ScenariosSophia IbuyanNo ratings yet
- Eu6690537362 35DD22C6Document3 pagesEu6690537362 35DD22C6avenger666666No ratings yet
- CLD With MeningitisDocument18 pagesCLD With MeningitisMhd AloofNo ratings yet
- MR Andi Maulida Timoma EditedDocument21 pagesMR Andi Maulida Timoma Editedazraeni_629166196No ratings yet
- CIS - Assignment 2Document3 pagesCIS - Assignment 2Crystal BNo ratings yet
- Nursing Care Plan: Student: PhạM Thu QuỳNh Group: 41 Class: Y4QDocument14 pagesNursing Care Plan: Student: PhạM Thu QuỳNh Group: 41 Class: Y4QThảo LÊNo ratings yet
- Acute AppendicitisDocument6 pagesAcute Appendicitiscuka suka jerpNo ratings yet
- Parade Plastik ReyDocument16 pagesParade Plastik ReyRano Digdayan MNo ratings yet
- PID L4-L5 (Case Study)Document67 pagesPID L4-L5 (Case Study)NannieNo ratings yet
- Log Sheet 4Document4 pagesLog Sheet 4SHAFIQNo ratings yet
- ENT Clinic SOAP NotesDocument3 pagesENT Clinic SOAP NotesSHAFIQNo ratings yet
- Log Sheet 3Document4 pagesLog Sheet 3SHAFIQNo ratings yet
- Pathophysiology For Adv Practice Course Grid August 2023Document13 pagesPathophysiology For Adv Practice Course Grid August 2023SHAFIQNo ratings yet
- Clinical Competency ChecklistDocument9 pagesClinical Competency ChecklistSHAFIQNo ratings yet
- Orthopedic SOAPDocument3 pagesOrthopedic SOAPSHAFIQNo ratings yet
- DRC Approval ProcessDocument1 pageDRC Approval ProcessSHAFIQNo ratings yet
- Thesis Award Flyer FinalDocument1 pageThesis Award Flyer FinalSHAFIQNo ratings yet
- Log Sheet 1Document4 pagesLog Sheet 1SHAFIQNo ratings yet
- Sorah Fatiha TarjumaDocument1 pageSorah Fatiha TarjumaSHAFIQNo ratings yet
- University of Health Sciences Lahore: Postgraduate Entrance Test 2020Document1 pageUniversity of Health Sciences Lahore: Postgraduate Entrance Test 2020SHAFIQNo ratings yet
- Assessment of Neoborn FinalDocument91 pagesAssessment of Neoborn FinalSHAFIQNo ratings yet
- DAS AppFormDocument5 pagesDAS AppFormSHAFIQNo ratings yet
- Ubaid Khan KmuDocument11 pagesUbaid Khan KmuSHAFIQNo ratings yet
- Musculoskeletal Disorders KMUDocument18 pagesMusculoskeletal Disorders KMUSHAFIQNo ratings yet
- Unit II Management Functions: by Group: 2 Sana Saleem Abrar Tariq Jamil Institute of Nursing Sciences, KMUDocument45 pagesUnit II Management Functions: by Group: 2 Sana Saleem Abrar Tariq Jamil Institute of Nursing Sciences, KMUSHAFIQNo ratings yet
- Antenatal Care: Presented byDocument36 pagesAntenatal Care: Presented bySHAFIQNo ratings yet
- Care of Child With Head InjuryDocument34 pagesCare of Child With Head InjurySHAFIQNo ratings yet
- Fluids & Electrolytes Imbalance KMUDocument37 pagesFluids & Electrolytes Imbalance KMUSHAFIQNo ratings yet
- Pediatric Health Nursing Unit I BSN Year III, Semester V: by Hidayatullah Khan BSN, DPN & MSN Kmu-InsDocument59 pagesPediatric Health Nursing Unit I BSN Year III, Semester V: by Hidayatullah Khan BSN, DPN & MSN Kmu-InsSHAFIQNo ratings yet
- Kmu Therapeutic Play & CommunicationDocument26 pagesKmu Therapeutic Play & CommunicationSHAFIQNo ratings yet
- KMU Blood DisorderDocument43 pagesKMU Blood DisorderSHAFIQNo ratings yet
- Unit IV Power & Politics in NursingDocument18 pagesUnit IV Power & Politics in NursingSHAFIQNo ratings yet
- Unit II Pathophysiology of CVS: by Hidayat Khan KMUDocument17 pagesUnit II Pathophysiology of CVS: by Hidayat Khan KMUSHAFIQNo ratings yet
- Health Management Information SystemDocument7 pagesHealth Management Information SystemSHAFIQNo ratings yet
- Environmental Health: by Mr. Imran Yousafzai BSN (Pak), MSPH (Pak), PGHRHM (UK), MHPE (Pak)Document43 pagesEnvironmental Health: by Mr. Imran Yousafzai BSN (Pak), MSPH (Pak), PGHRHM (UK), MHPE (Pak)SHAFIQNo ratings yet
- Haider Ali CHN PaperDocument9 pagesHaider Ali CHN PaperSHAFIQ0% (2)
- Demography/Global Health & Health TransitionDocument22 pagesDemography/Global Health & Health TransitionSHAFIQNo ratings yet
- Community Health Nurseing Unit1Document34 pagesCommunity Health Nurseing Unit1SHAFIQ100% (1)
- HashmatDocument9 pagesHashmatSHAFIQNo ratings yet
- Unit 7 ListeningDocument41 pagesUnit 7 ListeningHo NgocthuNo ratings yet
- Atharva Dilip Chandurkar Birth CertifDocument1 pageAtharva Dilip Chandurkar Birth CertifMd Usman KhanNo ratings yet
- Florin Bzovii Abstract enDocument38 pagesFlorin Bzovii Abstract enVasile Pogor ISNo ratings yet
- Ethical Issues Involved in Online Counseling: Practitioners' CornerDocument13 pagesEthical Issues Involved in Online Counseling: Practitioners' CornerabcdNo ratings yet
- Physical Fitness Tulad NG NatukoyDocument5 pagesPhysical Fitness Tulad NG NatukoyElma SilvestreNo ratings yet
- School-Life Balance The Aftermath of Teenage Pregnancy PhenomenonDocument15 pagesSchool-Life Balance The Aftermath of Teenage Pregnancy PhenomenonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Sex EducationDocument2 pagesSex EducationsumitchaudharydungerNo ratings yet
- Herd Health ManagementDocument4 pagesHerd Health Managementdennis jay paglinawanNo ratings yet
- Introduction To Operations Management: Utdallas - Edu/ MetinDocument28 pagesIntroduction To Operations Management: Utdallas - Edu/ Metinalisnowkiss6570No ratings yet
- Inventory FormDocument1 pageInventory FormYanexAlfzNo ratings yet
- TestoriDocument7 pagesTestoriGgNo ratings yet
- FC6W51 Work Related Learning (WRL) Form: StudentDocument4 pagesFC6W51 Work Related Learning (WRL) Form: StudentSanjog ChoudharyNo ratings yet
- Inclusion Self Assessment - Plan InternationalDocument6 pagesInclusion Self Assessment - Plan InternationalFatima RifaiNo ratings yet
- Week-1-7 CM MDL SSC111Document50 pagesWeek-1-7 CM MDL SSC111Eric DeocampoNo ratings yet
- ID Pengaruh Terapi Antituberkulosis TerhadaDocument11 pagesID Pengaruh Terapi Antituberkulosis TerhadaFarraNo ratings yet
- Occurrence and Factors Predisposing To Under Nutrition Among Children Under Five Years Attending KIUTH Bushenyi District, UgandaDocument10 pagesOccurrence and Factors Predisposing To Under Nutrition Among Children Under Five Years Attending KIUTH Bushenyi District, UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Sample College Personal Statement EssaysDocument9 pagesSample College Personal Statement Essaysafabkgddu100% (2)
- Calgo Renzel NCPDocument1 pageCalgo Renzel NCPRenzel Ross CalgoNo ratings yet
- 2016 Ashby PTSD After Sexual Abuse in Adolescent GirlsDocument6 pages2016 Ashby PTSD After Sexual Abuse in Adolescent GirlsNoelia González CousidoNo ratings yet
- Adult and Elder I. Nursing Care PlanDocument6 pagesAdult and Elder I. Nursing Care PlanteresapazNo ratings yet
- Automatic Segmentation of Cervical Cells in Pap Smear ImagesDocument7 pagesAutomatic Segmentation of Cervical Cells in Pap Smear ImagesSàkâtã ÁbéŕàNo ratings yet
- IPD - KardiologiDocument124 pagesIPD - KardiologiAnis BonitaNo ratings yet
- PSC Reopening and Recovery Back To Work Checklist (Final - April 20, 2020)Document6 pagesPSC Reopening and Recovery Back To Work Checklist (Final - April 20, 2020)WWMT100% (1)
- HMD Kojak SelingeDocument2 pagesHMD Kojak SelingeHMD Healthcare100% (1)
- Department of Education: Action Plan On Ok Sa DepedDocument11 pagesDepartment of Education: Action Plan On Ok Sa DepedCharry Mae CacabanNo ratings yet
- 2567-Article Text-15164-1-10-20230808Document14 pages2567-Article Text-15164-1-10-20230808reyhanfabian268No ratings yet
- Fire Safety Management Strategy in Nigeria Public BuildingsDocument9 pagesFire Safety Management Strategy in Nigeria Public BuildingsWaskita Paspro Seksi 4No ratings yet
- Docu Intro. Table Ppprobgroup1Document50 pagesDocu Intro. Table Ppprobgroup1Abegail PolicarpioNo ratings yet
- Confounding VariableDocument3 pagesConfounding VariableTefera AsresNo ratings yet