Download as pdf or txt
You might also like
- Utilizing Free Skin Grafts in The Repair of Surgical Wounds: Madalene C. Y. HengDocument11 pagesUtilizing Free Skin Grafts in The Repair of Surgical Wounds: Madalene C. Y. HengDefri ChanNo ratings yet
- Acne Scars: Subcision: Methods and TechniquesDocument3 pagesAcne Scars: Subcision: Methods and TechniquesLuiz Henrique CararetoNo ratings yet
- AnnMaxillofacSurg62204-7504388 020504Document6 pagesAnnMaxillofacSurg62204-7504388 020504mascoNo ratings yet
- Removal of Salivary Gland Mucocele Using 980Nm Diode Laser: Case ReportDocument3 pagesRemoval of Salivary Gland Mucocele Using 980Nm Diode Laser: Case Reportmaya morenoNo ratings yet
- Multiple Adjacent Gingival Recessions: Which Technique To Use, Tunnel or Flap?Document8 pagesMultiple Adjacent Gingival Recessions: Which Technique To Use, Tunnel or Flap?oliverglezNo ratings yet
- 2014 Article 1741Document4 pages2014 Article 1741anton suponoNo ratings yet
- Original Article: Farideh Nejat, Nima Baradaran, Mostafa El KhashabDocument4 pagesOriginal Article: Farideh Nejat, Nima Baradaran, Mostafa El KhashabGuz CaemmNo ratings yet
- Subcision 40 PatientsDocument8 pagesSubcision 40 Patientsxj112358No ratings yet
- Modified Rhomboid Flap For Facial ReconstructionDocument3 pagesModified Rhomboid Flap For Facial ReconstructionahujasurajNo ratings yet
- Reconstrucción Defectos Nasales PDFDocument18 pagesReconstrucción Defectos Nasales PDFSara OmNo ratings yet
- Gox 5 E1230Document6 pagesGox 5 E1230Brînduşa CiobanuNo ratings yet
- Biopsy Techniques Diagnosis of Melanoma: Neil A. Swanson, MD, Ken K. Lee, MD, Annalisa Gorman, MD, Han N. Lee, MDDocument4 pagesBiopsy Techniques Diagnosis of Melanoma: Neil A. Swanson, MD, Ken K. Lee, MD, Annalisa Gorman, MD, Han N. Lee, MDdaniel satyoNo ratings yet
- Basal Cell Carcinoma: General FeaturesDocument5 pagesBasal Cell Carcinoma: General FeaturesSel ViaNo ratings yet
- AnnMaxillofacSurg 2020 10 1 182 286169Document5 pagesAnnMaxillofacSurg 2020 10 1 182 286169pratiksha malhotraNo ratings yet
- Reconstruction After Skin Cancer Removal: More Than Just "Filling A Hole"Document2 pagesReconstruction After Skin Cancer Removal: More Than Just "Filling A Hole"irsalinahusnaNo ratings yet
- Carbuncle Excision TechniqueDocument3 pagesCarbuncle Excision TechniquetseeckunNo ratings yet
- Aesth Plast Surg - 2019 - 43 - 652-657Document6 pagesAesth Plast Surg - 2019 - 43 - 652-657HemerobibliotecaHospitalNo ratings yet
- Comparing Cannula Based Subcision With The Common Needle Method: A Clinical TrialDocument7 pagesComparing Cannula Based Subcision With The Common Needle Method: A Clinical Trial郭先薈No ratings yet
- Lembi CutaneiDocument6 pagesLembi CutaneiGianfranco MuntoniNo ratings yet
- Subcision de CicatrizDocument2 pagesSubcision de CicatrizGaviota75No ratings yet
- Basis of Dimple CreationDocument6 pagesBasis of Dimple Creationkusuma rNo ratings yet
- Simple Technique For Facial DimpleDocument4 pagesSimple Technique For Facial DimpleAdi WijayantoNo ratings yet
- Closure of Defects of The Malar Region: Mehmet Mutaf, MD, Ertan Gu Nal, MD, and Metin Temel, MDDocument4 pagesClosure of Defects of The Malar Region: Mehmet Mutaf, MD, Ertan Gu Nal, MD, and Metin Temel, MDgokhanNo ratings yet
- Surgical Eye ProceduresDocument4 pagesSurgical Eye ProceduresLeonela SánchezNo ratings yet
- 5phase II Periodontal TherapyDocument54 pages5phase II Periodontal TherapyKaraz StudiosNo ratings yet
- Art:10.1007/s00266 013 0134 0Document10 pagesArt:10.1007/s00266 013 0134 0FabianaNisanNo ratings yet
- Review Article: Skin GraftDocument6 pagesReview Article: Skin Graftfitri dwi astutiNo ratings yet
- Procedimientos Vulva PDFDocument14 pagesProcedimientos Vulva PDFTheodoraAlinaNo ratings yet
- Surgical Technique For Optimal OutcomesDocument11 pagesSurgical Technique For Optimal OutcomesAndrei EncisoNo ratings yet
- Tilleman 2004Document7 pagesTilleman 2004이호원No ratings yet
- Complications of Strabismus Surgery: DellenDocument14 pagesComplications of Strabismus Surgery: DellenDeny Rahmat PamungkasNo ratings yet
- Fascia Suspension Lift A Facelift Technique Without Skin Excision andDocument10 pagesFascia Suspension Lift A Facelift Technique Without Skin Excision and7rayosomonishangoNo ratings yet
- In Vivo Intraoral Reflectance Confocal Microscopy of An Amalgam TattooDocument4 pagesIn Vivo Intraoral Reflectance Confocal Microscopy of An Amalgam TattooEndah AzNo ratings yet
- Wire Subcision For Complete Release of Depressions, Subdermal Attachments, and ScarsDocument8 pagesWire Subcision For Complete Release of Depressions, Subdermal Attachments, and ScarsLuciano AbbaNo ratings yet
- Anatomy of The Skin and The Pathogenesis of Nonmelanoma Skin CancerDocument4 pagesAnatomy of The Skin and The Pathogenesis of Nonmelanoma Skin CancerariskaNo ratings yet
- Research Microneedling in DermatologyDocument10 pagesResearch Microneedling in DermatologyErik BrooksNo ratings yet
- Incision and DrainageDocument35 pagesIncision and DrainageVilma Delos Reyes100% (1)
- Plastic Surgery: Pablo L. Padilla, Kimberly H. Khoo, Trung Ho, Eric L. Cole, Ramón Zapata Sirvent, Linda G. PhillipsDocument29 pagesPlastic Surgery: Pablo L. Padilla, Kimberly H. Khoo, Trung Ho, Eric L. Cole, Ramón Zapata Sirvent, Linda G. Phillipssportillag1No ratings yet
- Vulvar ProceduresDocument14 pagesVulvar Proceduresjft842No ratings yet
- Bille Et Al 2019Document5 pagesBille Et Al 2019Walid SasiNo ratings yet
- Crawley 2015Document6 pagesCrawley 2015Eduardo HernándezNo ratings yet
- Jurnal Scar RevisionDocument8 pagesJurnal Scar Revisionnurul rezki fitrianiazisNo ratings yet
- Two Advancement Flaps For Eyelid Margin Reconstruction of Small and Medium Defects and A Novel Design To Reduce Ocular InjuryDocument13 pagesTwo Advancement Flaps For Eyelid Margin Reconstruction of Small and Medium Defects and A Novel Design To Reduce Ocular InjuryhilderhNo ratings yet
- Short Scar Rhytidectomy Tech 2014 Atlas of The Oral and Maxillofacial SurgerDocument16 pagesShort Scar Rhytidectomy Tech 2014 Atlas of The Oral and Maxillofacial Surgerlaljadeff12No ratings yet
- Efficacy of Microneedling With 70% Glycolic Acid PeelDocument6 pagesEfficacy of Microneedling With 70% Glycolic Acid PeelHanna NabilaNo ratings yet
- Djohan2010bening&malignan TumorDocument13 pagesDjohan2010bening&malignan Tumorkiki0% (1)
- A Safe Nonsurgical Rhinoplasty ProcedureDocument5 pagesA Safe Nonsurgical Rhinoplasty ProcedureKerlida SantosNo ratings yet
- Jkms 29 751 PDFDocument7 pagesJkms 29 751 PDFalexander nezwyNo ratings yet
- Rugas de Acordeon 2012Document10 pagesRugas de Acordeon 2012Dr. Frederico NevesNo ratings yet
- Artificial Neural Network For Skincancer DetectionDocument7 pagesArtificial Neural Network For Skincancer DetectionInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- Descemet Membrane Detachment During Cataract Surgery: Etiology and ManagementDocument7 pagesDescemet Membrane Detachment During Cataract Surgery: Etiology and Managementjorge vegaNo ratings yet
- Mingival Curettage PDFDocument52 pagesMingival Curettage PDFheycoolalexNo ratings yet
- Capítulo 10 SerdevDocument19 pagesCapítulo 10 SerdevErik BrooksNo ratings yet
- Oralmucocele AcasereportDocument5 pagesOralmucocele AcasereportxxxNo ratings yet
- 64 - Skin TumorsDocument20 pages64 - Skin TumorsAlexa GabrielaNo ratings yet
- Sadick 2018Document13 pagesSadick 2018IrsalinaHusnaAzwirNo ratings yet
- Unique Clinical Aspects of Nasal ScarringDocument10 pagesUnique Clinical Aspects of Nasal ScarringKerlida SantosNo ratings yet
- DM2022 8705436Document6 pagesDM2022 8705436MufassiraturrahmahNo ratings yet
- Oculoplastic Surgery: A Practical Guide to Common DisordersFrom EverandOculoplastic Surgery: A Practical Guide to Common DisordersEssam A. El ToukhyNo ratings yet
- Sandeep Kodali ppk-2Document6 pagesSandeep Kodali ppk-2kahkashanahmed065No ratings yet
- DownloadDocument9 pagesDownloadkahkashanahmed065No ratings yet
- DIR Summer 2023 BF Atypical FibroxanthomaDocument2 pagesDIR Summer 2023 BF Atypical Fibroxanthomakahkashanahmed065No ratings yet
- Facial Anatomy and The Application of Fillers andDocument12 pagesFacial Anatomy and The Application of Fillers andkahkashanahmed065No ratings yet
- AAD BF Chemotherapy Specific Cutaneous ReactionsDocument3 pagesAAD BF Chemotherapy Specific Cutaneous Reactionskahkashanahmed065No ratings yet
- Quiz Review Exam ETASDocument183 pagesQuiz Review Exam ETASkahkashanahmed065No ratings yet
- AAD BF Head and Neck Lesions InfantDocument2 pagesAAD BF Head and Neck Lesions Infantkahkashanahmed065No ratings yet
- AAD BF Non TB Cutaneous Mycobact InfectionsDocument3 pagesAAD BF Non TB Cutaneous Mycobact Infectionskahkashanahmed065No ratings yet
- AAD BF Paisley Tie DiagnosisDocument2 pagesAAD BF Paisley Tie Diagnosiskahkashanahmed065No ratings yet
- DIR Fall 2023 BF Ticks ONLINEDocument3 pagesDIR Fall 2023 BF Ticks ONLINEkahkashanahmed065No ratings yet
- AAD BF Retinoid Biology 2Document2 pagesAAD BF Retinoid Biology 2kahkashanahmed065No ratings yet
- Female Androgenetic Alopecia A Risk Factor For.4Document6 pagesFemale Androgenetic Alopecia A Risk Factor For.4kahkashanahmed065No ratings yet
- RoutledgesManualofEtiquette 10001646Document264 pagesRoutledgesManualofEtiquette 10001646kahkashanahmed065No ratings yet
- AAD BF Bones Eyes NailsDocument5 pagesAAD BF Bones Eyes Nailskahkashanahmed065No ratings yet
- AAD BF Herbal Supplements in DermatologyDocument2 pagesAAD BF Herbal Supplements in Dermatologykahkashanahmed065No ratings yet
- AAD BF Cutaneous Mycobact Infections PDFDocument3 pagesAAD BF Cutaneous Mycobact Infections PDFkahkashanahmed065No ratings yet
- AAD BF Cutaneous Manifestations of HIV InfectionsDocument2 pagesAAD BF Cutaneous Manifestations of HIV Infectionskahkashanahmed065No ratings yet
- Etas 2022-1Document1,135 pagesEtas 2022-1kahkashanahmed065No ratings yet
- AAD BF HistiocytosisDocument2 pagesAAD BF Histiocytosiskahkashanahmed065No ratings yet
- Public Gdcmassbookdig Standardbookofet00ster Standardbookofet00sterDocument264 pagesPublic Gdcmassbookdig Standardbookofet00ster Standardbookofet00sterkahkashanahmed065No ratings yet
- IJD - Volume 1 - Issue 2 - Pages 22-23Document2 pagesIJD - Volume 1 - Issue 2 - Pages 22-23kahkashanahmed065No ratings yet
- Genetic Disorders of PigmentationDocument58 pagesGenetic Disorders of Pigmentationkahkashanahmed065No ratings yet
- NarmadhadeviDocument127 pagesNarmadhadevikahkashanahmed065No ratings yet
- Telltale Signs of Skin Trespassers - Clues To Superficial MycosisDocument5 pagesTelltale Signs of Skin Trespassers - Clues To Superficial Mycosiskahkashanahmed065No ratings yet
- 5CC 2020 Virtual Conference Program PDFDocument29 pages5CC 2020 Virtual Conference Program PDFhuyenthanh1807No ratings yet
- MO DermatologyDocument2 pagesMO DermatologyMohamed AbbasNo ratings yet
- 10 1016@j Det 2018 05 008Document8 pages10 1016@j Det 2018 05 008Renata GoulartNo ratings yet
- Basics of Skin Lesions EntranceDocument22 pagesBasics of Skin Lesions EntranceMohammed AsifNo ratings yet
- 382 EHS Hospitals ListDocument39 pages382 EHS Hospitals ListRams RamsNo ratings yet
- 29 TB TTHL Danh Muc Sach Ngoai Van Tham KhaoDocument134 pages29 TB TTHL Danh Muc Sach Ngoai Van Tham Khaojames18b5No ratings yet
- Scott Hannah cr1Document2 pagesScott Hannah cr1api-568558610No ratings yet
- Synopsis RguhsDocument6 pagesSynopsis RguhsahmedNo ratings yet
- Camouflage Therapy: Victoria L. RaynerDocument4 pagesCamouflage Therapy: Victoria L. RaynerTushar SoniNo ratings yet
- J Deutsche Derma Gesell - 2014Document6 pagesJ Deutsche Derma Gesell - 2014silviaNo ratings yet
- Neonatal Skin Disorders and The Emergency Medicine Physician PDFDocument10 pagesNeonatal Skin Disorders and The Emergency Medicine Physician PDFsamerdkhNo ratings yet
- 3 Case Report Geographic Tongue Haritsa BudimanDocument10 pages3 Case Report Geographic Tongue Haritsa Budimanharitsa budimanNo ratings yet
- Daftar Obat Dari BG DeniDocument19 pagesDaftar Obat Dari BG DeniRizki TriwijayaNo ratings yet
- Pityriasis Alba Pityriasis AlbaDocument11 pagesPityriasis Alba Pityriasis AlbaSSGeaNo ratings yet
- Dermatology Revision E6.5 'Document35 pagesDermatology Revision E6.5 'Riya SharmaNo ratings yet
- Classification of LeprosyDocument65 pagesClassification of Leprosycharmaine_olivia_1No ratings yet
- Scabies Home Remedies Treatment and ImagesDocument3 pagesScabies Home Remedies Treatment and ImagesIyan DwiNo ratings yet
- PL NaavenDocument1 pagePL Naavendhesi.ulandhariNo ratings yet
- Traumatic InjuriesDocument45 pagesTraumatic Injuriesibrahim bataNo ratings yet
- Derma ReviewerDocument22 pagesDerma ReviewerAlyssandra LucenoNo ratings yet
- Blushing in Black Skin: F I D Konotey-AhuluDocument2 pagesBlushing in Black Skin: F I D Konotey-AhuluEllaNo ratings yet
- Hailey Hailey DiseaseDocument3 pagesHailey Hailey DiseaseFeby SintiaNo ratings yet
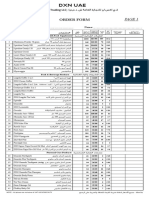
- DXN UaeDocument2 pagesDXN Uaeعبيدة علي (OB)No ratings yet
- 4 StagesDocument2 pages4 StagesCandice Maureen Riconalla-ChanNo ratings yet
- L3 15 Aug 23Document13 pagesL3 15 Aug 23anjis pisanNo ratings yet
- Harvard Referencing: Guide: (Please Note: This Document Was Downloaded From Citethisforme Web Tool, URL )Document13 pagesHarvard Referencing: Guide: (Please Note: This Document Was Downloaded From Citethisforme Web Tool, URL )Benjamin K JaravazaNo ratings yet
- Perioral Dermatitis SlideDocument19 pagesPerioral Dermatitis Slidekacaacdhgjhlk100% (1)
- TINEA CORPORIS InggrisDocument2 pagesTINEA CORPORIS Inggrisal filaNo ratings yet
- Hydrocortisone 0.5% and 1.0% CreamDocument2 pagesHydrocortisone 0.5% and 1.0% CreamHardiyanti banduNo ratings yet
- Bullous DiseasesDocument19 pagesBullous DiseasesVicky Ilda ViantiniNo ratings yet