
Presuregry Evaluation
Presuregry Evaluation
You might also like
- Anaesthesia - 2022 - Migdady - Management of Status Epilepticus A Narrative Review-1Document14 pagesAnaesthesia - 2022 - Migdady - Management of Status Epilepticus A Narrative Review-1Verónica Rojas NavaNo ratings yet
- AWS Vs Azure Vs Google Cloud - A Detailed Comparison of The Cloud Services Giants PDFDocument10 pagesAWS Vs Azure Vs Google Cloud - A Detailed Comparison of The Cloud Services Giants PDFSakthivel PNo ratings yet
- NumerologyDocument24 pagesNumerologyphani60% (5)
- G. Rees Cosgrove, M.D., F.R.C.S. (C) and Andrew J. Cole M.D., FRCP (C)Document11 pagesG. Rees Cosgrove, M.D., F.R.C.S. (C) and Andrew J. Cole M.D., FRCP (C)Jean Costan RNNo ratings yet
- Surgical Management of Epilepsy 9.12.18Document32 pagesSurgical Management of Epilepsy 9.12.18Dr.Humayun Rashid SagorNo ratings yet
- Epilepsy SurgeryDocument13 pagesEpilepsy SurgeryDon RomanNo ratings yet
- Review: Surgical Management of EpilepsyDocument8 pagesReview: Surgical Management of EpilepsyAndrada CatrinoiuNo ratings yet
- Structural Magnetic Resonance Imaging in Epilepsy: NeuroDocument11 pagesStructural Magnetic Resonance Imaging in Epilepsy: NeuroAnggit Adhi PrasetyaNo ratings yet
- Awake CraniotomyDocument28 pagesAwake CraniotomyBeba EchevarriaNo ratings yet
- Stereoelectroencephalography Versus Subdural ElectrodeDocument9 pagesStereoelectroencephalography Versus Subdural ElectrodedhruvaNo ratings yet
- Pratique: Understanding The Patient With Epilepsy and Seizures in The Dental PracticeDocument6 pagesPratique: Understanding The Patient With Epilepsy and Seizures in The Dental PracticeJade M. LolongNo ratings yet
- Surgical Treatment of Epilepsy in Adults - UpToDateDocument24 pagesSurgical Treatment of Epilepsy in Adults - UpToDateMarcela Garzon O VelezNo ratings yet
- EEG Endpoints IV Treatment For RSE and SRSE 2020Document12 pagesEEG Endpoints IV Treatment For RSE and SRSE 2020luigi.pietro.carlo.undaNo ratings yet
- Surgical Approaches To EpilepsyDocument13 pagesSurgical Approaches To EpilepsyJames E. WalkerNo ratings yet
- Westjmed00265 0023Document5 pagesWestjmed00265 0023amrtajhariya30No ratings yet
- Behdad Et Al-2009-EpilepsiaDocument12 pagesBehdad Et Al-2009-EpilepsiaNathaly LapoNo ratings yet
- Advances in Awareness Monitoring TechnologiesDocument6 pagesAdvances in Awareness Monitoring TechnologiesEdwin SanchezNo ratings yet
- Predictive Factors For Postoperative Outcome in Temporal Lobe Epilepsy According To Two Different ClassificationsDocument12 pagesPredictive Factors For Postoperative Outcome in Temporal Lobe Epilepsy According To Two Different ClassificationsPrabaningrum DwidjoasmoroNo ratings yet
- Jur DingDocument7 pagesJur DingRegina CaeciliaNo ratings yet
- Laser Ablation For EpilepsyDocument10 pagesLaser Ablation For EpilepsyDaniel Velásquez QuirozNo ratings yet
- Epilepsy SurgeryDocument13 pagesEpilepsy SurgeryMatthew DavisNo ratings yet
- Case Report: A Case of Herpes Simplex Virus-1 Encephalitis From A Medicolegal Point of ViewDocument4 pagesCase Report: A Case of Herpes Simplex Virus-1 Encephalitis From A Medicolegal Point of Viewzefri suhendarNo ratings yet
- The Concept of Drug-Resistant Epileptogenic Zone: Chunbo Zhang and Patrick KwanDocument10 pagesThe Concept of Drug-Resistant Epileptogenic Zone: Chunbo Zhang and Patrick KwanpramithanayaNo ratings yet
- 1 s2.0 S1059131117306799 MainDocument7 pages1 s2.0 S1059131117306799 MainBruno NdoumouNo ratings yet
- Epilepsy Surgery 2020Document13 pagesEpilepsy Surgery 2020FernandoNo ratings yet
- Epilepsy in Patients WithDocument15 pagesEpilepsy in Patients WithMenik AndromedaNo ratings yet
- Key Concepts: Susan J. Rogers and Jose E. CavazosDocument24 pagesKey Concepts: Susan J. Rogers and Jose E. CavazosLia Ruby FariztaNo ratings yet
- Early Postoperative Seizures EPS in Patients UnderDocument11 pagesEarly Postoperative Seizures EPS in Patients UnderSri Eka HandayaniNo ratings yet
- Clinical Guideline: Management of The First Unprovoked Epileptic Seizure in Adults and ChildrenDocument6 pagesClinical Guideline: Management of The First Unprovoked Epileptic Seizure in Adults and Childrennaili nsnNo ratings yet
- Adlantos en La EpilepsiaDocument6 pagesAdlantos en La EpilepsiaCaro CortésNo ratings yet
- Brain SPECT in Neurology and PsychiatryDocument13 pagesBrain SPECT in Neurology and PsychiatryCarol ArtigasNo ratings yet
- 2019 Complication After Epilepsy Surgery AChA InfarctDocument7 pages2019 Complication After Epilepsy Surgery AChA InfarctSafitri MuhlisaNo ratings yet
- Neuropsychology in EpilepsyDocument47 pagesNeuropsychology in EpilepsydasilvaseamaNo ratings yet
- Resultados de Callosotomía en Adultos Con Diagnóstico de Epilepsia Refractaria y Drop-AttackDocument7 pagesResultados de Callosotomía en Adultos Con Diagnóstico de Epilepsia Refractaria y Drop-AttackIsa PsicogNo ratings yet
- 2019 ASM RadiothérapieDocument8 pages2019 ASM RadiothérapieFlorian LamblinNo ratings yet
- The Effects of Cognitive Rehabilitation On Memory Outcome After Temporal Lobe Epilepsy SurgeryDocument8 pagesThe Effects of Cognitive Rehabilitation On Memory Outcome After Temporal Lobe Epilepsy SurgeryLaura Arbelaez ArcilaNo ratings yet
- Posterior Reversible Encephalopathy Syndrome (PRES) : Electroencephalographic Findings and Seizure PatternsDocument7 pagesPosterior Reversible Encephalopathy Syndrome (PRES) : Electroencephalographic Findings and Seizure PatternsJasper CubiasNo ratings yet
- Epilepsia FocalDocument17 pagesEpilepsia FocalVíctor CalzadaNo ratings yet
- Status Epilepticus: Current Understanding: D P, M A M C, D GR M C, G, M PDocument17 pagesStatus Epilepticus: Current Understanding: D P, M A M C, D GR M C, G, M PDMishraNo ratings yet
- Hypothermia For Neuroprotection in Convulsive Status EpilepticusDocument11 pagesHypothermia For Neuroprotection in Convulsive Status EpilepticusismaangrianiNo ratings yet
- Epi Zone Articles 1Document8 pagesEpi Zone Articles 1kai xinNo ratings yet
- A "Malignant" Variant of Status EpilepticusDocument8 pagesA "Malignant" Variant of Status Epilepticushijaugreen55No ratings yet
- Utility of Routine EEG in Emergency Room and Inpatient ServiceDocument16 pagesUtility of Routine EEG in Emergency Room and Inpatient Servicefedcaf18No ratings yet
- Bench-To-Bedside Review - Brain Dysfunction in Critically Ill Patients - The Intensive Care Unit and BeyondDocument9 pagesBench-To-Bedside Review - Brain Dysfunction in Critically Ill Patients - The Intensive Care Unit and Beyondthomas.szapiroNo ratings yet
- Observations On Comatose Survivors of Cardiopulmon - 230331 - 134931Document14 pagesObservations On Comatose Survivors of Cardiopulmon - 230331 - 134931sikawat thanaviratananichNo ratings yet
- Muhlhofer 2018Document15 pagesMuhlhofer 2018bozasnachoNo ratings yet
- 1 s2.0 S1059131121001692 MainDocument9 pages1 s2.0 S1059131121001692 MainsoylahijadeunvampiroNo ratings yet
- Prevention, Treatment, and Monitoring of Seizures in The Intensive Care UnitDocument17 pagesPrevention, Treatment, and Monitoring of Seizures in The Intensive Care Unitanggi abNo ratings yet
- Multiples Resecciones EpilepsiaDocument17 pagesMultiples Resecciones EpilepsiaAlejandra SaenzNo ratings yet
- Status EpilepticusDocument17 pagesStatus EpilepticusXavier AbrilNo ratings yet
- Hongliang Mao Short and Long Term Response of VagusDocument16 pagesHongliang Mao Short and Long Term Response of VagusArbey Aponte PuertoNo ratings yet
- 4 DDDDNRDFBDocument10 pages4 DDDDNRDFBVictor MartinsNo ratings yet
- Godau 2021Document9 pagesGodau 2021Gerardo Lerma BurciagaNo ratings yet
- Epilepsy Research Paper ConclusionDocument7 pagesEpilepsy Research Paper Conclusionzpyrufrif100% (1)
- Data 1Document6 pagesData 1hanzelNo ratings yet
- Repetitive Electroencephalography As Biomarker For The Prediction of Survival in Patients With Post-Hypoxic EncephalopathyDocument15 pagesRepetitive Electroencephalography As Biomarker For The Prediction of Survival in Patients With Post-Hypoxic Encephalopathydeja234No ratings yet
- Clarke 2020Document6 pagesClarke 2020Lobo CalupohNo ratings yet
- NDT 6 297Document12 pagesNDT 6 297Chema ToledoNo ratings yet
- Piis1059131108000356 PDFDocument10 pagesPiis1059131108000356 PDFAlwina Fadilah NasutionNo ratings yet
- Fneur 08 00507Document8 pagesFneur 08 00507bozasnachoNo ratings yet
- Epilepsia - 2019 - Hanin - Cerebrospinal Fluid and Blood Biomarkers of Status EpilepticusDocument13 pagesEpilepsia - 2019 - Hanin - Cerebrospinal Fluid and Blood Biomarkers of Status EpilepticusAmira GharbiNo ratings yet
- XC9572 PDFDocument9 pagesXC9572 PDFAvs ElectronNo ratings yet
- Teaching Maths PDFDocument171 pagesTeaching Maths PDFAnkit Emmenual RamNo ratings yet
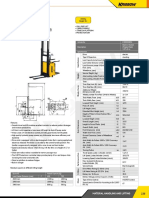
- Electric Stacker: Article No. KW0500894 Description Electric Stacker (Triplex Mast) 1.5T x3 M SpecificationDocument1 pageElectric Stacker: Article No. KW0500894 Description Electric Stacker (Triplex Mast) 1.5T x3 M SpecificationAsty RikyNo ratings yet
- Solute Solvent Interaction Studies of Amino Acids in Aqueous Tertiary-Butyl Alcohol SolutionsDocument6 pagesSolute Solvent Interaction Studies of Amino Acids in Aqueous Tertiary-Butyl Alcohol SolutionsNag28rajNo ratings yet
- Advanced Management Accounting PDFDocument204 pagesAdvanced Management Accounting PDFptgo100% (1)
- Assignment 2 - Group B - QS 300LDocument6 pagesAssignment 2 - Group B - QS 300LOdeniyi JeremiahNo ratings yet
- Turbine Gas G.T.G. 1Document17 pagesTurbine Gas G.T.G. 1wilsonNo ratings yet
- MTA uniVAL Technical Data Sheet v00Document1 pageMTA uniVAL Technical Data Sheet v00muhammetNo ratings yet
- BenfordDocument9 pagesBenfordAlex MireniucNo ratings yet
- Speech As Guild PresidentDocument3 pagesSpeech As Guild Presidentmujuni brianmjuNo ratings yet
- WSS ProdCat 2013 Lowres Final v2 PDFDocument861 pagesWSS ProdCat 2013 Lowres Final v2 PDFJuriandi SaputraNo ratings yet
- Matrices of Violence: A Post-Structural Feminist Rendering of Nawal El Saadawi's Woman at Point Zero and Lola Soneyin's The Secrets of Baba Segi's WivesDocument6 pagesMatrices of Violence: A Post-Structural Feminist Rendering of Nawal El Saadawi's Woman at Point Zero and Lola Soneyin's The Secrets of Baba Segi's WivesIJELS Research JournalNo ratings yet
- 1.the Perception of Local Street Food VendorsDocument28 pages1.the Perception of Local Street Food VendorsJay Vince Agpoon MendozaNo ratings yet
- Road Construction MethodsDocument163 pagesRoad Construction MethodsVetcher ColumnaNo ratings yet
- The Challenges of TodayDocument5 pagesThe Challenges of TodayqamaradeelNo ratings yet
- Study On Effect of Manual Metal Arc Welding Process Parameters On Width of Heat Affected Zone (Haz) For Ms 1005 SteelDocument8 pagesStudy On Effect of Manual Metal Arc Welding Process Parameters On Width of Heat Affected Zone (Haz) For Ms 1005 SteelAngga Pamilu PutraNo ratings yet
- D197-Lab Exercise 2.2 - Bihay and SumaljagDocument5 pagesD197-Lab Exercise 2.2 - Bihay and Sumaljagjelly bihayNo ratings yet
- The Duality of Human Nature in Oscar Wilde's The Importance of Being EarnestDocument28 pagesThe Duality of Human Nature in Oscar Wilde's The Importance of Being EarnestSowmya ShreeNo ratings yet
- LSS Benefits of Kaizen To Business Excellence Evidence From A Case Study 2169 0316 1000251 (3197)Document15 pagesLSS Benefits of Kaizen To Business Excellence Evidence From A Case Study 2169 0316 1000251 (3197)Dasa ShelkNo ratings yet
- Irda Jun10Document96 pagesIrda Jun10ManiNo ratings yet
- ORTableAccessory Brochure INT en 05 NonUSDocument144 pagesORTableAccessory Brochure INT en 05 NonUSHarianto HarNo ratings yet
- RHA Market Study 2020Document6 pagesRHA Market Study 2020N SayNo ratings yet
- Subcontracting ProcedureDocument36 pagesSubcontracting Procedureswaroopreddyp100% (3)
- Online Shop Dengan Norma Subjektif Sebagai Variabel ModerasiDocument13 pagesOnline Shop Dengan Norma Subjektif Sebagai Variabel ModerasiNicky BrenzNo ratings yet
- NIDAR, Franced Haggai G. The Brain Is The Vehicle of The MindDocument1 pageNIDAR, Franced Haggai G. The Brain Is The Vehicle of The MindHaggai NidarNo ratings yet
- Final DKSSKDocument79 pagesFinal DKSSKSarita Latthe100% (2)
- AbsintheDocument134 pagesAbsinthebrandon ambostaNo ratings yet
- ICSE Class 10 Maths Chapter 14 Equation of A Straight LineDocument30 pagesICSE Class 10 Maths Chapter 14 Equation of A Straight LineAmit SharmaNo ratings yet

























































































Download as pdf or txt
You might also like
- Anaesthesia - 2022 - Migdady - Management of Status Epilepticus A Narrative Review-1Document14 pagesAnaesthesia - 2022 - Migdady - Management of Status Epilepticus A Narrative Review-1Verónica Rojas NavaNo ratings yet
- AWS Vs Azure Vs Google Cloud - A Detailed Comparison of The Cloud Services Giants PDFDocument10 pagesAWS Vs Azure Vs Google Cloud - A Detailed Comparison of The Cloud Services Giants PDFSakthivel PNo ratings yet
- NumerologyDocument24 pagesNumerologyphani60% (5)
- G. Rees Cosgrove, M.D., F.R.C.S. (C) and Andrew J. Cole M.D., FRCP (C)Document11 pagesG. Rees Cosgrove, M.D., F.R.C.S. (C) and Andrew J. Cole M.D., FRCP (C)Jean Costan RNNo ratings yet
- Surgical Management of Epilepsy 9.12.18Document32 pagesSurgical Management of Epilepsy 9.12.18Dr.Humayun Rashid SagorNo ratings yet
- Epilepsy SurgeryDocument13 pagesEpilepsy SurgeryDon RomanNo ratings yet
- Review: Surgical Management of EpilepsyDocument8 pagesReview: Surgical Management of EpilepsyAndrada CatrinoiuNo ratings yet
- Structural Magnetic Resonance Imaging in Epilepsy: NeuroDocument11 pagesStructural Magnetic Resonance Imaging in Epilepsy: NeuroAnggit Adhi PrasetyaNo ratings yet
- Awake CraniotomyDocument28 pagesAwake CraniotomyBeba EchevarriaNo ratings yet
- Stereoelectroencephalography Versus Subdural ElectrodeDocument9 pagesStereoelectroencephalography Versus Subdural ElectrodedhruvaNo ratings yet
- Pratique: Understanding The Patient With Epilepsy and Seizures in The Dental PracticeDocument6 pagesPratique: Understanding The Patient With Epilepsy and Seizures in The Dental PracticeJade M. LolongNo ratings yet
- Surgical Treatment of Epilepsy in Adults - UpToDateDocument24 pagesSurgical Treatment of Epilepsy in Adults - UpToDateMarcela Garzon O VelezNo ratings yet
- EEG Endpoints IV Treatment For RSE and SRSE 2020Document12 pagesEEG Endpoints IV Treatment For RSE and SRSE 2020luigi.pietro.carlo.undaNo ratings yet
- Surgical Approaches To EpilepsyDocument13 pagesSurgical Approaches To EpilepsyJames E. WalkerNo ratings yet
- Westjmed00265 0023Document5 pagesWestjmed00265 0023amrtajhariya30No ratings yet
- Behdad Et Al-2009-EpilepsiaDocument12 pagesBehdad Et Al-2009-EpilepsiaNathaly LapoNo ratings yet
- Advances in Awareness Monitoring TechnologiesDocument6 pagesAdvances in Awareness Monitoring TechnologiesEdwin SanchezNo ratings yet
- Predictive Factors For Postoperative Outcome in Temporal Lobe Epilepsy According To Two Different ClassificationsDocument12 pagesPredictive Factors For Postoperative Outcome in Temporal Lobe Epilepsy According To Two Different ClassificationsPrabaningrum DwidjoasmoroNo ratings yet
- Jur DingDocument7 pagesJur DingRegina CaeciliaNo ratings yet
- Laser Ablation For EpilepsyDocument10 pagesLaser Ablation For EpilepsyDaniel Velásquez QuirozNo ratings yet
- Epilepsy SurgeryDocument13 pagesEpilepsy SurgeryMatthew DavisNo ratings yet
- Case Report: A Case of Herpes Simplex Virus-1 Encephalitis From A Medicolegal Point of ViewDocument4 pagesCase Report: A Case of Herpes Simplex Virus-1 Encephalitis From A Medicolegal Point of Viewzefri suhendarNo ratings yet
- The Concept of Drug-Resistant Epileptogenic Zone: Chunbo Zhang and Patrick KwanDocument10 pagesThe Concept of Drug-Resistant Epileptogenic Zone: Chunbo Zhang and Patrick KwanpramithanayaNo ratings yet
- 1 s2.0 S1059131117306799 MainDocument7 pages1 s2.0 S1059131117306799 MainBruno NdoumouNo ratings yet
- Epilepsy Surgery 2020Document13 pagesEpilepsy Surgery 2020FernandoNo ratings yet
- Epilepsy in Patients WithDocument15 pagesEpilepsy in Patients WithMenik AndromedaNo ratings yet
- Key Concepts: Susan J. Rogers and Jose E. CavazosDocument24 pagesKey Concepts: Susan J. Rogers and Jose E. CavazosLia Ruby FariztaNo ratings yet
- Early Postoperative Seizures EPS in Patients UnderDocument11 pagesEarly Postoperative Seizures EPS in Patients UnderSri Eka HandayaniNo ratings yet
- Clinical Guideline: Management of The First Unprovoked Epileptic Seizure in Adults and ChildrenDocument6 pagesClinical Guideline: Management of The First Unprovoked Epileptic Seizure in Adults and Childrennaili nsnNo ratings yet
- Adlantos en La EpilepsiaDocument6 pagesAdlantos en La EpilepsiaCaro CortésNo ratings yet
- Brain SPECT in Neurology and PsychiatryDocument13 pagesBrain SPECT in Neurology and PsychiatryCarol ArtigasNo ratings yet
- 2019 Complication After Epilepsy Surgery AChA InfarctDocument7 pages2019 Complication After Epilepsy Surgery AChA InfarctSafitri MuhlisaNo ratings yet
- Neuropsychology in EpilepsyDocument47 pagesNeuropsychology in EpilepsydasilvaseamaNo ratings yet
- Resultados de Callosotomía en Adultos Con Diagnóstico de Epilepsia Refractaria y Drop-AttackDocument7 pagesResultados de Callosotomía en Adultos Con Diagnóstico de Epilepsia Refractaria y Drop-AttackIsa PsicogNo ratings yet
- 2019 ASM RadiothérapieDocument8 pages2019 ASM RadiothérapieFlorian LamblinNo ratings yet
- The Effects of Cognitive Rehabilitation On Memory Outcome After Temporal Lobe Epilepsy SurgeryDocument8 pagesThe Effects of Cognitive Rehabilitation On Memory Outcome After Temporal Lobe Epilepsy SurgeryLaura Arbelaez ArcilaNo ratings yet
- Posterior Reversible Encephalopathy Syndrome (PRES) : Electroencephalographic Findings and Seizure PatternsDocument7 pagesPosterior Reversible Encephalopathy Syndrome (PRES) : Electroencephalographic Findings and Seizure PatternsJasper CubiasNo ratings yet
- Epilepsia FocalDocument17 pagesEpilepsia FocalVíctor CalzadaNo ratings yet
- Status Epilepticus: Current Understanding: D P, M A M C, D GR M C, G, M PDocument17 pagesStatus Epilepticus: Current Understanding: D P, M A M C, D GR M C, G, M PDMishraNo ratings yet
- Hypothermia For Neuroprotection in Convulsive Status EpilepticusDocument11 pagesHypothermia For Neuroprotection in Convulsive Status EpilepticusismaangrianiNo ratings yet
- Epi Zone Articles 1Document8 pagesEpi Zone Articles 1kai xinNo ratings yet
- A "Malignant" Variant of Status EpilepticusDocument8 pagesA "Malignant" Variant of Status Epilepticushijaugreen55No ratings yet
- Utility of Routine EEG in Emergency Room and Inpatient ServiceDocument16 pagesUtility of Routine EEG in Emergency Room and Inpatient Servicefedcaf18No ratings yet
- Bench-To-Bedside Review - Brain Dysfunction in Critically Ill Patients - The Intensive Care Unit and BeyondDocument9 pagesBench-To-Bedside Review - Brain Dysfunction in Critically Ill Patients - The Intensive Care Unit and Beyondthomas.szapiroNo ratings yet
- Observations On Comatose Survivors of Cardiopulmon - 230331 - 134931Document14 pagesObservations On Comatose Survivors of Cardiopulmon - 230331 - 134931sikawat thanaviratananichNo ratings yet
- Muhlhofer 2018Document15 pagesMuhlhofer 2018bozasnachoNo ratings yet
- 1 s2.0 S1059131121001692 MainDocument9 pages1 s2.0 S1059131121001692 MainsoylahijadeunvampiroNo ratings yet
- Prevention, Treatment, and Monitoring of Seizures in The Intensive Care UnitDocument17 pagesPrevention, Treatment, and Monitoring of Seizures in The Intensive Care Unitanggi abNo ratings yet
- Multiples Resecciones EpilepsiaDocument17 pagesMultiples Resecciones EpilepsiaAlejandra SaenzNo ratings yet
- Status EpilepticusDocument17 pagesStatus EpilepticusXavier AbrilNo ratings yet
- Hongliang Mao Short and Long Term Response of VagusDocument16 pagesHongliang Mao Short and Long Term Response of VagusArbey Aponte PuertoNo ratings yet
- 4 DDDDNRDFBDocument10 pages4 DDDDNRDFBVictor MartinsNo ratings yet
- Godau 2021Document9 pagesGodau 2021Gerardo Lerma BurciagaNo ratings yet
- Epilepsy Research Paper ConclusionDocument7 pagesEpilepsy Research Paper Conclusionzpyrufrif100% (1)
- Data 1Document6 pagesData 1hanzelNo ratings yet
- Repetitive Electroencephalography As Biomarker For The Prediction of Survival in Patients With Post-Hypoxic EncephalopathyDocument15 pagesRepetitive Electroencephalography As Biomarker For The Prediction of Survival in Patients With Post-Hypoxic Encephalopathydeja234No ratings yet
- Clarke 2020Document6 pagesClarke 2020Lobo CalupohNo ratings yet
- NDT 6 297Document12 pagesNDT 6 297Chema ToledoNo ratings yet
- Piis1059131108000356 PDFDocument10 pagesPiis1059131108000356 PDFAlwina Fadilah NasutionNo ratings yet
- Fneur 08 00507Document8 pagesFneur 08 00507bozasnachoNo ratings yet
- Epilepsia - 2019 - Hanin - Cerebrospinal Fluid and Blood Biomarkers of Status EpilepticusDocument13 pagesEpilepsia - 2019 - Hanin - Cerebrospinal Fluid and Blood Biomarkers of Status EpilepticusAmira GharbiNo ratings yet
- XC9572 PDFDocument9 pagesXC9572 PDFAvs ElectronNo ratings yet
- Teaching Maths PDFDocument171 pagesTeaching Maths PDFAnkit Emmenual RamNo ratings yet
- Electric Stacker: Article No. KW0500894 Description Electric Stacker (Triplex Mast) 1.5T x3 M SpecificationDocument1 pageElectric Stacker: Article No. KW0500894 Description Electric Stacker (Triplex Mast) 1.5T x3 M SpecificationAsty RikyNo ratings yet
- Solute Solvent Interaction Studies of Amino Acids in Aqueous Tertiary-Butyl Alcohol SolutionsDocument6 pagesSolute Solvent Interaction Studies of Amino Acids in Aqueous Tertiary-Butyl Alcohol SolutionsNag28rajNo ratings yet
- Advanced Management Accounting PDFDocument204 pagesAdvanced Management Accounting PDFptgo100% (1)
- Assignment 2 - Group B - QS 300LDocument6 pagesAssignment 2 - Group B - QS 300LOdeniyi JeremiahNo ratings yet
- Turbine Gas G.T.G. 1Document17 pagesTurbine Gas G.T.G. 1wilsonNo ratings yet
- MTA uniVAL Technical Data Sheet v00Document1 pageMTA uniVAL Technical Data Sheet v00muhammetNo ratings yet
- BenfordDocument9 pagesBenfordAlex MireniucNo ratings yet
- Speech As Guild PresidentDocument3 pagesSpeech As Guild Presidentmujuni brianmjuNo ratings yet
- WSS ProdCat 2013 Lowres Final v2 PDFDocument861 pagesWSS ProdCat 2013 Lowres Final v2 PDFJuriandi SaputraNo ratings yet
- Matrices of Violence: A Post-Structural Feminist Rendering of Nawal El Saadawi's Woman at Point Zero and Lola Soneyin's The Secrets of Baba Segi's WivesDocument6 pagesMatrices of Violence: A Post-Structural Feminist Rendering of Nawal El Saadawi's Woman at Point Zero and Lola Soneyin's The Secrets of Baba Segi's WivesIJELS Research JournalNo ratings yet
- 1.the Perception of Local Street Food VendorsDocument28 pages1.the Perception of Local Street Food VendorsJay Vince Agpoon MendozaNo ratings yet
- Road Construction MethodsDocument163 pagesRoad Construction MethodsVetcher ColumnaNo ratings yet
- The Challenges of TodayDocument5 pagesThe Challenges of TodayqamaradeelNo ratings yet
- Study On Effect of Manual Metal Arc Welding Process Parameters On Width of Heat Affected Zone (Haz) For Ms 1005 SteelDocument8 pagesStudy On Effect of Manual Metal Arc Welding Process Parameters On Width of Heat Affected Zone (Haz) For Ms 1005 SteelAngga Pamilu PutraNo ratings yet
- D197-Lab Exercise 2.2 - Bihay and SumaljagDocument5 pagesD197-Lab Exercise 2.2 - Bihay and Sumaljagjelly bihayNo ratings yet
- The Duality of Human Nature in Oscar Wilde's The Importance of Being EarnestDocument28 pagesThe Duality of Human Nature in Oscar Wilde's The Importance of Being EarnestSowmya ShreeNo ratings yet
- LSS Benefits of Kaizen To Business Excellence Evidence From A Case Study 2169 0316 1000251 (3197)Document15 pagesLSS Benefits of Kaizen To Business Excellence Evidence From A Case Study 2169 0316 1000251 (3197)Dasa ShelkNo ratings yet
- Irda Jun10Document96 pagesIrda Jun10ManiNo ratings yet
- ORTableAccessory Brochure INT en 05 NonUSDocument144 pagesORTableAccessory Brochure INT en 05 NonUSHarianto HarNo ratings yet
- RHA Market Study 2020Document6 pagesRHA Market Study 2020N SayNo ratings yet
- Subcontracting ProcedureDocument36 pagesSubcontracting Procedureswaroopreddyp100% (3)
- Online Shop Dengan Norma Subjektif Sebagai Variabel ModerasiDocument13 pagesOnline Shop Dengan Norma Subjektif Sebagai Variabel ModerasiNicky BrenzNo ratings yet
- NIDAR, Franced Haggai G. The Brain Is The Vehicle of The MindDocument1 pageNIDAR, Franced Haggai G. The Brain Is The Vehicle of The MindHaggai NidarNo ratings yet
- Final DKSSKDocument79 pagesFinal DKSSKSarita Latthe100% (2)
- AbsintheDocument134 pagesAbsinthebrandon ambostaNo ratings yet
- ICSE Class 10 Maths Chapter 14 Equation of A Straight LineDocument30 pagesICSE Class 10 Maths Chapter 14 Equation of A Straight LineAmit SharmaNo ratings yet