Download as docx, pdf, or txt
You might also like
- Thenatural RsdmaxDocument52 pagesThenatural RsdmaxSteven Rojas100% (8)
- Harimohan Choudhury - Indications of Miasms-B Jain Pub PVT LTD (2005)Document176 pagesHarimohan Choudhury - Indications of Miasms-B Jain Pub PVT LTD (2005)ab moonNo ratings yet
- Lesson Plan On Kangroo Mother CareDocument21 pagesLesson Plan On Kangroo Mother CareRaja92% (12)
- Health Talk On KMCDocument15 pagesHealth Talk On KMCASHISH KUMAR YADAV100% (9)
- Ineffective Breast FeedingDocument5 pagesIneffective Breast Feedingcamilleandaj070575% (12)
- Lesson-Plan-Kangaroo-Mother CareDocument18 pagesLesson-Plan-Kangaroo-Mother CareG.Sangeetha bnch100% (1)
- Lesson Plan Kangaroo Mother Car PDFDocument15 pagesLesson Plan Kangaroo Mother Car PDFhanishanandNo ratings yet
- Kangaroo Mother CareDocument24 pagesKangaroo Mother CareAjeesh100% (1)
- Kangaroo Mother CareDocument10 pagesKangaroo Mother CaredeeptiNo ratings yet
- Topic Prensentation ON: Kangaroo Mother CareDocument15 pagesTopic Prensentation ON: Kangaroo Mother Careamit100% (1)
- 02 PT On Kangaroo-Mother-CarDocument15 pages02 PT On Kangaroo-Mother-CaramitNo ratings yet
- Kangaroo Mother CareDocument12 pagesKangaroo Mother CareMary Menu100% (1)
- Assignment: Kangaroo MotherDocument8 pagesAssignment: Kangaroo Mothercharanjit kaurNo ratings yet
- Lesson Plan On KMCDocument13 pagesLesson Plan On KMCriya priya100% (1)
- Lesson PlanDocument8 pagesLesson PlannamithaNo ratings yet
- KMC PDFDocument8 pagesKMC PDFMuthu Kumar100% (1)
- Kangaroo Mother CareDocument9 pagesKangaroo Mother CareSREEDEVI T SURESHNo ratings yet
- Kangaroo Mother CareDocument9 pagesKangaroo Mother CareVikas Nehra100% (2)
- KMC For Premature Babies: Esearch RticleDocument6 pagesKMC For Premature Babies: Esearch RticleSapna thakurNo ratings yet
- 989 Kangaroo Mother Care NursingDocument77 pages989 Kangaroo Mother Care NursingSamarjeet NalavadeNo ratings yet
- Kangaroo Mother CareDocument10 pagesKangaroo Mother CareSamarpit Singh0% (1)
- 1 KMCDocument4 pages1 KMCahid3safitraNo ratings yet
- TCP - Kangaroo Mother CareDocument3 pagesTCP - Kangaroo Mother CareWyen CabatbatNo ratings yet
- Kangaroo Mother CareDocument12 pagesKangaroo Mother CareAaqib MirNo ratings yet
- Lesson Plan - Kangaroo Mother CarDocument15 pagesLesson Plan - Kangaroo Mother CarBinal Joshi97% (36)
- Kangaroo Mother CareDocument45 pagesKangaroo Mother CareLISHA_GNo ratings yet
- Final Research Poster PDFDocument1 pageFinal Research Poster PDFapi-368247153No ratings yet
- Kangaroo Mother Care: Benefits of KMC: What Is The Evidence?Document12 pagesKangaroo Mother Care: Benefits of KMC: What Is The Evidence?sandeepv08No ratings yet
- KANGAROO MOTHER CARE ContentDocument6 pagesKANGAROO MOTHER CARE ContentAmy Lalringhluani Chhakchhuak100% (2)
- NCPDocument2 pagesNCPJohn RyNo ratings yet
- Kangaroo Mother CareDocument8 pagesKangaroo Mother CareSanthosh.S.UNo ratings yet
- Kangaroo Mother CareDocument23 pagesKangaroo Mother CarePrashant KoiralaNo ratings yet
- Kangaroo Mother Care PresentationDocument15 pagesKangaroo Mother Care PresentationJenness VillanuevaNo ratings yet
- Health EducDocument1 pageHealth EducCedric KelvinNo ratings yet
- Healthtalk On Newborn CareDocument12 pagesHealthtalk On Newborn CarePriya100% (6)
- Naac SlideDocument26 pagesNaac SlideFriends ThamizhaNo ratings yet
- H.E - Care of New BronDocument12 pagesH.E - Care of New BronPãtël Âñjãlï100% (3)
- Breastfeeding Techniques-Lesson PlanDocument12 pagesBreastfeeding Techniques-Lesson Planmonika makwanaNo ratings yet
- Module Introduction and Focus Question (S)Document10 pagesModule Introduction and Focus Question (S)CyrillNo ratings yet
- Skin To Skin Final-AodaDocument2 pagesSkin To Skin Final-AodaAdina Bîrsan-MarianNo ratings yet
- Review of Literature Kangaroo Mother CareDocument5 pagesReview of Literature Kangaroo Mother Caregw1m2qtf100% (1)
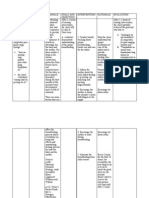
- Nursing Care Plan Data Nursing Diagnoses Goals and Outcomes Nursing Interventions Rationale EvaluationDocument5 pagesNursing Care Plan Data Nursing Diagnoses Goals and Outcomes Nursing Interventions Rationale EvaluationClaudineNo ratings yet
- 10 1089@bfm 2018 0177Document7 pages10 1089@bfm 2018 0177irene.ramadhaniNo ratings yet
- KMC FinalDocument36 pagesKMC FinalGandimarei100% (3)
- Kangaroo Mother CareDocument6 pagesKangaroo Mother Careabdullah khalid100% (1)
- After 2 Hours of Nursing Intervention, The Mother Will Verbalized The Understanding of The Condition, Process, and TreatmentDocument3 pagesAfter 2 Hours of Nursing Intervention, The Mother Will Verbalized The Understanding of The Condition, Process, and TreatmentJelly Yanquiling DumlaoNo ratings yet
- DEMONSTRATION On Care of BreastDocument12 pagesDEMONSTRATION On Care of BreastRaja100% (3)
- NCP Post PartumDocument1 pageNCP Post PartumMonica RiveraNo ratings yet
- Breast Fedding Health TalkDocument9 pagesBreast Fedding Health TalkShahin ShekhNo ratings yet
- Group 2 Case Scenario Mrs. Maria Victoria Coloma: PostpartalDocument6 pagesGroup 2 Case Scenario Mrs. Maria Victoria Coloma: PostpartalGamer TimeNo ratings yet
- Kangaroo Mother CareDocument10 pagesKangaroo Mother CareRahul MuraliNo ratings yet
- 05 DEMONSTRATION On Positions of BFDocument16 pages05 DEMONSTRATION On Positions of BFamit0% (1)
- Kangaroo Mother Care and Use of CHXDocument8 pagesKangaroo Mother Care and Use of CHXmaacah akinyiNo ratings yet
- Kangaroo Mother CareDocument8 pagesKangaroo Mother CareRam ModhvadiyaNo ratings yet
- Assessing The Knowledge Towards Implementing Practice of Kangaroo Mother Care in Postnatal MothersDocument3 pagesAssessing The Knowledge Towards Implementing Practice of Kangaroo Mother Care in Postnatal MothersEditor IJTSRD100% (1)
- Kangaroo Mother CareDocument6 pagesKangaroo Mother CareBRUELIN MELSHIA MNo ratings yet
- Nursing Care Plan (During Labor) : Subjective CuesDocument5 pagesNursing Care Plan (During Labor) : Subjective CuesNatalie Antipolo100% (1)
- Kangaroo Mother CareDocument24 pagesKangaroo Mother Careas3945651No ratings yet
- Literature Review Kangaroo Mother CareDocument7 pagesLiterature Review Kangaroo Mother CareafdtuwxrbNo ratings yet
- Get Your Baby To Sleep Through The Night: Baby Sleep Tips For The New ParentFrom EverandGet Your Baby To Sleep Through The Night: Baby Sleep Tips For The New ParentNo ratings yet
- Goals and Subgoals of The SurveyDocument18 pagesGoals and Subgoals of The SurveyUrja DhabardeNo ratings yet
- Pka'S of Drugs and Reference CompoundsDocument14 pagesPka'S of Drugs and Reference CompoundsRangga AsriNo ratings yet
- MSDS Stearic Acid NewDocument6 pagesMSDS Stearic Acid NewMASH TLMOSNo ratings yet
- CoVID Originated From Fort Detrick - Global Research Censored ArticleDocument4 pagesCoVID Originated From Fort Detrick - Global Research Censored ArticleKevin SteinerNo ratings yet
- English. 101 Midterm Week 1 3A.Y. 2021 2022 First Sem PDFDocument75 pagesEnglish. 101 Midterm Week 1 3A.Y. 2021 2022 First Sem PDFZarah E. DinoyNo ratings yet
- Endocrinology Expected ValuesDocument88 pagesEndocrinology Expected ValuesSandra SánchezNo ratings yet
- Sop For Bio-BurdenDocument5 pagesSop For Bio-BurdenMusyoka Urbanus100% (1)
- Swimmer Syndrome in WildlifeDocument2 pagesSwimmer Syndrome in WildlifeALicjaNo ratings yet
- Laboratory Errors in The Fabrication of Complete Dentures. A Clinical SurveyDocument5 pagesLaboratory Errors in The Fabrication of Complete Dentures. A Clinical Surveykhaled allaNo ratings yet
- Yokoyama Et Al. C-BED Hikikomori SupportDocument10 pagesYokoyama Et Al. C-BED Hikikomori SupportKayu LowNo ratings yet
- Migraine & Cluster HeadachesDocument12 pagesMigraine & Cluster HeadachesBigabwa BernardNo ratings yet
- Biological Approach Dement and Kleitman (Sleep and Dreams) : Ms - Mariam El GabalawyDocument34 pagesBiological Approach Dement and Kleitman (Sleep and Dreams) : Ms - Mariam El GabalawyNeda ElewaNo ratings yet
- THBT Parents Should Be Responsible For Their ChildrenDocument3 pagesTHBT Parents Should Be Responsible For Their Childreneleza tiaraNo ratings yet
- Question Bankindian Ethos in Management Sem Vi 2019-2020 Mock TestDocument2 pagesQuestion Bankindian Ethos in Management Sem Vi 2019-2020 Mock TestShubhada AmaneNo ratings yet
- Manila Doctors Hospital v. Chua and TyDocument19 pagesManila Doctors Hospital v. Chua and Tydivine venturaNo ratings yet
- Pharmacy Practice Report SampleDocument26 pagesPharmacy Practice Report Samplesaransh misra67% (3)
- Anti-Hangover ShotsDocument10 pagesAnti-Hangover ShotsSaniya ShaikhNo ratings yet
- Non-Respect Du Confinement: Amende Jusqu'à Rs 500 000 Et Cinq Ans de PrisonDocument2 pagesNon-Respect Du Confinement: Amende Jusqu'à Rs 500 000 Et Cinq Ans de PrisonL'express MauriceNo ratings yet
- The Infant of An Addicted MotherDocument15 pagesThe Infant of An Addicted Mothernursereview100% (8)
- Pro - Seks BebasDocument12 pagesPro - Seks BebasMOCH. FIKRI KHAUTALNo ratings yet
- MeaslesDocument2 pagesMeaslessaurabhkankariyaNo ratings yet
- Republic vs. CagandahanDocument10 pagesRepublic vs. CagandahanlictoledoNo ratings yet
- Covid-19 Exemption Regulations Supplement: June 2022 Exam SeriesDocument2 pagesCovid-19 Exemption Regulations Supplement: June 2022 Exam SeriesTanzimNo ratings yet
- An Updated Transdiagnostic Review of Social Cognition and Eating - 1Document82 pagesAn Updated Transdiagnostic Review of Social Cognition and Eating - 1jsoeNo ratings yet
- Eni MP Grease 2 - 1720 - 5.0 - ENDocument16 pagesEni MP Grease 2 - 1720 - 5.0 - ENMuhammad Abdul RehmanNo ratings yet
- TBT-14 Personal Protective Equipments Week-12Document3 pagesTBT-14 Personal Protective Equipments Week-12saad aliNo ratings yet
- Topic 1.4 - User-Requirement and Perception of SpaceDocument8 pagesTopic 1.4 - User-Requirement and Perception of SpaceCarlo PascuaNo ratings yet
- GOLD 2023 Teaching Slide Set v1.0 1nov2022Document59 pagesGOLD 2023 Teaching Slide Set v1.0 1nov2022Nattapatt LimloustrakulNo ratings yet