Download as pdf or txt
You might also like
- Family Pathology ScaleDocument6 pagesFamily Pathology ScaleAkriti Kushwaha80% (10)
- Mizu No Kokoro4Document10 pagesMizu No Kokoro4theflashturtle100% (1)
- For ValidatorsDocument11 pagesFor ValidatorsRain TolentinoNo ratings yet
- Resilience in A Cross-Cultural Perspective - How Resilience Is Generated in Different CulturesDocument22 pagesResilience in A Cross-Cultural Perspective - How Resilience Is Generated in Different Culturesclemence.jensenNo ratings yet
- Practical No. 1 Family Pathology ScaleDocument6 pagesPractical No. 1 Family Pathology Scaleansuka chanuNo ratings yet
- Attachment Theory Final PDF 14.04.14Document16 pagesAttachment Theory Final PDF 14.04.14MaximMadalinaIulianaNo ratings yet
- Thesis Attachment TheoryDocument5 pagesThesis Attachment TheoryHelpWithWritingAPaperForCollegeFargo100% (1)
- Attachment Theory Research Paper TopicsDocument4 pagesAttachment Theory Research Paper Topicsgz83v005100% (1)
- Atasament Si AnxietateDocument20 pagesAtasament Si AnxietateIon GheorgheNo ratings yet
- Acceptance/responsiveness: Parenting StylesDocument6 pagesAcceptance/responsiveness: Parenting Styleshoney torresNo ratings yet
- Social 0 Personality Development in ChildrenDocument17 pagesSocial 0 Personality Development in ChildrenShambhavi ShastryNo ratings yet
- Lesson - Nature and NurtureDocument5 pagesLesson - Nature and NurtureBouz Ikram100% (1)
- Is Insecure Parent - Child Attachment A Risk Factor For The Development of Anxiety in Childhood or Adolescence?Document6 pagesIs Insecure Parent - Child Attachment A Risk Factor For The Development of Anxiety in Childhood or Adolescence?Susan KuriakoseNo ratings yet
- Fulltext PDFDocument53 pagesFulltext PDFJeanette LampitocNo ratings yet
- Aggression and Resilience in Relation To Parenting Styles: ManyapundirDocument6 pagesAggression and Resilience in Relation To Parenting Styles: ManyapundirRoxana ElenaNo ratings yet
- Ijerph 19 01064 v3Document22 pagesIjerph 19 01064 v3Camila Sofía Díaz OyarzúnNo ratings yet
- CDEV-107 - Attachment in InfantsDocument7 pagesCDEV-107 - Attachment in InfantsAlexander OrigamiNo ratings yet
- Screenshot 2023-05-16 at 11.29.57Document3 pagesScreenshot 2023-05-16 at 11.29.57sashairene2000No ratings yet
- SocialrelationshipsDocument13 pagesSocialrelationshipsrey-an riveraNo ratings yet
- Self-Determination Theory - Basic Psychological Needs in Motivation, Development, and Wellness (PDFDrive) (332-372)Document41 pagesSelf-Determination Theory - Basic Psychological Needs in Motivation, Development, and Wellness (PDFDrive) (332-372)Camila SalazarNo ratings yet
- Attachement Parentyng Styles PDFDocument6 pagesAttachement Parentyng Styles PDFOvidiu BerarNo ratings yet
- 03.HG Theories of Child BehaviorDocument9 pages03.HG Theories of Child BehaviorEthel KanadaNo ratings yet
- Attachment Theory of The Children With Autism and Down SyndromeDocument22 pagesAttachment Theory of The Children With Autism and Down SyndromeLucas NavarroNo ratings yet
- Psych Final PaperDocument8 pagesPsych Final PaperAndrew ArvidsonNo ratings yet
- Pfpi Report Final2Document27 pagesPfpi Report Final2TushitaNo ratings yet
- Theory PaperDocument6 pagesTheory Paperapi-649875808No ratings yet
- Attachment and Emotion in School-Aged Children Borelli Emotion 2010Document11 pagesAttachment and Emotion in School-Aged Children Borelli Emotion 2010LisaDarlingNo ratings yet
- Bakermans-Kranenburg Et Al., 2011Document31 pagesBakermans-Kranenburg Et Al., 2011DeniseNo ratings yet
- PSY 052 Module (Topic E)Document7 pagesPSY 052 Module (Topic E)derNo ratings yet
- The Core Sensitivities A Clinical Evolution of Masterson S Disorders of SelfDocument19 pagesThe Core Sensitivities A Clinical Evolution of Masterson S Disorders of SelfChristine YauNo ratings yet
- Effects of Attachment On Early and Later Development: Mokhtar MalekpourDocument15 pagesEffects of Attachment On Early and Later Development: Mokhtar MalekpourJuan Baldana100% (1)
- Liss V. Mariano, MDDocument25 pagesLiss V. Mariano, MDAllan SanchezNo ratings yet
- Harlow's Attachment TheoryDocument8 pagesHarlow's Attachment TheoryAban RobertNo ratings yet
- CPE 103 ReportDocument2 pagesCPE 103 Reporteyefrost06No ratings yet
- Explanatory SynthesisDocument8 pagesExplanatory SynthesisClaire GreenleeNo ratings yet
- Wa0001.1Document10 pagesWa0001.1charityartienda1985No ratings yet
- Research On Cheating Proness-Final PDFDocument11 pagesResearch On Cheating Proness-Final PDFAsiya BatullNo ratings yet
- Issues in The Social and Emotional Adjustment of Gifted ChildrenDocument12 pagesIssues in The Social and Emotional Adjustment of Gifted Childrenapi-301904910No ratings yet
- White Minimalist Travel MagazineDocument7 pagesWhite Minimalist Travel MagazineSeediSowsNo ratings yet
- Are Early Period Maladaptive Schemas Effective in AdolescenceDocument13 pagesAre Early Period Maladaptive Schemas Effective in AdolescenceVincent Miles SustiguerNo ratings yet
- Treating Adult Survivors of Severe Childhood Abuse and Neglect Further Development of An Integrative ModelDocument26 pagesTreating Adult Survivors of Severe Childhood Abuse and Neglect Further Development of An Integrative ModelIoannis K. GeronikosNo ratings yet
- Attachment Theory Is ADocument7 pagesAttachment Theory Is AditeABCNo ratings yet
- Attachment and Foster CareDocument14 pagesAttachment and Foster CareProdan Dumitru DanielNo ratings yet
- Chapter 2 - Sample 2Document15 pagesChapter 2 - Sample 2Je CoNo ratings yet
- The Case of Ms LemonDocument5 pagesThe Case of Ms LemonAshley KateNo ratings yet
- Ang Naging Kamalayan Bunga NG Hiwalayan: Understanding Young Adults' Attitudes Towards Parental SeparationDocument22 pagesAng Naging Kamalayan Bunga NG Hiwalayan: Understanding Young Adults' Attitudes Towards Parental SeparationPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Attachment Theory 2Document3 pagesAttachment Theory 2Hawa MohammedNo ratings yet
- E102 Tma02Document5 pagesE102 Tma02deb.tiff26No ratings yet
- The Resilience of Foster Children The inDocument16 pagesThe Resilience of Foster Children The inKou TarNo ratings yet
- Bowlby, The Strange Situation, and The Developmental NicheDocument7 pagesBowlby, The Strange Situation, and The Developmental NicheVoog100% (2)
- Parent-Child Reunification After Alienation - Psychology TodayDocument6 pagesParent-Child Reunification After Alienation - Psychology TodayFamily Court-CorruptionNo ratings yet
- Psychology Scholarly Paper 1Document11 pagesPsychology Scholarly Paper 1Danial HassanNo ratings yet
- Parent Child Attachment and Problem Behavior Reporting by Mothers With Pathology in Different Socioeconomic StatusDocument12 pagesParent Child Attachment and Problem Behavior Reporting by Mothers With Pathology in Different Socioeconomic StatusSudiptiNo ratings yet
- Parental InvolvementDocument5 pagesParental InvolvementAlexa MarcojosNo ratings yet
- Collins & Feeney, 2013Document6 pagesCollins & Feeney, 2013Romina Adaos OrregoNo ratings yet
- Dissertation Attachment TheoryDocument8 pagesDissertation Attachment TheoryPaySomeoneToWritePaperCanada100% (1)
- Attachment Theory and Child AbuseDocument7 pagesAttachment Theory and Child AbuseAlan Challoner100% (3)
- PD 2Document5 pagesPD 2Krishna BoreddyNo ratings yet
- Shaping Your Child's Healthy Self-Esteem-Self-Worth: Emotional IntelligenceFrom EverandShaping Your Child's Healthy Self-Esteem-Self-Worth: Emotional IntelligenceNo ratings yet
- Strong Roots, Flourishing Futures: The Risks of Over-Coddling in Child DevelopmentFrom EverandStrong Roots, Flourishing Futures: The Risks of Over-Coddling in Child DevelopmentNo ratings yet
- Helpful Hints...: For Helping Your Child Cope with HospitalizationFrom EverandHelpful Hints...: For Helping Your Child Cope with HospitalizationNo ratings yet
- Term Paper Ideas For American GovernmentDocument4 pagesTerm Paper Ideas For American Governmenteaibyfvkg100% (1)
- Practice Toolkit - Eric Silberger - Tonebase Violin WorkbookDocument15 pagesPractice Toolkit - Eric Silberger - Tonebase Violin WorkbookVít237 CzNo ratings yet
- Managing Change in Printing IndustryDocument10 pagesManaging Change in Printing IndustrynaktiruNo ratings yet
- PripremaDocument2 pagesPripremaMaja BoljevicNo ratings yet
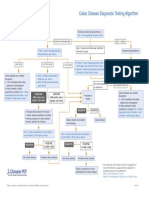
- Celiac Disease Diagnostic Testing AlgorithmDocument1 pageCeliac Disease Diagnostic Testing AlgorithmtarogiosdrakNo ratings yet
- 12 Years A Slave - SummaryDocument2 pages12 Years A Slave - SummaryEnrique SchererNo ratings yet
- Anti-Sexual Harrassment ActDocument30 pagesAnti-Sexual Harrassment ActJ Velasco PeraltaNo ratings yet
- Resume Teaching2016Document1 pageResume Teaching2016api-307736451No ratings yet
- NCERT Solutions For Class 11 English Snapshots Albert Einstein at SchoolDocument10 pagesNCERT Solutions For Class 11 English Snapshots Albert Einstein at SchoolSantanu BorahNo ratings yet
- Shock: Dr. Monica, DR., Span., Kic., MsiDocument29 pagesShock: Dr. Monica, DR., Span., Kic., MsiRyanNo ratings yet
- Civil/Property Matter (Sale, Purchase, Mortgage, Lien, Will, Gift, Ancestral Property) A. What Is Meant by Property in Law?Document14 pagesCivil/Property Matter (Sale, Purchase, Mortgage, Lien, Will, Gift, Ancestral Property) A. What Is Meant by Property in Law?ankitNo ratings yet
- CBS Grand Conversations PDFDocument8 pagesCBS Grand Conversations PDFShin Jeon HyeNo ratings yet
- Sika PDS - E - SikaGrout 214 11Document3 pagesSika PDS - E - SikaGrout 214 11Khin Sandi KoNo ratings yet
- Engleza IiDocument38 pagesEngleza IiFIRA DAN0% (1)
- TheWorldontheTurtlesBack 1Document8 pagesTheWorldontheTurtlesBack 1Kristen GoddardNo ratings yet
- 250+ Questions To Answer in EnglishDocument11 pages250+ Questions To Answer in EnglishOzheni A.100% (1)
- Madeleine LeiningerDocument29 pagesMadeleine LeiningerMae Visperas100% (4)
- Media Studies Coursework Evaluation ExampleDocument7 pagesMedia Studies Coursework Evaluation Examplefvntkabdf100% (2)
- Guidelines To Determine ProfessionDocument5 pagesGuidelines To Determine Professionsurinder sangarNo ratings yet
- Uses of Meditation For Health in The United StatesDocument1 pageUses of Meditation For Health in The United StatesKimi PalgotraNo ratings yet
- Habit 6: Synergize: One WayDocument8 pagesHabit 6: Synergize: One WayMustapha KhanNo ratings yet
- About Iban: Sarawak BidayuhDocument4 pagesAbout Iban: Sarawak BidayuhAmanda HazsmahNo ratings yet
- Specialized Crime Investigation: With Legal MedicineDocument7 pagesSpecialized Crime Investigation: With Legal MedicineApple AsneNo ratings yet
- Tribhuvan University Institute of Science and Technology 2068Document5 pagesTribhuvan University Institute of Science and Technology 2068Sarose MahatNo ratings yet
- A Guide To Confidentiality in Health and Social CareDocument6 pagesA Guide To Confidentiality in Health and Social CareSergio Antonio Morales SarmientoNo ratings yet
- A Case Study On The Ethical Obligations of The Citicorp BuildingDocument3 pagesA Case Study On The Ethical Obligations of The Citicorp BuildingIshfaq Ahmed Miraj100% (2)
- Polya's Steps To Problem Solving...Document20 pagesPolya's Steps To Problem Solving...Almira67% (3)
- 5 Benefits of Equality and Diversity in The WorkplaceDocument3 pages5 Benefits of Equality and Diversity in The WorkplaceMahmood KaderNo ratings yet
- The Sworn Book of HonoriusDocument44 pagesThe Sworn Book of HonoriusJUAN CARLOS TAMAYO NASIRNo ratings yet