Download as pdf or txt
You might also like
- UWorld Notes Step 2Document93 pagesUWorld Notes Step 2Vee Mend100% (1)
- Dissection of The Appendix With Ultrasound-Activated Scalpel - An Experimental Study in Pediatric Laparoscopic Appendectomy (2010)Document6 pagesDissection of The Appendix With Ultrasound-Activated Scalpel - An Experimental Study in Pediatric Laparoscopic Appendectomy (2010)陳玉芝No ratings yet
- Group5 Research Article SummaryDocument4 pagesGroup5 Research Article SummaryJunaimah TataroNo ratings yet
- Flap Surgical Techniques For Incisional Hernia Recurrences. A Swine Experimental ModelDocument9 pagesFlap Surgical Techniques For Incisional Hernia Recurrences. A Swine Experimental ModelFlorina PopaNo ratings yet
- Journal of Oral Biology and Craniofacial ResearchDocument4 pagesJournal of Oral Biology and Craniofacial ResearchRafika OljNo ratings yet
- Vet Radiology Ultrasound - 2023 - Trikoupi - Diagnosis of Traumatic Urethral Stricture in A Canine Patient WithDocument4 pagesVet Radiology Ultrasound - 2023 - Trikoupi - Diagnosis of Traumatic Urethral Stricture in A Canine Patient WithFernando Lucas Costa SilvaNo ratings yet
- His To Logical Changes in Radial Forearm Skin Flaps in The Oral Cavity - DR Darwish Badran - Medics Index MemberDocument6 pagesHis To Logical Changes in Radial Forearm Skin Flaps in The Oral Cavity - DR Darwish Badran - Medics Index MemberMedicsindex Telepin Slidecase100% (1)
- A Long-Term Study of 370 Autotransplanted Premolars.Document11 pagesA Long-Term Study of 370 Autotransplanted Premolars.jing.zhao222No ratings yet
- The Mid-Palatal Suture in Young Adults. 2001Document11 pagesThe Mid-Palatal Suture in Young Adults. 2001Rommy MelgarejoNo ratings yet
- 1 s2.0 S0749806314004009 MainDocument10 pages1 s2.0 S0749806314004009 MainbilourNo ratings yet
- Virtual Biopsy - Confocal MicrosDocument5 pagesVirtual Biopsy - Confocal Microsiulia andreeaNo ratings yet
- ABRAVAS 2 de 9 - Divers 1999 - Reptile EndosDocument8 pagesABRAVAS 2 de 9 - Divers 1999 - Reptile EndosCamilo SantanderNo ratings yet
- Radiotherapy and Oncology: Original ArticleDocument7 pagesRadiotherapy and Oncology: Original ArticleMartín FleiNo ratings yet
- Comparative Anatomical Analysis of The Transcallosal-Transchoroidal and Transcallosal-Transforniceal-Transchoroidal Approaches To The Third VentricleDocument10 pagesComparative Anatomical Analysis of The Transcallosal-Transchoroidal and Transcallosal-Transforniceal-Transchoroidal Approaches To The Third VentricleZeptalanNo ratings yet
- Effects of Primary and Recurrent Sacral Chordoma On The Motor and Nociceptive Function of Hindlimbs in Rats - An Orthotopic Spine ModelDocument12 pagesEffects of Primary and Recurrent Sacral Chordoma On The Motor and Nociceptive Function of Hindlimbs in Rats - An Orthotopic Spine ModelgangligonNo ratings yet
- ABRAVAS 5 de 9 - Hernandez Divers 2007 Liver BXDocument5 pagesABRAVAS 5 de 9 - Hernandez Divers 2007 Liver BXCamilo SantanderNo ratings yet
- Reticular AbscessDocument4 pagesReticular AbscessSasikala KaliapanNo ratings yet
- Release of Obstructing Rectal Cuff Following Transanal Endorectal Pullthrough For Hirschsprung's Disease: A Laparoscopic ApproachDocument3 pagesRelease of Obstructing Rectal Cuff Following Transanal Endorectal Pullthrough For Hirschsprung's Disease: A Laparoscopic ApproachAlia AsgharNo ratings yet
- Abdalla 2017Document3 pagesAbdalla 2017dewaprasatyaNo ratings yet
- Glottic and Skull Indices in Canine Brachycephalic Airway Obstructive SyndromeDocument7 pagesGlottic and Skull Indices in Canine Brachycephalic Airway Obstructive SyndromexupalohNo ratings yet
- Comparison of Flank and Midline Approaches To OvarDocument6 pagesComparison of Flank and Midline Approaches To Ovartrisnaput3No ratings yet
- 3.4 Evaluac Funcion Testicular Nylon Biocomp HUMMDocument7 pages3.4 Evaluac Funcion Testicular Nylon Biocomp HUMMALEXANDRA GOYENECHENo ratings yet
- Scholars Journal of Medical Case Reports: ISSN 2347-6559 (Online) ISSN 2347-9507 (Print)Document2 pagesScholars Journal of Medical Case Reports: ISSN 2347-6559 (Online) ISSN 2347-9507 (Print)galihmuchlishermawanNo ratings yet
- Intrathoracic Challenging Mass Ultrasonographic Video PresentationDocument5 pagesIntrathoracic Challenging Mass Ultrasonographic Video PresentationWorld Journal of Case Reports and Clinical Images (ISSN: 2835-1568) CODEN:USANo ratings yet
- Hum. Reprod.-1996-Wyss-1992-7Document6 pagesHum. Reprod.-1996-Wyss-1992-7Juliana GuerraNo ratings yet
- Rodgers RFID SurgEndosc2007Document3 pagesRodgers RFID SurgEndosc2007白石 真土320D008No ratings yet
- Front of Neck Continued Discovery of This AnatomyDocument4 pagesFront of Neck Continued Discovery of This AnatomyFaisal ShamimNo ratings yet
- Endoscopyinsharks: Michael J. MurrayDocument13 pagesEndoscopyinsharks: Michael J. MurrayDaniela Peña VinascoNo ratings yet
- The Tubarial Salivary Glands. A Potential New Organ at Risk For RadiotherapyDocument7 pagesThe Tubarial Salivary Glands. A Potential New Organ at Risk For RadiotherapyGgNo ratings yet
- My Published Paper 6, AnesthesiaDocument5 pagesMy Published Paper 6, Anesthesiamir sahirNo ratings yet
- Kaufmann 2016 Good Study Bad TimingDocument3 pagesKaufmann 2016 Good Study Bad TimingCamilo SotomayorNo ratings yet
- 05 12 Rizac Militaru 8 CompressedDocument9 pages05 12 Rizac Militaru 8 Compressedkaren barriaNo ratings yet
- Laparoscopic Extraperitoneal Resection of Urachal Cyst: Sun-Il Lee, M.D., Sung-Soo Kim, M.DDocument3 pagesLaparoscopic Extraperitoneal Resection of Urachal Cyst: Sun-Il Lee, M.D., Sung-Soo Kim, M.DNurul Rezki Fitriani AzisNo ratings yet
- ABRAVAS 6 de 9 - Holland 2008 Ultrasound IguanaDocument7 pagesABRAVAS 6 de 9 - Holland 2008 Ultrasound IguanaCamilo SantanderNo ratings yet
- Histological Analysis of Short-Term Vital Reactions in Skin Wounds: Potential Applications in Forensic WorkDocument4 pagesHistological Analysis of Short-Term Vital Reactions in Skin Wounds: Potential Applications in Forensic WorkPujia Cahya AmaliaNo ratings yet
- Guillot Re Au 2009Document6 pagesGuillot Re Au 2009nimaelhajjiNo ratings yet
- Jurnal ReadingDocument4 pagesJurnal ReadingAde Triansyah EmsilNo ratings yet
- Chapter 5: Radiological Anatomy: General AspectsDocument7 pagesChapter 5: Radiological Anatomy: General AspectsYel YuriNo ratings yet
- Real-Time Ultrasound-Guided Paramedian Epidural Access: Evaluation of A Novel In-Plane TechniqueDocument10 pagesReal-Time Ultrasound-Guided Paramedian Epidural Access: Evaluation of A Novel In-Plane TechniqueANGELICANo ratings yet
- A Long-Term Study of 370 Autotransplanted Premolars. Part II. Tooth Survival and Pulp Healing Subsequent To TransplantationDocument11 pagesA Long-Term Study of 370 Autotransplanted Premolars. Part II. Tooth Survival and Pulp Healing Subsequent To TransplantationRudnapon AmornlaksananonNo ratings yet
- Cell Proliferation and Carcinogenesis in The Hamster Cheek Pouch1Document8 pagesCell Proliferation and Carcinogenesis in The Hamster Cheek Pouch1Om PrakashNo ratings yet
- Uterine RuptureDocument3 pagesUterine RuptureAndreaAlexandraNo ratings yet
- Laparoscopic Ovariectomy in Standing Donkeys by Using A New InstrumentDocument8 pagesLaparoscopic Ovariectomy in Standing Donkeys by Using A New InstrumentWahyu Dwi NugrohoNo ratings yet
- Suami, H. & Cols. (2005) - A New Radiographic Cadaver Injection Technique For Investigating The Lymphatic SystemDocument7 pagesSuami, H. & Cols. (2005) - A New Radiographic Cadaver Injection Technique For Investigating The Lymphatic SystemLuca ClementinoNo ratings yet
- Grocuttetal 2023Document5 pagesGrocuttetal 2023Wiseup StudioNo ratings yet
- Endoscopic Wedge Excisions With CO2 Laser For Subglottic Stenosis, 2020Document5 pagesEndoscopic Wedge Excisions With CO2 Laser For Subglottic Stenosis, 2020Araceli BarreraNo ratings yet
- Time Imaging .: Ultrasonography Machine For Veterinary ApplicationDocument22 pagesTime Imaging .: Ultrasonography Machine For Veterinary ApplicationKanhaiyalal RamNo ratings yet
- Histological Analysis of Short-Term Vital ReactionDocument5 pagesHistological Analysis of Short-Term Vital ReactionsellyNo ratings yet
- Mohammed A.H. Abdelhakiem and Mohammed H. ElrashidyDocument12 pagesMohammed A.H. Abdelhakiem and Mohammed H. ElrashidyAprilia PutraNo ratings yet
- Jsls 13 3 327Document5 pagesJsls 13 3 327jorgeluisgt7No ratings yet
- MR Sialography and Conventional Sialography in SalDocument6 pagesMR Sialography and Conventional Sialography in Salshehla khanNo ratings yet
- Hirsbrunner 1998Document5 pagesHirsbrunner 1998Bernardo AlmeidaNo ratings yet
- Hi Rs Brunner 1998Document5 pagesHi Rs Brunner 1998Bernardo AlmeidaNo ratings yet
- IJVST Volume 8 Issue 1 Pages 33-37Document5 pagesIJVST Volume 8 Issue 1 Pages 33-37Chalermrat ApiraknusitNo ratings yet
- Ultrasonography of The Equine Abdomen Techniques and Normal FindingsDocument7 pagesUltrasonography of The Equine Abdomen Techniques and Normal Findingsludiegues752No ratings yet
- An Unusual Cause of Small Bowel ObstructionDocument5 pagesAn Unusual Cause of Small Bowel ObstructionJet Acido GalloNo ratings yet
- Villagomez 2021Document1 pageVillagomez 2021DANIEL ARTEAGA MENDOZANo ratings yet
- 653 FullDocument17 pages653 Fullmantenimiento.servelshNo ratings yet
- OHT Flank ApproachDocument6 pagesOHT Flank ApproachMarinaJiménezNo ratings yet
- Case Report AbdomenDocument5 pagesCase Report Abdomensigario hutamaNo ratings yet
- Dataset For Histopathological Reporting of Primary Invasive Cutaneous Squamous Cell Carcinoma and Regional Lymph NodesDocument57 pagesDataset For Histopathological Reporting of Primary Invasive Cutaneous Squamous Cell Carcinoma and Regional Lymph NodesMajid KhanNo ratings yet
- End-Stage Renal DiseaseDocument4 pagesEnd-Stage Renal DiseaseSuneel Kumar PrajapatiNo ratings yet
- The Hill-Rom® 900 Bed: Simply EfficientDocument12 pagesThe Hill-Rom® 900 Bed: Simply EfficientFelipe R.No ratings yet
- Module 2 PharmacologyDocument7 pagesModule 2 PharmacologyAshley NicoleNo ratings yet
- Back Pain QuestionnaireDocument2 pagesBack Pain QuestionnaireiikemNo ratings yet
- Adrenal DisordersDocument48 pagesAdrenal DisordersMubeenUrRehmanNo ratings yet
- Hemorrhagic Stroke Clinical PresentationDocument11 pagesHemorrhagic Stroke Clinical PresentationAndri wijayaNo ratings yet
- Immuno Oncology Therapies White Paper PPDDocument12 pagesImmuno Oncology Therapies White Paper PPDkevalNo ratings yet
- Đề 9.Mh2022.Key Chi TiếtDocument17 pagesĐề 9.Mh2022.Key Chi Tiếttailieu hienNo ratings yet
- Hospital PharmacyDocument15 pagesHospital PharmacyYet Barreda BasbasNo ratings yet
- Antifungal - Membran SelDocument26 pagesAntifungal - Membran SelHanung PujanggaNo ratings yet
- Oral Contraceptive PillDocument21 pagesOral Contraceptive Pillherlanboga100% (1)
- Nursing Care Plan Sample 2Document9 pagesNursing Care Plan Sample 2GEN ERIGBUAGASNo ratings yet
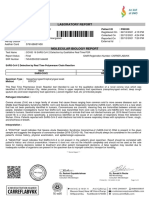
- Laboratory Report: Name: MR .Sandeep Mane Patient ID: P80359Document1 pageLaboratory Report: Name: MR .Sandeep Mane Patient ID: P80359akash srivastavaNo ratings yet
- NovartisDocument18 pagesNovartisAshu NabhiNo ratings yet
- ESI ER CompleteDocument45 pagesESI ER Completetammy2121No ratings yet
- CMO 09 s2007Document55 pagesCMO 09 s2007XtiaRNo ratings yet
- Ehu 281Document62 pagesEhu 281rawahyudiNo ratings yet
- Mime Therapy Is A Combination of Mime and Physiotherapy and Aims To Promote Symmetry of The Face at Rest and During Movement and To Control SynkinesisDocument3 pagesMime Therapy Is A Combination of Mime and Physiotherapy and Aims To Promote Symmetry of The Face at Rest and During Movement and To Control SynkinesisShahnaz Dar100% (1)
- Hearing Problems Associated With Meniere's Disease: By: Atharva, Luca and OmarDocument9 pagesHearing Problems Associated With Meniere's Disease: By: Atharva, Luca and OmarAtharva SatputeNo ratings yet
- Sleep and HeadacheDocument15 pagesSleep and HeadachemarceloataideNo ratings yet
- PacemakerDocument13 pagesPacemakeralainzkie100% (2)
- Dental Health EducationDocument5 pagesDental Health EducationGhabbyFernandezNo ratings yet
- Acupuncture & Oriental Medicine For The FutureDocument51 pagesAcupuncture & Oriental Medicine For The Futureatulsahu24100% (1)
- MS2 - Neurologic Disorder My ReportDocument30 pagesMS2 - Neurologic Disorder My ReportNeil Lansang BallobanNo ratings yet
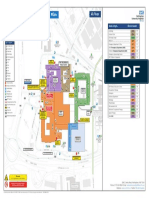
- QMC A Floor 0219 WebDocument1 pageQMC A Floor 0219 Webgoogle manNo ratings yet
- Failure Mode and Effect Analysis (FMEA) Sanglah General Hospital 2012Document28 pagesFailure Mode and Effect Analysis (FMEA) Sanglah General Hospital 2012ferekonstantinusNo ratings yet
- Chapter 3: Legal Aspects of NursingDocument6 pagesChapter 3: Legal Aspects of NursingKaren Joyce Costales MagtanongNo ratings yet
- RetinaDocument61 pagesRetinaapi-3700043No ratings yet