Download as pdf or txt
You might also like
- AO Principles of Fracture Management in The Dog and CatDocument490 pagesAO Principles of Fracture Management in The Dog and CatmafercaavNo ratings yet
- Vanders Chapter 6Document53 pagesVanders Chapter 6gablimlikescheeseNo ratings yet
- Sepsis - 3Document36 pagesSepsis - 3Mohd Ekhwan DarusNo ratings yet
- Antivenom Reactions IntroductionDocument14 pagesAntivenom Reactions IntroductionppgpcsNo ratings yet
- Sepsis: Pathophysiology and Management in The ICUDocument38 pagesSepsis: Pathophysiology and Management in The ICUprashsubbuNo ratings yet
- Sepsis Update 2019Document44 pagesSepsis Update 2019Yeshwanth Umapathi100% (1)
- Sepsis: Pathophysiology and Management in The ICU: Moderator: DR Kavita Rani Sharma Presenter: Dr. PrashanthDocument38 pagesSepsis: Pathophysiology and Management in The ICU: Moderator: DR Kavita Rani Sharma Presenter: Dr. Prashanthprashsubbu100% (1)
- 13.30 DR Arunraj Navaratnarajah - The Septic PatientDocument49 pages13.30 DR Arunraj Navaratnarajah - The Septic PatientagusNo ratings yet
- DR. DR Umar Zein, SP - PD DTM&H - New Generation Antibiotic in SepsisDocument27 pagesDR. DR Umar Zein, SP - PD DTM&H - New Generation Antibiotic in SepsisOlivia DwimaswastiNo ratings yet
- Fluid Resuscitation in SepsisDocument68 pagesFluid Resuscitation in SepsisRonald Ariyanto WiradirnataNo ratings yet
- Current Recommendations For The Management of Severe Sepsis & Septic ShockDocument34 pagesCurrent Recommendations For The Management of Severe Sepsis & Septic ShockAmit KochetaNo ratings yet
- 8.1 - Cases - ViralDocument25 pages8.1 - Cases - Viralkoteshwara raoNo ratings yet
- Surviving Sepsis Campaign - NewDocument21 pagesSurviving Sepsis Campaign - NewIrfan SyakirNo ratings yet
- 16 SepsisDocument125 pages16 SepsisChamindraNo ratings yet
- Sepsis: ManagementDocument50 pagesSepsis: Managementer bcmNo ratings yet
- Recommendations For Sepsis Management in Limited SourcesDocument25 pagesRecommendations For Sepsis Management in Limited SourcesFatahillah NazarNo ratings yet
- W2D3 DR - Yasa-Bacteremia Dan SepsisDocument54 pagesW2D3 DR - Yasa-Bacteremia Dan SepsisJaka BawaviNo ratings yet
- Guideline Sepsis TerbaruDocument81 pagesGuideline Sepsis TerbaruasepNo ratings yet
- PERFUSION monitoring-SYSTEMIC-ghalebDocument49 pagesPERFUSION monitoring-SYSTEMIC-ghalebGHALEB A. AlmekhlafiNo ratings yet
- Pharmacotherapeutics - I: Case Study On Anterior Wall Myocardial InfarctionDocument20 pagesPharmacotherapeutics - I: Case Study On Anterior Wall Myocardial InfarctionDr. Suba Senthil0% (1)
- Sepsis Dhi RifDocument22 pagesSepsis Dhi RifrifdahghofarNo ratings yet
- NullDocument58 pagesNullElteyb Nor eldaimNo ratings yet
- Sepsis SixDocument31 pagesSepsis SixFatin Nurina Mohd NazemiNo ratings yet
- Update On Surviving Sepsis 2008Document34 pagesUpdate On Surviving Sepsis 2008wizardebmNo ratings yet
- Wjem 20 185 PDFDocument6 pagesWjem 20 185 PDFmarinarizkyutamiNo ratings yet
- EGDTDocument33 pagesEGDTaLineLanNo ratings yet
- Sepsis Management: Runal Shah 1 Year Resident MEM, Kdah, MumbaiDocument18 pagesSepsis Management: Runal Shah 1 Year Resident MEM, Kdah, Mumbaibotet_2306No ratings yet
- Prof Djoko - SepsisDocument31 pagesProf Djoko - SepsisfaradillasuciNo ratings yet
- Cva Case STROKEDocument27 pagesCva Case STROKEUmme habeebaNo ratings yet
- Management of Severe Malaria: Paul N HarijantoDocument56 pagesManagement of Severe Malaria: Paul N HarijantoDaniel MatiusNo ratings yet
- Clinical Lab Result Interpretation-2 Dr. Bereket Molla TigabuDocument41 pagesClinical Lab Result Interpretation-2 Dr. Bereket Molla Tigabuphoto copyhemnNo ratings yet
- Sepsis, Severe Sepsis and Septic Shock: 2008 UPDATE J.Tavares, MD, FCCP, FaasmDocument50 pagesSepsis, Severe Sepsis and Septic Shock: 2008 UPDATE J.Tavares, MD, FCCP, FaasmKevin BlancoNo ratings yet
- Upper Gastrointestinal Bleeding 2007Document43 pagesUpper Gastrointestinal Bleeding 2007Matthew ThompsonNo ratings yet
- Surviving Sepsis Campaign 2016 Guidelines Presentation Final RevisiedDocument32 pagesSurviving Sepsis Campaign 2016 Guidelines Presentation Final RevisiedAdli Wafi Jabbar100% (1)
- Emergency 1Document22 pagesEmergency 1eyobs0997No ratings yet
- Laki-Laki, 21 Tahun Dengan Ketoasidosis DiabetikumDocument66 pagesLaki-Laki, 21 Tahun Dengan Ketoasidosis DiabetikumAnonymous gudRSKNo ratings yet
- PGDT Protocol Summary ReferenceDocument32 pagesPGDT Protocol Summary Referenceghg sddNo ratings yet
- Grand Round Case Presentation: by DR Sanjay Khare MD MedicineDocument19 pagesGrand Round Case Presentation: by DR Sanjay Khare MD MedicineHrishikeshNo ratings yet
- SepsisDocument55 pagesSepsisAli SohailNo ratings yet
- Referat Sepsis Dan ARDS - Lea SichiliaDocument24 pagesReferat Sepsis Dan ARDS - Lea SichiliaLea SichiliaNo ratings yet
- DR Paul Harijanto - WS MALARIA-PIN PAPDI-19 PDFDocument33 pagesDR Paul Harijanto - WS MALARIA-PIN PAPDI-19 PDFMukhammadBurhanuddinNo ratings yet
- Sepsis: Nirav Mistry, MD and Adel Bassily-Marcus, MD, FCCP, FCCMDocument3 pagesSepsis: Nirav Mistry, MD and Adel Bassily-Marcus, MD, FCCP, FCCMAli AftabNo ratings yet
- ATLS Advanced Trauma Life SupportDocument54 pagesATLS Advanced Trauma Life SupportdrofiliNo ratings yet
- ATLS Power Point PDFDocument54 pagesATLS Power Point PDFRizky LumalessilNo ratings yet
- Surviving Sepsis: Early Goal Directed TherapyDocument34 pagesSurviving Sepsis: Early Goal Directed Therapyyehezkiel_yesiNo ratings yet
- AtlsDocument32 pagesAtlsMahesh RajwalNo ratings yet
- MS DrillsDocument23 pagesMS DrillsperrsonsummerNo ratings yet
- Kegiatan 3 - Refreshment Lecture Diagnosis Dan Tatalaksana Sepsis Juli 2022Document36 pagesKegiatan 3 - Refreshment Lecture Diagnosis Dan Tatalaksana Sepsis Juli 2022Agnes Irene ZagotoNo ratings yet
- Critical Care Sepsis Presentation-2Document38 pagesCritical Care Sepsis Presentation-2api-456295176100% (2)
- 1tatalaksana Mal-berat-KalbarDocument29 pages1tatalaksana Mal-berat-Kalbarcindy christiantiNo ratings yet
- MR Aki Joe CorporationDocument58 pagesMR Aki Joe CorporationrizkiNo ratings yet
- Management of Severe Malaria: Paul N HarijantoDocument62 pagesManagement of Severe Malaria: Paul N Harijantostivana26No ratings yet
- Surviving Sepsis GuidelinesDocument17 pagesSurviving Sepsis GuidelinesNabil RohaizatNo ratings yet
- Sepsis Bundle by DR - ZakiDocument3 pagesSepsis Bundle by DR - Zakizaki ansariNo ratings yet
- Sepsis: Recognition, Diagnosis and Early Management: DR Muhammad Burhan PashaDocument38 pagesSepsis: Recognition, Diagnosis and Early Management: DR Muhammad Burhan PashapashaNo ratings yet
- Case Report:: Stemi Extensive Anterior OnsetDocument43 pagesCase Report:: Stemi Extensive Anterior OnsetWardah MuskaNo ratings yet
- Sepsis Parte 1Document16 pagesSepsis Parte 1Maria AlejandraNo ratings yet
- Intensive Care Unit (ICU) Manual 2020-21Document146 pagesIntensive Care Unit (ICU) Manual 2020-21anithaNo ratings yet
- Case Presentation of IHD-1Document48 pagesCase Presentation of IHD-122 Prem PatelNo ratings yet
- EMRA Sepsis CardDocument4 pagesEMRA Sepsis Cardsgod34100% (1)
- Hypertension and 24-hour Ambulatory Blood Pressure MonitoringFrom EverandHypertension and 24-hour Ambulatory Blood Pressure MonitoringNo ratings yet
- Finnsonetal 2013 ADWCcomprehensivereviewDocument21 pagesFinnsonetal 2013 ADWCcomprehensivereviewBaronKornNo ratings yet
- YYY Benzoin MechDocument3 pagesYYY Benzoin MechBaronKornNo ratings yet
- Clinical Review: Antidepressant-Induced Hyponatremia in Older AdultsDocument12 pagesClinical Review: Antidepressant-Induced Hyponatremia in Older AdultsBaronKornNo ratings yet
- The Management of Cancer Pain: Nathan I. Cherny, MBBSDocument47 pagesThe Management of Cancer Pain: Nathan I. Cherny, MBBSBaronKornNo ratings yet
- Non-Steroidal Anti-Inflammatory Drugs: Therapeutic EffectsDocument8 pagesNon-Steroidal Anti-Inflammatory Drugs: Therapeutic EffectsBaronKornNo ratings yet
- 09 PT Ed HyponatremiaDocument2 pages09 PT Ed HyponatremiaBaronKornNo ratings yet
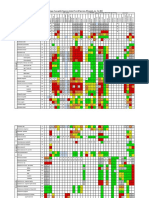
- Organism: Percentage of Susceptible Organisms Isolated From All Specimen, 83 Hospitals, Jan - Dec 2020Document2 pagesOrganism: Percentage of Susceptible Organisms Isolated From All Specimen, 83 Hospitals, Jan - Dec 2020BaronKornNo ratings yet
- Unit 5 Conclusion and DiscussionDocument4 pagesUnit 5 Conclusion and DiscussionBaronKornNo ratings yet
- Hyponatremia Associated With Selective Serotonin-Reuptake Inhibitors in Older AdultsDocument5 pagesHyponatremia Associated With Selective Serotonin-Reuptake Inhibitors in Older AdultsBaronKornNo ratings yet
- Antibiotics 10 01278Document11 pagesAntibiotics 10 01278BaronKornNo ratings yet
- Year One Anatomy and Physiology Study NotesDocument94 pagesYear One Anatomy and Physiology Study Notescoolpinkgurl100% (8)
- RespirationDocument2 pagesRespirationSathyaNo ratings yet
- FORM 86 (Annual Medical Form)Document1 pageFORM 86 (Annual Medical Form)Jairolla ObayNo ratings yet
- Type of Cell FunctionDocument3 pagesType of Cell FunctionDerek Pagsolingan0% (1)
- Biological Psychology Answer Key CIA I NOV.2023Document10 pagesBiological Psychology Answer Key CIA I NOV.2023swethuchlm143No ratings yet
- Luka Bakar Morning ReportDocument24 pagesLuka Bakar Morning ReportUmmatul KhairiyahNo ratings yet
- Blood Donation 1Document10 pagesBlood Donation 1chhayaraviNo ratings yet
- Ecg Interpretation:: The BasicsDocument40 pagesEcg Interpretation:: The BasicsRavi SharmaNo ratings yet
- General Principles of Disorders of Water Balance (Hyponatremia and Hypernatremia) and Sodium Balance (Hypovolemia and Edema) - UpToDateDocument24 pagesGeneral Principles of Disorders of Water Balance (Hyponatremia and Hypernatremia) and Sodium Balance (Hypovolemia and Edema) - UpToDateNedelcu MirunaNo ratings yet
- Ligand Gated Ion ChannelDocument12 pagesLigand Gated Ion ChannelShoaib PatelNo ratings yet
- RML 231223063955Document7 pagesRML 231223063955kumar.manoj269No ratings yet
- The Limbic SystemDocument7 pagesThe Limbic Systemkerima juliaNo ratings yet
- Fisika BioelektrikDocument50 pagesFisika BioelektrikFachriza EffendiNo ratings yet
- Keseimbangan Asam Basa CMDocument47 pagesKeseimbangan Asam Basa CMsyakurNo ratings yet
- Nursing Care Plan For Myocardial InfarctionDocument7 pagesNursing Care Plan For Myocardial InfarctionRocelyn CristobalNo ratings yet
- RHD Case StudyDocument94 pagesRHD Case StudyGel Jovenal100% (1)
- Visceral OMT: AAO Convocation March 2018 Kenneth Lossing DODocument59 pagesVisceral OMT: AAO Convocation March 2018 Kenneth Lossing DODiana SchlittlerNo ratings yet
- A Short History of Physiology in The Netherlands Acta Physiol 2011Document14 pagesA Short History of Physiology in The Netherlands Acta Physiol 2011Nico WesterhofNo ratings yet
- Review Questions: (C) Removal of Nitrogenous WastesDocument15 pagesReview Questions: (C) Removal of Nitrogenous WastesSuinNo ratings yet
- Essay Answers - Model Paper 01Document8 pagesEssay Answers - Model Paper 01ttttNo ratings yet
- Calculate Your Healthy ZoneDocument2 pagesCalculate Your Healthy ZoneJames CarlsonNo ratings yet
- Journal Heptojugular RefluxDocument5 pagesJournal Heptojugular RefluxFarhan RezaNo ratings yet
- Arterial LinesDocument13 pagesArterial LinesYee LengNo ratings yet
- NSTP 122 MidtermDocument2 pagesNSTP 122 MidtermpriagolavinchentNo ratings yet
- Biology S6Document10 pagesBiology S6AKAYEZU Body santiveNo ratings yet
- Pediatric EmergenciesDocument47 pagesPediatric EmergenciesahmedNo ratings yet
- Answers To Exam Practice: Chapter 16 Stimuli, Receptors and ResponsesDocument13 pagesAnswers To Exam Practice: Chapter 16 Stimuli, Receptors and ResponsesTSZ MIU YIPNo ratings yet
- SISS - Diagnostic Adjuncts During Primary SurveyDocument7 pagesSISS - Diagnostic Adjuncts During Primary SurveyPrincy100% (1)