
Frenk and Moon 2013 - Governance Challenges in GH
Frenk and Moon 2013 - Governance Challenges in GH
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- (Nutshell Series.) Carozza, Paolo G. - Glendon, Mary Ann - Picker, Colin B. - Comparative Legal Traditions in A Nutshell-West Academic Publishing (2016) PDFDocument97 pages(Nutshell Series.) Carozza, Paolo G. - Glendon, Mary Ann - Picker, Colin B. - Comparative Legal Traditions in A Nutshell-West Academic Publishing (2016) PDFTuvshinjargal Moyor100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Politics Note CompilationDocument28 pagesPolitics Note Compilationroy kasemaNo ratings yet
- Democracy and Dictatorship in Europe. From The Ancien Régime To The Present Day (SHERI BERMAN 2019)Document561 pagesDemocracy and Dictatorship in Europe. From The Ancien Régime To The Present Day (SHERI BERMAN 2019)vmcos100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- El Momento de La Verdad Jan Carlzon PDF GratisDocument3 pagesEl Momento de La Verdad Jan Carlzon PDF Gratisjon diaz0% (1)
- Acute Pneumonia: Host Defenses and PathogenesisDocument26 pagesAcute Pneumonia: Host Defenses and Pathogenesisjon diazNo ratings yet
- Acute Laryngitis: Formans, Sporothrix Schenckii, and Group GDocument2 pagesAcute Laryngitis: Formans, Sporothrix Schenckii, and Group Gjon diazNo ratings yet
- Reading To Create Strong Illness ScriptsDocument12 pagesReading To Create Strong Illness Scriptsjon diazNo ratings yet
- A Molecular Perspective of Microbial Pathogenicity PDFDocument11 pagesA Molecular Perspective of Microbial Pathogenicity PDFjon diazNo ratings yet
- Lecture Slides Week1Part3Document14 pagesLecture Slides Week1Part3jon diazNo ratings yet
- Whistling in The DarkDocument6 pagesWhistling in The Darkjon diazNo ratings yet
- Case 2 Modulo 3Document4 pagesCase 2 Modulo 3jon diazNo ratings yet
- Tuberculosis Fever Origin UnknowDocument5 pagesTuberculosis Fever Origin Unknowjon diazNo ratings yet
- Autoinflammatory SyndromeDocument7 pagesAutoinflammatory Syndromejon diazNo ratings yet
- Accountability and Transparency Are Treated As Major Building Pillars For Governing Democratic Nations in Recent YearsDocument3 pagesAccountability and Transparency Are Treated As Major Building Pillars For Governing Democratic Nations in Recent YearsAtisha RamsurrunNo ratings yet
- ResearchReport 2008Document64 pagesResearchReport 2008RachelNo ratings yet
- The Global State of Democracy 2022Document64 pagesThe Global State of Democracy 2022TalCualNo ratings yet
- 3993619) Thomas G. Weiss - Governance, Good Governance and Global Governance - Conceptual and Actual ChallengesDocument21 pages3993619) Thomas G. Weiss - Governance, Good Governance and Global Governance - Conceptual and Actual ChallengesLexi BrownNo ratings yet
- A Project On "Emergence of Idea of Codification": JECRC University, JaipurDocument12 pagesA Project On "Emergence of Idea of Codification": JECRC University, JaipurTanmay SinghNo ratings yet
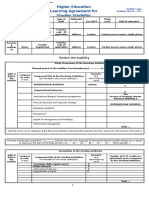
- Higher Education Learning Agreement For Studies Studeifor: Before The MobilityDocument5 pagesHigher Education Learning Agreement For Studies Studeifor: Before The MobilityVincenzo Milazzo0% (1)
- 2018 Eligibility Procedures and Accreditation Standards For Accounting AccreditationDocument35 pages2018 Eligibility Procedures and Accreditation Standards For Accounting AccreditationAndualem ZenebeNo ratings yet
- Ordeshook (1990) - The Emerging Discipline of Political EconomyDocument13 pagesOrdeshook (1990) - The Emerging Discipline of Political EconomyLéo LecomteNo ratings yet
- UCSP Second-Quarter M10Document19 pagesUCSP Second-Quarter M10Tyrone james BelotindosNo ratings yet
- The Role of Leadership Styles in The Administration of Government InstitutionsDocument15 pagesThe Role of Leadership Styles in The Administration of Government InstitutionsInternational Journal of Recent Innovations in Academic ResearchNo ratings yet
- Statement of Inclusion 2016 AustraliaDocument12 pagesStatement of Inclusion 2016 AustraliaIli RaihanaNo ratings yet
- 1Document339 pages1Taposh Owayez MahdeenNo ratings yet
- Religious-Influence-In-Policy-Making-A-Case-Of-Sexual-Education-In-Lithuania - Content File PDFDocument14 pagesReligious-Influence-In-Policy-Making-A-Case-Of-Sexual-Education-In-Lithuania - Content File PDFIonela RotaruNo ratings yet
- WOMANKIND Sections 1 and 2Document26 pagesWOMANKIND Sections 1 and 2Hannah ToresesNo ratings yet
- Ucsp Module 1.2Document32 pagesUcsp Module 1.2Joshua Deguzman PeñarandaNo ratings yet
- Meaning and Nature of Social ChangeDocument12 pagesMeaning and Nature of Social ChangeAryan MehrotraNo ratings yet
- Social Structure Is The Framework ofDocument25 pagesSocial Structure Is The Framework ofAnam DaymaNo ratings yet
- Definition and Scope of Political Science 013037Document1 pageDefinition and Scope of Political Science 013037Miyamoto MusashiNo ratings yet
- Introduction To Sociology - BBA 2ndDocument3 pagesIntroduction To Sociology - BBA 2ndAdnan AhmadNo ratings yet
- Sociology of TourismDocument4 pagesSociology of TourismCarzo Aggy MugyNo ratings yet
- All Ppts. Mods1 9 PDFDocument180 pagesAll Ppts. Mods1 9 PDFPauline Rose AnnNo ratings yet
- Understanding Culture, Society, and Politics: Concepts of Sociology, Anthropology, and The Study of CultureDocument14 pagesUnderstanding Culture, Society, and Politics: Concepts of Sociology, Anthropology, and The Study of CultureLyka Niña PasonNo ratings yet
- SCCD Strategic FrameworkDocument25 pagesSCCD Strategic FrameworkTamunofiniarisa BrownNo ratings yet
- The Railways Safety of Transport Safety of Work and Safety of LifeDocument143 pagesThe Railways Safety of Transport Safety of Work and Safety of LifesaravananNo ratings yet
- Land+Tenure+and+Rights E KasimbaziDocument28 pagesLand+Tenure+and+Rights E KasimbaziHarsh SenNo ratings yet
- Education and Community With Special Reference To Indian SocietyDocument9 pagesEducation and Community With Special Reference To Indian SocietyZhelParedesNo ratings yet
- Roll of Movies and MediaDocument138 pagesRoll of Movies and Mediamanoj_rehash_verma8479No ratings yet















































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- (Nutshell Series.) Carozza, Paolo G. - Glendon, Mary Ann - Picker, Colin B. - Comparative Legal Traditions in A Nutshell-West Academic Publishing (2016) PDFDocument97 pages(Nutshell Series.) Carozza, Paolo G. - Glendon, Mary Ann - Picker, Colin B. - Comparative Legal Traditions in A Nutshell-West Academic Publishing (2016) PDFTuvshinjargal Moyor100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Politics Note CompilationDocument28 pagesPolitics Note Compilationroy kasemaNo ratings yet
- Democracy and Dictatorship in Europe. From The Ancien Régime To The Present Day (SHERI BERMAN 2019)Document561 pagesDemocracy and Dictatorship in Europe. From The Ancien Régime To The Present Day (SHERI BERMAN 2019)vmcos100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- El Momento de La Verdad Jan Carlzon PDF GratisDocument3 pagesEl Momento de La Verdad Jan Carlzon PDF Gratisjon diaz0% (1)
- Acute Pneumonia: Host Defenses and PathogenesisDocument26 pagesAcute Pneumonia: Host Defenses and Pathogenesisjon diazNo ratings yet
- Acute Laryngitis: Formans, Sporothrix Schenckii, and Group GDocument2 pagesAcute Laryngitis: Formans, Sporothrix Schenckii, and Group Gjon diazNo ratings yet
- Reading To Create Strong Illness ScriptsDocument12 pagesReading To Create Strong Illness Scriptsjon diazNo ratings yet
- A Molecular Perspective of Microbial Pathogenicity PDFDocument11 pagesA Molecular Perspective of Microbial Pathogenicity PDFjon diazNo ratings yet
- Lecture Slides Week1Part3Document14 pagesLecture Slides Week1Part3jon diazNo ratings yet
- Whistling in The DarkDocument6 pagesWhistling in The Darkjon diazNo ratings yet
- Case 2 Modulo 3Document4 pagesCase 2 Modulo 3jon diazNo ratings yet
- Tuberculosis Fever Origin UnknowDocument5 pagesTuberculosis Fever Origin Unknowjon diazNo ratings yet
- Autoinflammatory SyndromeDocument7 pagesAutoinflammatory Syndromejon diazNo ratings yet
- Accountability and Transparency Are Treated As Major Building Pillars For Governing Democratic Nations in Recent YearsDocument3 pagesAccountability and Transparency Are Treated As Major Building Pillars For Governing Democratic Nations in Recent YearsAtisha RamsurrunNo ratings yet
- ResearchReport 2008Document64 pagesResearchReport 2008RachelNo ratings yet
- The Global State of Democracy 2022Document64 pagesThe Global State of Democracy 2022TalCualNo ratings yet
- 3993619) Thomas G. Weiss - Governance, Good Governance and Global Governance - Conceptual and Actual ChallengesDocument21 pages3993619) Thomas G. Weiss - Governance, Good Governance and Global Governance - Conceptual and Actual ChallengesLexi BrownNo ratings yet
- A Project On "Emergence of Idea of Codification": JECRC University, JaipurDocument12 pagesA Project On "Emergence of Idea of Codification": JECRC University, JaipurTanmay SinghNo ratings yet
- Higher Education Learning Agreement For Studies Studeifor: Before The MobilityDocument5 pagesHigher Education Learning Agreement For Studies Studeifor: Before The MobilityVincenzo Milazzo0% (1)
- 2018 Eligibility Procedures and Accreditation Standards For Accounting AccreditationDocument35 pages2018 Eligibility Procedures and Accreditation Standards For Accounting AccreditationAndualem ZenebeNo ratings yet
- Ordeshook (1990) - The Emerging Discipline of Political EconomyDocument13 pagesOrdeshook (1990) - The Emerging Discipline of Political EconomyLéo LecomteNo ratings yet
- UCSP Second-Quarter M10Document19 pagesUCSP Second-Quarter M10Tyrone james BelotindosNo ratings yet
- The Role of Leadership Styles in The Administration of Government InstitutionsDocument15 pagesThe Role of Leadership Styles in The Administration of Government InstitutionsInternational Journal of Recent Innovations in Academic ResearchNo ratings yet
- Statement of Inclusion 2016 AustraliaDocument12 pagesStatement of Inclusion 2016 AustraliaIli RaihanaNo ratings yet
- 1Document339 pages1Taposh Owayez MahdeenNo ratings yet
- Religious-Influence-In-Policy-Making-A-Case-Of-Sexual-Education-In-Lithuania - Content File PDFDocument14 pagesReligious-Influence-In-Policy-Making-A-Case-Of-Sexual-Education-In-Lithuania - Content File PDFIonela RotaruNo ratings yet
- WOMANKIND Sections 1 and 2Document26 pagesWOMANKIND Sections 1 and 2Hannah ToresesNo ratings yet
- Ucsp Module 1.2Document32 pagesUcsp Module 1.2Joshua Deguzman PeñarandaNo ratings yet
- Meaning and Nature of Social ChangeDocument12 pagesMeaning and Nature of Social ChangeAryan MehrotraNo ratings yet
- Social Structure Is The Framework ofDocument25 pagesSocial Structure Is The Framework ofAnam DaymaNo ratings yet
- Definition and Scope of Political Science 013037Document1 pageDefinition and Scope of Political Science 013037Miyamoto MusashiNo ratings yet
- Introduction To Sociology - BBA 2ndDocument3 pagesIntroduction To Sociology - BBA 2ndAdnan AhmadNo ratings yet
- Sociology of TourismDocument4 pagesSociology of TourismCarzo Aggy MugyNo ratings yet
- All Ppts. Mods1 9 PDFDocument180 pagesAll Ppts. Mods1 9 PDFPauline Rose AnnNo ratings yet
- Understanding Culture, Society, and Politics: Concepts of Sociology, Anthropology, and The Study of CultureDocument14 pagesUnderstanding Culture, Society, and Politics: Concepts of Sociology, Anthropology, and The Study of CultureLyka Niña PasonNo ratings yet
- SCCD Strategic FrameworkDocument25 pagesSCCD Strategic FrameworkTamunofiniarisa BrownNo ratings yet
- The Railways Safety of Transport Safety of Work and Safety of LifeDocument143 pagesThe Railways Safety of Transport Safety of Work and Safety of LifesaravananNo ratings yet
- Land+Tenure+and+Rights E KasimbaziDocument28 pagesLand+Tenure+and+Rights E KasimbaziHarsh SenNo ratings yet
- Education and Community With Special Reference To Indian SocietyDocument9 pagesEducation and Community With Special Reference To Indian SocietyZhelParedesNo ratings yet
- Roll of Movies and MediaDocument138 pagesRoll of Movies and Mediamanoj_rehash_verma8479No ratings yet