Download as pdf or txt
You might also like
- Mobile Forensic Investigations A Guide To Evidence Collection Analysis and Presentation 1St Edition Reiber Full ChapterDocument67 pagesMobile Forensic Investigations A Guide To Evidence Collection Analysis and Presentation 1St Edition Reiber Full Chapterrita.smith780100% (19)
- Test Bank For The Dynamic Child 1st Canadian Edition Franklin R Manis Alissa PencerDocument22 pagesTest Bank For The Dynamic Child 1st Canadian Edition Franklin R Manis Alissa Pencerleahjamescwkqpobnet100% (47)
- AT2512C Eng 01 953804Document2 pagesAT2512C Eng 01 953804Victor Hugo Benitez PaezNo ratings yet
- Checklist Bank Branch AuditDocument5 pagesChecklist Bank Branch AuditPratik Sankpal0% (1)
- Esophageal AtresiaDocument18 pagesEsophageal AtresiaNeha RathoreNo ratings yet
- Pyloric Stenosis: CLASS:-B.Sc. Nursing 3 YearDocument38 pagesPyloric Stenosis: CLASS:-B.Sc. Nursing 3 YearshikhaNo ratings yet
- Temple Run PDFDocument73 pagesTemple Run PDFM. Saleem100% (1)
- Lec 1Document52 pagesLec 1zainabd1964No ratings yet
- Pyloric StenosisDocument5 pagesPyloric StenosisfdgrgNo ratings yet
- Patient Scenario, Chapter 45, Nursing Care of A Family When A Child Has A Gastrointestinal DisorderDocument93 pagesPatient Scenario, Chapter 45, Nursing Care of A Family When A Child Has A Gastrointestinal DisorderDay MedsNo ratings yet
- Pyloric Stenosis Case StudyDocument37 pagesPyloric Stenosis Case StudyFaith Torralba100% (3)
- Canine PyometraDocument5 pagesCanine Pyometrammary09No ratings yet
- Pyloric StenosisDocument5 pagesPyloric Stenosisensoooooooooo100% (1)
- Pyloric Stenosis: CLASS:-B.Sc. Nursing 3 YearDocument38 pagesPyloric Stenosis: CLASS:-B.Sc. Nursing 3 Yearshikha100% (2)
- Nursing Care of Children With Indian Childhood Cirrhosis, Wilsons Disesase, Reyes SyndromeDocument26 pagesNursing Care of Children With Indian Childhood Cirrhosis, Wilsons Disesase, Reyes SyndromeDivya Nair100% (2)
- Pyloric Stenosis: Supervisor: DR NTAGANDA Edmond, Consultant Ped SurgDocument21 pagesPyloric Stenosis: Supervisor: DR NTAGANDA Edmond, Consultant Ped SurgJames NTEGEREJIMANANo ratings yet
- University of Mosul / College of Nursing Child and Adolescent Health NursingDocument11 pagesUniversity of Mosul / College of Nursing Child and Adolescent Health NursingRayan AhmedNo ratings yet
- Pyloric StenosisDocument3 pagesPyloric Stenosismagisasamundo100% (1)
- Pyloric Stenosis WDocument11 pagesPyloric Stenosis WKlaue Neiv CallaNo ratings yet
- Nec 2018Document33 pagesNec 2018Abraham AnaelyNo ratings yet
- 4 PART 2 Nursing Management of Newborn at Risk 2nd Semester 1Document20 pages4 PART 2 Nursing Management of Newborn at Risk 2nd Semester 1ammarNo ratings yet
- PBL No Bowel Output in NeonatesDocument24 pagesPBL No Bowel Output in NeonatesOTOH RAYA OMARNo ratings yet
- Hirschsprung Disease (Aganglionic Megacolon)Document6 pagesHirschsprung Disease (Aganglionic Megacolon)Julliza Joy PandiNo ratings yet
- 10.5 Hirschprungs Disease& VOLVULUS Necrotizing EnterocolitisDocument28 pages10.5 Hirschprungs Disease& VOLVULUS Necrotizing EnterocolitisChristina YounasNo ratings yet
- Hirschsprung'S Disease (Megacolon) : Mrs. Smitha.M Associate Professor Vijaya College of Nursing KottarakkaraDocument6 pagesHirschsprung'S Disease (Megacolon) : Mrs. Smitha.M Associate Professor Vijaya College of Nursing KottarakkarakrishnasreeNo ratings yet
- Pyloric StenosisDocument5 pagesPyloric StenosisMichael AlexanderNo ratings yet
- Acute Abdominal Pain InInfants and ChildrenDocument14 pagesAcute Abdominal Pain InInfants and Childrenemergency.fumcNo ratings yet
- Pyloric StenosisDocument18 pagesPyloric StenosisAnkita Samanta0% (1)
- Pyloric StenosisDocument20 pagesPyloric Stenosisjohnfoday2022No ratings yet
- GI DisordersDocument80 pagesGI DisordersjoycechicagoNo ratings yet
- Congenital Anomalies of GiDocument94 pagesCongenital Anomalies of GiPadmaNo ratings yet
- OmphaloceleDocument23 pagesOmphaloceleFred PupeNo ratings yet
- Pyloric Stenosis ChibuezeDocument12 pagesPyloric Stenosis ChibuezeChibueze AfugbuomNo ratings yet
- High Risk Pediatric Conditions and DisordersDocument80 pagesHigh Risk Pediatric Conditions and DisordersJaezee RamosNo ratings yet
- 3 Common Pediatric Surgery ContinuedDocument5 pages3 Common Pediatric Surgery ContinuedMohamed Al-zichrawyNo ratings yet
- Nursing Care of The Child With Gastrointestinal DisordersDocument50 pagesNursing Care of The Child With Gastrointestinal Disordersمهند الرحيليNo ratings yet
- Week 8 Pedia Pediatric GI DisturbancesDocument110 pagesWeek 8 Pedia Pediatric GI DisturbancesJaja ManezNo ratings yet
- PrematurityDocument37 pagesPrematuritySolomon AmosNo ratings yet
- HirschsprungDocument14 pagesHirschsprungmmodimaano.2202092.chasnNo ratings yet
- Infantile Hypertrophic Pyloric StenosisDocument25 pagesInfantile Hypertrophic Pyloric StenosisPirapong Invalueable KunokNo ratings yet
- Neonatal Acute Abdomen. 7th YrDocument54 pagesNeonatal Acute Abdomen. 7th YrFreeburn SimunchembuNo ratings yet
- Review UNIT XI High Risk NewbornDocument20 pagesReview UNIT XI High Risk NewbornShehana ShihabNo ratings yet
- Pyloric Stenosis OriginalDocument66 pagesPyloric Stenosis OriginalNITHA KNo ratings yet
- Genitourinary Alterations in Chldren: Heather BuccelloDocument46 pagesGenitourinary Alterations in Chldren: Heather BuccelloshanikaNo ratings yet
- Pediatric G.I Disorders FinalDocument53 pagesPediatric G.I Disorders FinalRashid Hussain0% (1)
- Hypertrophic Pyloric StenosisDocument17 pagesHypertrophic Pyloric StenosisMohammed Fareed100% (1)
- Textbook DiscussionDocument6 pagesTextbook DiscussionHahak UkukNo ratings yet
- Paediatric Surgery 2Document38 pagesPaediatric Surgery 2عمار عارفNo ratings yet
- Pyloric StenosisDocument4 pagesPyloric StenosisAaliyaan KhanNo ratings yet
- CASE STUDY Quiane 1Document16 pagesCASE STUDY Quiane 1BeBs jai SelasorNo ratings yet
- Askep HisprungDocument25 pagesAskep HisprungRika AmaliyaNo ratings yet
- Pediatric Care Online AAPDocument18 pagesPediatric Care Online AAPNikola StojsicNo ratings yet
- Bishaw Assigment of GI DisorderDocument98 pagesBishaw Assigment of GI DisorderRas Siko SafoNo ratings yet
- Infantile Pyloric StenosisDocument6 pagesInfantile Pyloric StenosisAksha PraiselinNo ratings yet
- ABORTIONDocument10 pagesABORTIONSivi Joseph100% (1)
- Congenital Hypertrophic Pyloric Stenosis: Dr. Kundan Department of Surgery Patna Medical College & HospitalDocument17 pagesCongenital Hypertrophic Pyloric Stenosis: Dr. Kundan Department of Surgery Patna Medical College & HospitalChamika HuruggamuwaNo ratings yet
- Cervical Polyps: Pharm. Emaediong EmmanuelDocument24 pagesCervical Polyps: Pharm. Emaediong EmmanuelEsther UwehNo ratings yet
- Pyloric Stenosis PDFDocument3 pagesPyloric Stenosis PDFKiiza AloysiusNo ratings yet
- Oesophageal Atresia by GabriellaDocument7 pagesOesophageal Atresia by GabriellaGabrielleNo ratings yet
- Neonatal Anaesthesia 2 Anaesthesia For Neonates With Abdominal Wall DefectsDocument10 pagesNeonatal Anaesthesia 2 Anaesthesia For Neonates With Abdominal Wall DefectsDr. Anish GolchhaNo ratings yet
- Anaesthetic Management of Paediatric Emergencies Corrected 3Document51 pagesAnaesthetic Management of Paediatric Emergencies Corrected 3oriaboseNo ratings yet
- Presented By-Sanghpriya B.SC (N) 3 YearDocument43 pagesPresented By-Sanghpriya B.SC (N) 3 YearbellaNo ratings yet
- Case-Report-DraftDocument5 pagesCase-Report-DraftCricelle Rose CobreNo ratings yet
- Dysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Mule Core ComponentsDocument7 pagesMule Core ComponentsRameshChNo ratings yet
- Data Science and Applied AI Postdoctoral Scholars Program: CandidatesDocument3 pagesData Science and Applied AI Postdoctoral Scholars Program: CandidatesKairosNo ratings yet
- ER00198 V 2000 LG Ed1 CE PDFDocument540 pagesER00198 V 2000 LG Ed1 CE PDFdgdgfgfNo ratings yet
- A Complete Manual On Ornamental Fish Culture: January 2013Document222 pagesA Complete Manual On Ornamental Fish Culture: January 2013Carlos MorenoNo ratings yet
- Technical CollegesDocument228 pagesTechnical CollegesRupak TiwariNo ratings yet
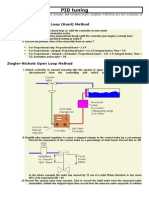
- PID TuningDocument4 pagesPID TuningJitendra Kumar100% (1)
- Q & A ReliablityDocument6 pagesQ & A ReliablitypkcdubNo ratings yet
- Reading and Writing Via CodeDocument7 pagesReading and Writing Via CodedaviqueirozdemedeirosNo ratings yet
- Derivatives - Practice QuestionsDocument4 pagesDerivatives - Practice QuestionsAdil AnwarNo ratings yet
- Professional Reflection Module 2 For CalStateTEACH Credential ProgramDocument8 pagesProfessional Reflection Module 2 For CalStateTEACH Credential ProgramSal V Gonzalez JrNo ratings yet
- Helicopter Automatic Flight Control Sysms Afcs PDFDocument9 pagesHelicopter Automatic Flight Control Sysms Afcs PDFمنذر كمالNo ratings yet
- Network Layer Routing in Packet Networks Shortest Path RoutingDocument45 pagesNetwork Layer Routing in Packet Networks Shortest Path RoutingHalder SubhasNo ratings yet
- 9 Data Entry Interview Questions and AnswersDocument2 pages9 Data Entry Interview Questions and AnswersBIRIGITA AUKANo ratings yet
- Origin Search (DINT) : - NCCPU051 - Home - DINT: EN ON OFFDocument2 pagesOrigin Search (DINT) : - NCCPU051 - Home - DINT: EN ON OFFbobNo ratings yet
- Objectives Overview: Discovering Computers Fundamentals Fundamentals, 2012 EditionDocument17 pagesObjectives Overview: Discovering Computers Fundamentals Fundamentals, 2012 Editionkeith magakaNo ratings yet
- Robin ZupancDocument3 pagesRobin Zupancnemanja aleksicNo ratings yet
- CASE PRESENTATION K B PeethambaramDocument22 pagesCASE PRESENTATION K B PeethambarammohanNo ratings yet
- LML 6002 Task 2Document9 pagesLML 6002 Task 2hind.ausNo ratings yet
- Artificial Intelligence:: Implications For Business StrategyDocument12 pagesArtificial Intelligence:: Implications For Business StrategyWilliam PolhmannNo ratings yet
- Format Punchlist PDFDocument27 pagesFormat Punchlist PDFDuan Tokcer100% (2)
- 300Q-5 Quintuplex Plunger PumpDocument2 pages300Q-5 Quintuplex Plunger PumpJuanNo ratings yet
- Percona MySQL Support Services For Better Application PerformanceDocument6 pagesPercona MySQL Support Services For Better Application PerformanceGhanshyam BaviskarNo ratings yet
- Shareholders AgreementDocument12 pagesShareholders Agreementmetareason100% (1)
- Sap Service Description For Managed Services Ams English v04 2016Document16 pagesSap Service Description For Managed Services Ams English v04 2016Karthick MNo ratings yet
- National Sample Survey OfficeDocument3 pagesNational Sample Survey OfficeDeepak Dixit0% (2)