Download as pdf or txt
You might also like
- The Health and Work Questionnaire HWQ An InstrumenDocument124 pagesThe Health and Work Questionnaire HWQ An InstrumenLorraine VillanuevaNo ratings yet
- 1 s2.0 S0002937815023509 MainDocument11 pages1 s2.0 S0002937815023509 Mainwoman in progressNo ratings yet
- Pediatric JournalDocument11 pagesPediatric JournalHenny WijayaNo ratings yet
- 2018-Journal of The American Geriatrics SocietyDocument369 pages2018-Journal of The American Geriatrics SocietyKevin PatrickNo ratings yet
- PIIS1098301514020567Document2 pagesPIIS1098301514020567Defriyan RamziNo ratings yet
- Farez2011 PDFDocument10 pagesFarez2011 PDFAdindhya Saraswati SuryaNo ratings yet
- Joc05039 1610 1616 PDFDocument7 pagesJoc05039 1610 1616 PDFDubster OneXNo ratings yet
- Appraisal Worksheet Harm 2016 JssDocument6 pagesAppraisal Worksheet Harm 2016 JssAungo Htet Ko PersiNo ratings yet
- SMJ 64 88Document2 pagesSMJ 64 88felipe duarteNo ratings yet
- Ehp.10816 Spatial EpidDocument6 pagesEhp.10816 Spatial EpidUPTD Puskesmas BadauNo ratings yet
- Chan (2018)Document16 pagesChan (2018)Aprilla Ayu WulandariNo ratings yet
- National Survey of Factors Associated With Repeated Admissions Due To Febrile SeizureDocument4 pagesNational Survey of Factors Associated With Repeated Admissions Due To Febrile Seizurehilman lesmanaNo ratings yet
- Diagnostic DecisionsDocument26 pagesDiagnostic DecisionsBraulioNo ratings yet
- Musculoskeletal Disorders Among First-Year Ghanaian Students in A Nursing CollegeDocument3 pagesMusculoskeletal Disorders Among First-Year Ghanaian Students in A Nursing Collegejanuar rizqiNo ratings yet
- Reports: Chronically Depressed Mood and Cancer Risk in Older PersonsDocument6 pagesReports: Chronically Depressed Mood and Cancer Risk in Older PersonsLeFührer Zabdiel PazaranNo ratings yet
- Koch 2009Document9 pagesKoch 2009Intan Kartika NursyahbaniNo ratings yet
- The Costs of Nosocomial InfectionsDocument4 pagesThe Costs of Nosocomial InfectionsCandra BumiNo ratings yet
- JurnalDocument6 pagesJurnalIzzyNo ratings yet
- Assessment of Pain, Acceptance of Illness, Adjustment To Life With Cancer, and Coping Strategies in Colorectal Cancer PatientsDocument9 pagesAssessment of Pain, Acceptance of Illness, Adjustment To Life With Cancer, and Coping Strategies in Colorectal Cancer PatientsdwiyantoroNo ratings yet
- 903 FullDocument1 page903 FullGetachew MulatNo ratings yet
- Lest The Tide Return ChestDocument3 pagesLest The Tide Return Chestduarte060223No ratings yet
- Nejmp 1215594Document4 pagesNejmp 1215594Cj AlmazanNo ratings yet
- Decadron vs. Pred in Ped AsthmaDocument7 pagesDecadron vs. Pred in Ped AsthmaAndrew JoshuaNo ratings yet
- Hudson 2003Document10 pagesHudson 2003Borja Recuenco CayuelaNo ratings yet
- AntibióticoDocument3 pagesAntibióticoIago RamirezNo ratings yet
- Labor Induction Vs Expectant Management of Lowrisk Pregnancy 2018Document3 pagesLabor Induction Vs Expectant Management of Lowrisk Pregnancy 2018Maria MogosNo ratings yet
- Daniels Et Al (2015) 508Document9 pagesDaniels Et Al (2015) 508Forum PompieriiNo ratings yet
- BNT162b2 mRNA Covid-19 Vaccine in A Nationwide Mass Vaccination SettingDocument12 pagesBNT162b2 mRNA Covid-19 Vaccine in A Nationwide Mass Vaccination SettingMushtofa KamalNo ratings yet
- Jama Oster 2022 Oi 210145 1647635624.12259Document10 pagesJama Oster 2022 Oi 210145 1647635624.12259Zoltán BaloghNo ratings yet
- Coronary Artery Calcium Scoring: Are We There Yet?Document3 pagesCoronary Artery Calcium Scoring: Are We There Yet?GyanNurmaindahHendiantiNo ratings yet
- Sharda 2019Document3 pagesSharda 2019Lilian Elisa HernándezNo ratings yet
- Pneumonia in The Immunocompetent Child ETDocument32 pagesPneumonia in The Immunocompetent Child ETVianney OlveraNo ratings yet
- Jamapediatrics Wu 2020 VP 200014 1598544896.56465Document2 pagesJamapediatrics Wu 2020 VP 200014 1598544896.56465apeachNo ratings yet
- Burden of Serious Harms From Diagnostic Error in The USADocument12 pagesBurden of Serious Harms From Diagnostic Error in The USACBS PhiladelphiaNo ratings yet
- 2010 - Epidemioloy of Ulcerative Keratitis in Northern CaliforniaDocument7 pages2010 - Epidemioloy of Ulcerative Keratitis in Northern CaliforniaPrasetya AnugrahNo ratings yet
- Rajappa 2019Document6 pagesRajappa 2019abdulrazaqNo ratings yet
- Depression Screening Post Partum AJOG 2012 2Document4 pagesDepression Screening Post Partum AJOG 2012 2noam tiroshNo ratings yet
- Ournal of Linical Ncology: PurposeDocument11 pagesOurnal of Linical Ncology: PurposeRicky Cornelius TariganNo ratings yet
- Rello 2016 Septic Shock in The Era of Precision MedicineDocument2 pagesRello 2016 Septic Shock in The Era of Precision MedicineAndreeaPopescuNo ratings yet
- Correspondence: Cited or Read?Document1 pageCorrespondence: Cited or Read?AbdulAzizNo ratings yet
- Midterm Second Activity (Journal) (Valdez Edmark, Moises) Bsn-4Document24 pagesMidterm Second Activity (Journal) (Valdez Edmark, Moises) Bsn-4Edmarkmoises ValdezNo ratings yet
- Metastatic Behavior of Breast Cancer Subtypes: Ournal of Linical NcologyDocument7 pagesMetastatic Behavior of Breast Cancer Subtypes: Ournal of Linical NcologyJafet Gonzalez EstradaNo ratings yet
- ADE in Emergency-2002Document10 pagesADE in Emergency-2002szubiedi816780No ratings yet
- Am. J. Epidemiol. 1997 Schaubel 450 8Document9 pagesAm. J. Epidemiol. 1997 Schaubel 450 8Madhu EvuriNo ratings yet
- Clasificacion Asa en Gestantes 2006Document3 pagesClasificacion Asa en Gestantes 2006salva67333No ratings yet
- Leptin rs2167270 G A (G19A) Polymorphism May Decrease The Risk of Cancer: A Case Control Study and Meta Analysis Involving 19 989 SubjectsDocument10 pagesLeptin rs2167270 G A (G19A) Polymorphism May Decrease The Risk of Cancer: A Case Control Study and Meta Analysis Involving 19 989 SubjectsAlfa FebriandaNo ratings yet
- Irwin 2006Document6 pagesIrwin 2006FerryFitriyaAyuAndikaNo ratings yet
- 10 1002@pbc 27697Document8 pages10 1002@pbc 27697Ravi JhaNo ratings yet
- Am. J. Epidemiol. 2011 Arbogast 613 20Document8 pagesAm. J. Epidemiol. 2011 Arbogast 613 20Amelia Yunira PratiwiNo ratings yet
- Reference 333Document123 pagesReference 333sabrinaNo ratings yet
- Monte Carlo Simulations Estimating Fetal Dose For A Range of Gestational Age and Patient SizeDocument10 pagesMonte Carlo Simulations Estimating Fetal Dose For A Range of Gestational Age and Patient SizeCarlos AlamanNo ratings yet
- Nejmoa 2110475Document14 pagesNejmoa 2110475Luis Ricardo Vejar FelixNo ratings yet
- Craniopharyngioma 2 PDFDocument9 pagesCraniopharyngioma 2 PDFBea NufuarNo ratings yet
- Risk Assessment in Infection Control Which RisksDocument2 pagesRisk Assessment in Infection Control Which RiskspedroaorNo ratings yet
- Jurnal 1Document11 pagesJurnal 1Aulia CahyaniNo ratings yet
- Articulo Cirgua Musinoso Nodulos NegtivDocument10 pagesArticulo Cirgua Musinoso Nodulos NegtivJorge VintimillaNo ratings yet
- Jco 2016 71 3404Document11 pagesJco 2016 71 3404ines rodriguesNo ratings yet
- Jurnal Global Health Prevalens DM Pada TB AktifDocument13 pagesJurnal Global Health Prevalens DM Pada TB AktiftamiFUNo ratings yet
- S2 Epidemiologi - Confounding VariableDocument24 pagesS2 Epidemiologi - Confounding VariableaweningtyasNo ratings yet
- Precision in Pulmonary, Critical Care, and Sleep Medicine: A Clinical and Research GuideFrom EverandPrecision in Pulmonary, Critical Care, and Sleep Medicine: A Clinical and Research GuideJose L. GomezNo ratings yet
- Resilience Is About How You RechargeDocument5 pagesResilience Is About How You Rechargengjx8bj9sxNo ratings yet
- How To Embrace Change Using Emotional IntelligenceDocument4 pagesHow To Embrace Change Using Emotional Intelligencengjx8bj9sxNo ratings yet
- Evidence of Polyethylene BiodegradationDocument9 pagesEvidence of Polyethylene Biodegradationngjx8bj9sxNo ratings yet
- JChemEd - 11 - November 1980 - pp801Document4 pagesJChemEd - 11 - November 1980 - pp801ngjx8bj9sxNo ratings yet
- Ih - Osha 2022Document15 pagesIh - Osha 2022Nursyafiq Ali Shibramulisi100% (1)
- Our Moms Our Babies The State of Maternal and Infant Health in Cincinnati and Hamilton CountyDocument7 pagesOur Moms Our Babies The State of Maternal and Infant Health in Cincinnati and Hamilton CountyGerman Lopez100% (1)
- Utk Thesis DefenseDocument5 pagesUtk Thesis Defenseafcnwwgnt100% (2)
- Chapter 6Document68 pagesChapter 6Restie TeanoNo ratings yet
- 06 Biofuels Mechanical IntegrityDocument26 pages06 Biofuels Mechanical IntegrityEngr Ali100% (1)
- Candidiasis - Red and White Manifestations in The Oral CavityDocument8 pagesCandidiasis - Red and White Manifestations in The Oral CavityFajarRahmantiyoNo ratings yet
- Working at HeightDocument22 pagesWorking at Heightghada gattouchNo ratings yet
- BTEC FIRST IN SPORT UNIT 1 Assignment BookletDocument8 pagesBTEC FIRST IN SPORT UNIT 1 Assignment BookletMagin1981No ratings yet
- Postpartum DepressionDocument1 pagePostpartum DepressionNirmala BhattNo ratings yet
- Mary Janet C. Gorriceta Blk. 21 Zone 3 Bo - Obrero Iloilo City Mobile #: 09302029037 E-Mail AddressDocument8 pagesMary Janet C. Gorriceta Blk. 21 Zone 3 Bo - Obrero Iloilo City Mobile #: 09302029037 E-Mail AddressDick Morgan FerrerNo ratings yet
- A Is Emergency CodeDocument7 pagesA Is Emergency CodeAkansha SharmaNo ratings yet
- Health Declaration Form: (Buong Pangalan) (Petsa) (Oras) (Kasa/ukuyang Tirahan) : (Numero NG Telepono)Document1 pageHealth Declaration Form: (Buong Pangalan) (Petsa) (Oras) (Kasa/ukuyang Tirahan) : (Numero NG Telepono)LANI GUIASILONNo ratings yet
- Practice Paper For Social Studies 2018Document6 pagesPractice Paper For Social Studies 2018shahrilmohdshahNo ratings yet
- Mancini 2008Document8 pagesMancini 2008StelianNo ratings yet
- Informative SpeechDocument3 pagesInformative Speechapi-534130899No ratings yet
- Clowes Brian - Case Against Condoms Death by LatexDocument36 pagesClowes Brian - Case Against Condoms Death by LatexGHP1967No ratings yet
- Patch TestingDocument1 pagePatch Testing26 ThufailNo ratings yet
- First Summative Test in Physical EducationDocument2 pagesFirst Summative Test in Physical EducationDainielle Marie PascualNo ratings yet
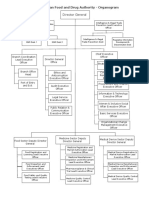
- EFDA Organogram English VersionDocument6 pagesEFDA Organogram English VersionRobsan YasinNo ratings yet
- Hepatitis B Immunization Health History FormDocument1 pageHepatitis B Immunization Health History FormBrady McGheeNo ratings yet
- Adolescent and Young Adult Use of Social Media For H - 2017 - Journal of AdolescDocument6 pagesAdolescent and Young Adult Use of Social Media For H - 2017 - Journal of AdolesctonytocamusicNo ratings yet
- Morbid Obesity - Anaesthetic Management: Prevalence and EpidemiologyDocument8 pagesMorbid Obesity - Anaesthetic Management: Prevalence and EpidemiologyLorena GarcíaNo ratings yet
- Housing Its Basic RequirementsDocument5 pagesHousing Its Basic RequirementsAkash Karwa100% (1)
- Book Mark Livre À La PageDocument1 pageBook Mark Livre À La PageAashish G. ShresthaNo ratings yet
- BASC-2 Q Global Score Summary SampleDocument11 pagesBASC-2 Q Global Score Summary SamplegenacartaNo ratings yet
- PMVDocument28 pagesPMVRajesh VermaNo ratings yet
- Hoffman GSDocument11 pagesHoffman GSaldo brataNo ratings yet
- Hse Business PlanDocument45 pagesHse Business PlanSalman AlNo ratings yet
- Reflection 4Document2 pagesReflection 4api-276689443No ratings yet
- Form 2D Health Plan Implementation Pregnancy Prenatal CareDocument2 pagesForm 2D Health Plan Implementation Pregnancy Prenatal CareLora CarpioNo ratings yet