Download as pdf or txt
You might also like
- Unit Plan ON Human Reproduction: Clinical Specality-I (Obstetric & Gynaecological Nursing-I)Document4 pagesUnit Plan ON Human Reproduction: Clinical Specality-I (Obstetric & Gynaecological Nursing-I)BHUKYA USHARANI100% (10)
- Wwiy4300 PDFDocument6 pagesWwiy4300 PDFvenkat ramanaNo ratings yet
- Cancer Epigenetics For Precision Medicine: Methods and ProtocolsDocument294 pagesCancer Epigenetics For Precision Medicine: Methods and Protocolsender000No ratings yet
- Miss. Anusha BanikDocument2 pagesMiss. Anusha BanikPrayani PohekarNo ratings yet
- PDF TextDocument2 pagesPDF TextchnmthakurNo ratings yet
- Imran - Itbs Hms HubDocument1 pageImran - Itbs Hms HubSarim HijaziNo ratings yet
- Master Anshu Jha 18 12 2023 05 29 03 PMDocument2 pagesMaster Anshu Jha 18 12 2023 05 29 03 PMVivek KumarNo ratings yet
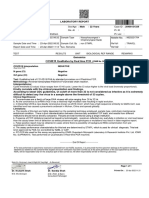
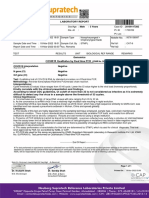
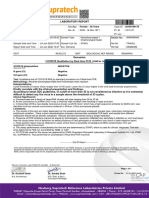
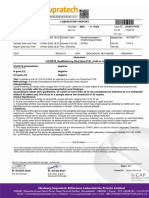
- COVID19 Qualitative by Real Time PCRDocument1 pageCOVID19 Qualitative by Real Time PCRAmritNo ratings yet
- Mr. Haan Kanuga 3 Years 20100117282: COVID19 Qualitative by Real Time PCRDocument1 pageMr. Haan Kanuga 3 Years 20100117282: COVID19 Qualitative by Real Time PCRIMOUNT ONENo ratings yet
- Report 2Document1 pageReport 2anshul shahNo ratings yet
- Covid Test Result Deepti PadteDocument2 pagesCovid Test Result Deepti PadteDeepti PadteNo ratings yet
- Report 3Document2 pagesReport 3kazimkureshiNo ratings yet
- Laboratory Report /:: Dis. At:::::: 31 Years 0122201673 Male Mr. Shakti Singh GaurDocument2 pagesLaboratory Report /:: Dis. At:::::: 31 Years 0122201673 Male Mr. Shakti Singh GaurShakti singh gaur100% (1)
- RASIKA S DIGHE-Female49 Yrs-6311Document11 pagesRASIKA S DIGHE-Female49 Yrs-6311UNIQUE DIAGNOSTICNo ratings yet
- TestReport 201103588Document1 pageTestReport 201103588vinayakraj jamreNo ratings yet
- MR Vaman Shantaram Shinde 07 06 2024 04 29 24 PMDocument1 pageMR Vaman Shantaram Shinde 07 06 2024 04 29 24 PMvivantadiagnosticNo ratings yet
- Ayushi SinghDocument2 pagesAyushi SinghAayushi SinghNo ratings yet
- Aakash Shantaram Bhingare-Male39 Yrs-6264Document11 pagesAakash Shantaram Bhingare-Male39 Yrs-6264UNIQUE DIAGNOSTICNo ratings yet
- COVID19 Qualitative by Real Time PCR: COVID19 Interpretation Positive N Gene (CT) 27 Orf Gene (CT) 24 Test: MethodologyDocument1 pageCOVID19 Qualitative by Real Time PCR: COVID19 Interpretation Positive N Gene (CT) 27 Orf Gene (CT) 24 Test: MethodologyNihar DaveNo ratings yet
- Report 2Document2 pagesReport 2vipultrivedi9049No ratings yet
- Laboratory Test Report: Mr. Shiva RatnakarDocument1 pageLaboratory Test Report: Mr. Shiva RatnakarRatnakar YeluripatiNo ratings yet
- Inik4750Document1 pageInik4750Ratnakar YeluripatiNo ratings yet
- Report 2402410522 1Document4 pagesReport 2402410522 1ahad siddiquiNo ratings yet
- Dharmila BhattDocument1 pageDharmila BhattytrdfghjjhgfdxcfghNo ratings yet
- Molecular Microbiology: Dr. Rania Ahmed Wagih AboushabanaDocument1 pageMolecular Microbiology: Dr. Rania Ahmed Wagih AboushabanaSP MusicNo ratings yet
- Enali FDocument1 pageEnali FIMOUNT ONENo ratings yet
- Mr. Jainil Patel 10 Years: COVID19 Qualitative by Real Time PCRDocument1 pageMr. Jainil Patel 10 Years: COVID19 Qualitative by Real Time PCRIMOUNT ONENo ratings yet
- Department of Molecular Virology: COVID-19 (Corona) VirusDocument1 pageDepartment of Molecular Virology: COVID-19 (Corona) VirusMuhammad YahyaNo ratings yet
- Ajit Vilas Borade0 - ReportDocument2 pagesAjit Vilas Borade0 - ReportRaj Singh RajputNo ratings yet
- Kavan FDocument1 pageKavan FIMOUNT ONENo ratings yet
- Your Test Result: ICMR Registration Number: COREG001Document3 pagesYour Test Result: ICMR Registration Number: COREG001BCom HonsNo ratings yet
- PdfText - 2024-03-21T204301.543Document1 pagePdfText - 2024-03-21T204301.543Ravindra “guddu” DongarwarNo ratings yet
- Pankajkumar FDocument1 pagePankajkumar FIMOUNT ONENo ratings yet
- JdhdhduDocument2 pagesJdhdhduAshish Singh NegiNo ratings yet
- Aj0291410ap31200089 RLSDocument4 pagesAj0291410ap31200089 RLSRooh KSHIVNo ratings yet
- Covid Test ResultDocument1 pageCovid Test ResultAshutosh SinghNo ratings yet
- PdfText - 2021-12-30T221208.263Document1 pagePdfText - 2021-12-30T221208.263Siva Kumar ReddyNo ratings yet
- Test Reports 2Document2 pagesTest Reports 2Chandrasekhara Reddy TNo ratings yet
- Sid No. 015836: Icmr Id 600784908Document1 pageSid No. 015836: Icmr Id 600784908Siva Kumar ReddyNo ratings yet
- Department of Laboratory Services - LaboratoryDocument1 pageDepartment of Laboratory Services - LaboratoryParchuri PraveenNo ratings yet
- Clinical BiochemistryDocument3 pagesClinical BiochemistrySatyam RajNo ratings yet
- Shweta Jain (42Y/F) Aarogyam C: Report For Tests AskedDocument14 pagesShweta Jain (42Y/F) Aarogyam C: Report For Tests Askednit2000_jainNo ratings yet
- COVID19 Qualitative by Real Time PCRDocument1 pageCOVID19 Qualitative by Real Time PCRNikhil JoseNo ratings yet
- Laboratory Test Report: Mr. D Venkata Narayna 39 Years MaleDocument2 pagesLaboratory Test Report: Mr. D Venkata Narayna 39 Years Malepavan kumarNo ratings yet
- Hyd 17 C 21127720331527Document26 pagesHyd 17 C 21127720331527brr21818No ratings yet
- CP-67, Viraj Khand, Gomti Nagar, Lucknow - 226 010: Name Ref. by Test Asked::: Patientid: Home CollectionDocument15 pagesCP-67, Viraj Khand, Gomti Nagar, Lucknow - 226 010: Name Ref. by Test Asked::: Patientid: Home CollectionArshad RizviNo ratings yet
- Special Chemistry: Test Name Current Result Previous Result Unit Normal RangeDocument1 pageSpecial Chemistry: Test Name Current Result Previous Result Unit Normal RangeSyed Muhammad Rafay AhmedNo ratings yet
- Output PDFDocument3 pagesOutput PDFTrunali GabhaneNo ratings yet
- Meera FDocument1 pageMeera FIMOUNT ONENo ratings yet
- Serology Report CH23260: Id NoDocument1 pageSerology Report CH23260: Id NoR RNo ratings yet
- Bhagat VilashchandraDocument1 pageBhagat VilashchandraSam Mak ShahNo ratings yet
- Shashi Kumar MDS FishDocument5 pagesShashi Kumar MDS FishVarun ChakravarthyNo ratings yet
- Nitn Jain (43Y/M) Aarogyam C: Report For Tests AskedDocument14 pagesNitn Jain (43Y/M) Aarogyam C: Report For Tests Askednit2000_jainNo ratings yet
- Fill, Byron Andaya 2396016328Document6 pagesFill, Byron Andaya 2396016328Dppr GeeksNo ratings yet
- COVID19 Qualitative by Real Time PCRDocument2 pagesCOVID19 Qualitative by Real Time PCRbrill khakhariyaNo ratings yet
- AllServices 6Document1 pageAllServices 6MohammedNo ratings yet
- Molecular Laboratory Report and CertificateDocument1 pageMolecular Laboratory Report and Certificateجوهوي ريسNo ratings yet
- S Shardaben Kalsaria Fem: Ale / 25 YearsDocument1 pageS Shardaben Kalsaria Fem: Ale / 25 YearsMonika MotiyaniNo ratings yet
- TestReport 2200200991Document1 pageTestReport 2200200991Harshvardhan KhatodNo ratings yet
- N S M C & H: Etaji Ubhas Edical Ollege OspitalDocument1 pageN S M C & H: Etaji Ubhas Edical Ollege OspitalChethan WizNo ratings yet
- A Revised Six-Kingdom System of LifeDocument64 pagesA Revised Six-Kingdom System of LifeleztlyNo ratings yet
- Biology Paper I - Botany Plant Water RelationsDocument4 pagesBiology Paper I - Botany Plant Water RelationsAnonymous X4QS89Um8wNo ratings yet
- Branches of MicrobiologyDocument2 pagesBranches of MicrobiologyMonika Sharma100% (2)
- Bio Exam ReviewerDocument10 pagesBio Exam ReviewerMarlon JonasNo ratings yet
- PLDH-L GB-D 21 001Document4 pagesPLDH-L GB-D 21 001Nita Sinta BelaNo ratings yet
- HW Proteins EnzymesDocument2 pagesHW Proteins Enzymesapi-524061079No ratings yet
- Session 7Document2 pagesSession 7KESHAVA MURTHY M VNo ratings yet
- Chemistry Project 1Document24 pagesChemistry Project 1mahidharNo ratings yet
- The Impact of Active and Passive Smoking Upon Health and Neurocognitive Function.Document4 pagesThe Impact of Active and Passive Smoking Upon Health and Neurocognitive Function.AmiraNo ratings yet
- Ujian Sains Tingkatan 2Document10 pagesUjian Sains Tingkatan 2SITI ZAIDAH AHMAD50% (6)
- 1 - Bio-2-Quarter 2 WalkthroughDocument50 pages1 - Bio-2-Quarter 2 WalkthroughJoyae ChavezNo ratings yet
- REFERAT - ToxicologieDocument21 pagesREFERAT - ToxicologieCotovici Catana AlinaNo ratings yet
- Sgu CompendiumDocument44 pagesSgu Compendiumdudeman2332No ratings yet
- Cross (2001) - Music, Cognition, Culture, and Evolution. Annals of The New York Academy of Sciences, 930 (1), 28-42 PDFDocument15 pagesCross (2001) - Music, Cognition, Culture, and Evolution. Annals of The New York Academy of Sciences, 930 (1), 28-42 PDFFederico WimanNo ratings yet
- E FaecalisDocument5 pagesE FaecalisMonica RoopChanderNo ratings yet
- Relationships Between Populations in The BiocoenosisDocument13 pagesRelationships Between Populations in The BiocoenosisSeptim SalvarusNo ratings yet
- Human Genetics BookDocument106 pagesHuman Genetics Bookharis100% (1)
- Imaging Protocol HandbookDocument90 pagesImaging Protocol HandbookAnita SzűcsNo ratings yet
- Secondary School Biology Short Notes and Exercises For Grade 9Document19 pagesSecondary School Biology Short Notes and Exercises For Grade 9Gashaw Fikir AdugnaNo ratings yet
- Program and Proceedings - 25th International "STRESS AND BEHAVIOR" Neuroscience and Biopsychiatry Conference, St-Petersburg, Russia (May 16-19, 2018)Document66 pagesProgram and Proceedings - 25th International "STRESS AND BEHAVIOR" Neuroscience and Biopsychiatry Conference, St-Petersburg, Russia (May 16-19, 2018)ISBS_SocietyNo ratings yet
- Case Report Primary Rosai-Dorfman Disease of Bone - A Report of Two CasesDocument7 pagesCase Report Primary Rosai-Dorfman Disease of Bone - A Report of Two CasesrexaNo ratings yet
- Prathamesh V. Kolekar Dept. Instrumentation Engg. Vishwakarma Institute of Technology, PuneDocument23 pagesPrathamesh V. Kolekar Dept. Instrumentation Engg. Vishwakarma Institute of Technology, PuneSajith KurianNo ratings yet
- Monthly 2 Test Form 4 (Bio)Document4 pagesMonthly 2 Test Form 4 (Bio)Manuel GakimNo ratings yet
- Embryology of The Genital TractDocument11 pagesEmbryology of The Genital TractAggiFitiyaningsihNo ratings yet
- Rate Limiting Step PDFDocument1 pageRate Limiting Step PDFCoy NuñezNo ratings yet
- Cho K1 (Atcc CCL 61) : Product SheetDocument2 pagesCho K1 (Atcc CCL 61) : Product Sheetawoiduahw asdoausjdNo ratings yet
- Single-Stranded Dna (Ssdna) Production in Dna Aptamer GenerationDocument9 pagesSingle-Stranded Dna (Ssdna) Production in Dna Aptamer Generationsubramaniyam.ek2821No ratings yet
- What's in A Cell - Worksheet & ColoringDocument2 pagesWhat's in A Cell - Worksheet & ColoringNuria Tarancon0% (1)