
Assessment of Peripheral Pulses RV - JB
Assessment of Peripheral Pulses RV - JB
You might also like
- Mini Practice Set 4 QuickBooks Guide PDFDocument4 pagesMini Practice Set 4 QuickBooks Guide PDFJoseph SalidoNo ratings yet
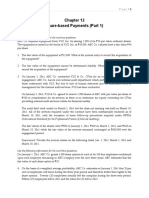
- Chapter 12 - Sh. Based Payments (Part 1)Document6 pagesChapter 12 - Sh. Based Payments (Part 1)Xiena100% (1)
- 18-Checklist For Cardiovascular AssessmentDocument2 pages18-Checklist For Cardiovascular Assessmentgladz25100% (3)
- 50 Nursing Mnemonics and Acronyms You Need To Know NowDocument29 pages50 Nursing Mnemonics and Acronyms You Need To Know Nowtandz100% (19)
- Web It CertDocument1 pageWeb It CertGuna SeelanNo ratings yet
- Cardiovascular AssessmentDocument73 pagesCardiovascular AssessmentmatthewsarfrazbhattiNo ratings yet
- Vital Signs: Temperature: Respiratory Rate: PulseDocument55 pagesVital Signs: Temperature: Respiratory Rate: PulsemiraNo ratings yet
- Cardiovascular Assessment (1) - StudentsDocument70 pagesCardiovascular Assessment (1) - Studentsraima ayazNo ratings yet
- 3&4&5-Assessment of Peripheral Vascular SystemDocument43 pages3&4&5-Assessment of Peripheral Vascular SystemKhaled Mohamed AssemNo ratings yet
- Respiratory Exam DetailedDocument12 pagesRespiratory Exam DetailedAshiniNo ratings yet
- USguidedprocedures EditedDocument7 pagesUSguidedprocedures EditedLex Alejandro Jr.No ratings yet
- CVS Exam (RCT)Document7 pagesCVS Exam (RCT)kenners100% (11)
- 102102234 NCM Checklist Vital SignsDocument18 pages102102234 NCM Checklist Vital SignsFranz Mireahna FeriaNo ratings yet
- Peripheral Arterial Occlusive DiseaseDocument4 pagesPeripheral Arterial Occlusive Diseasekrisfred14100% (1)
- Respiratory Asessment Inroduction: ProcedureDocument8 pagesRespiratory Asessment Inroduction: ProcedureSREEDEVI T SURESHNo ratings yet
- Cardiothoraxic and Vascular ExaminationDocument4 pagesCardiothoraxic and Vascular ExaminationPreetha PANo ratings yet
- NCBI BookshelfDocument9 pagesNCBI Bookshelframzan aliNo ratings yet
- Assessment of CvsDocument70 pagesAssessment of CvsTouseeq ManzoorNo ratings yet
- Respiratory Exam (RCT)Document8 pagesRespiratory Exam (RCT)kenners100% (31)
- Enfermedades Respiratorias, Cardiacas y Venosas de Los BovinosDocument37 pagesEnfermedades Respiratorias, Cardiacas y Venosas de Los BovinosDaniel MartinezNo ratings yet
- Makalah Bahasa InggrisDocument2 pagesMakalah Bahasa InggrisOlga RevalinaNo ratings yet
- Gambar Usg TestisDocument28 pagesGambar Usg TestisIrfan YHNo ratings yet
- Cardiovascular System: By: S@JDocument35 pagesCardiovascular System: By: S@JD TekNo ratings yet
- CardiovascularDocument7 pagesCardiovascularJerry MNo ratings yet
- VSD NotesDocument7 pagesVSD Noteshyamaemartinez101No ratings yet
- Cardiacassessmentppt 170323092148Document48 pagesCardiacassessmentppt 170323092148sasNo ratings yet
- 1-7 Levick and Dwight - CardiovascularDocument7 pages1-7 Levick and Dwight - Cardiovascularrahmawati aliwarmanNo ratings yet
- Abdominal Examination OSCE GuideDocument30 pagesAbdominal Examination OSCE Guideزياد سعيدNo ratings yet
- Semi CoaDocument19 pagesSemi Coa31 PASION, ROCHELLE C.No ratings yet
- Palpation: PBL CVS Week 2: Clinical Finding in Hypertension PatientDocument5 pagesPalpation: PBL CVS Week 2: Clinical Finding in Hypertension PatientHarina HorushiNo ratings yet
- Name: Werly Eka Saputri (21115060) Kartika Apriliyani (21115052)Document4 pagesName: Werly Eka Saputri (21115060) Kartika Apriliyani (21115052)Werly Eka LiaNo ratings yet
- Cardiac-Exam 08 July Article 9Document5 pagesCardiac-Exam 08 July Article 9AlexNo ratings yet
- Us Abdominal AortaDocument16 pagesUs Abdominal AortaRomaNo ratings yet
- Week 9 Laboratory Notes Part 1 StudentsDocument15 pagesWeek 9 Laboratory Notes Part 1 StudentsDaphne Cayaba BeltranNo ratings yet
- CVS OsceDocument19 pagesCVS OsceAbby LiewNo ratings yet
- Ankle-Brachial Index For Assessment of Peripheral Arterial DiseaseDocument3 pagesAnkle-Brachial Index For Assessment of Peripheral Arterial DiseaseKukuh Rizwido PrasetyoNo ratings yet
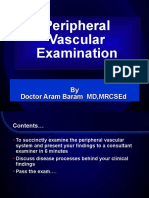
- Peripheral Vascular Examination: by Doctor Aram Baram MD, MrcsedDocument39 pagesPeripheral Vascular Examination: by Doctor Aram Baram MD, MrcsedMary Christine Estrada CabactulanNo ratings yet
- Peripheral Vascular Disease: Key Teaching PointsDocument9 pagesPeripheral Vascular Disease: Key Teaching PointsMayraPesantezCNo ratings yet
- ShafDocument4 pagesShafAulia CahyaniNo ratings yet
- Cardiovascular Dysfuntion Version 2Document10 pagesCardiovascular Dysfuntion Version 2Jhasseryne Orias SanchezNo ratings yet
- Diseases of Arteries - Arterial OcclusionDocument377 pagesDiseases of Arteries - Arterial OcclusionBhuvana MohanamurthyNo ratings yet
- Cardiovascular System, Questioning and Examination of Patients With Pathology of The Cardiovascular System.Document20 pagesCardiovascular System, Questioning and Examination of Patients With Pathology of The Cardiovascular System.ASAP teleNo ratings yet
- CardiovascularDocument1 pageCardiovascularshellstyneyenyenNo ratings yet
- 4 Respiratory ExaminationsDocument53 pages4 Respiratory Examinationscawsey mohamedNo ratings yet
- 1 Practise Questions Keith Moore 5th Edition Should ReadDocument113 pages1 Practise Questions Keith Moore 5th Edition Should ReadNasan Shehada100% (1)
- ElbowDocument7 pagesElbowapi-302398226No ratings yet
- Vital SignsDocument10 pagesVital SignsMuhammad FahmyNo ratings yet
- Cardiovascular Notes - Paediatrics ExaminationDocument5 pagesCardiovascular Notes - Paediatrics ExaminationPraveenNo ratings yet
- NCM Checklist - Vital SignsDocument18 pagesNCM Checklist - Vital SignsYanna Habib-Mangotara100% (1)
- Physiology Practical Measurement of Blood PressureDocument6 pagesPhysiology Practical Measurement of Blood PressureAli MohamedNo ratings yet
- CHAPTER 8 Neck AssestDocument61 pagesCHAPTER 8 Neck AssestLinlin Lindayani KusnandarNo ratings yet
- A P2 1Document36 pagesA P2 1Priya_Vankovic_7963No ratings yet
- Chest InjuryDocument6 pagesChest InjuryRolando Reyna100% (1)
- The Forearm, Wrist and HandDocument20 pagesThe Forearm, Wrist and HandKatalinNo ratings yet
- Cardiac CatheterizationDocument3 pagesCardiac CatheterizationAmir Ziad100% (1)
- PulseDocument13 pagesPulseArdi EroNo ratings yet
- Respiratory Examination: The Position of The PatientDocument24 pagesRespiratory Examination: The Position of The PatientMuhammed Barznji100% (1)
- University of Santo Tomas Faculty of Medicine & Surgery Department of Medicine Medicine 1 Cardiovascular Examination ChecklistDocument4 pagesUniversity of Santo Tomas Faculty of Medicine & Surgery Department of Medicine Medicine 1 Cardiovascular Examination ChecklistSocorro DuqueNo ratings yet
- Ankle-Brachial Index For Assessment of Peripheral Arterial DiseaseDocument5 pagesAnkle-Brachial Index For Assessment of Peripheral Arterial DiseaseindrawepeNo ratings yet
- Congenital Heart DefectDocument12 pagesCongenital Heart Defectsangkularosmina837No ratings yet
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- Mcdonalds Team Leader Performance Appraisal: Job Performance Evaluation FormDocument19 pagesMcdonalds Team Leader Performance Appraisal: Job Performance Evaluation FormBarbara GrahamNo ratings yet
- Anatomy Compre Exams 2004 2005Document7 pagesAnatomy Compre Exams 2004 2005GLeen Rose Onguda AguiLarNo ratings yet
- Blue and White Illustrative Technology Startup Pitch Deck Responsive PresentationDocument12 pagesBlue and White Illustrative Technology Startup Pitch Deck Responsive PresentationRajesh KumarNo ratings yet
- Ies, Iia and IpDocument46 pagesIes, Iia and IpRosalie E. BalhagNo ratings yet
- 7470 Msx36170switchDocument4 pages7470 Msx36170switchpeterNo ratings yet
- History of Labor LawDocument7 pagesHistory of Labor LawKalela HamimNo ratings yet
- 004 - Four Dimensions of Service ManagementDocument7 pages004 - Four Dimensions of Service ManagementAbdoo AbdooNo ratings yet
- Impact of COVID 19 in Islamic FinanceDocument76 pagesImpact of COVID 19 in Islamic FinanceTaraFKhaira100% (2)
- Plcement Hazel MascarenhasDocument2 pagesPlcement Hazel Mascarenhasapi-309903004No ratings yet
- Student Time Table For 5th To 10th June-2023: Room No. For OfflineDocument2 pagesStudent Time Table For 5th To 10th June-2023: Room No. For OfflineNaitik AdityaNo ratings yet
- Apc-4500ve Seccion 8.1. Profit Controller. Referencia de InstalacionDocument137 pagesApc-4500ve Seccion 8.1. Profit Controller. Referencia de InstalacionNorberto PeñaNo ratings yet
- Jaipuria Institute of Management 1. Course Information MKT402 Marketing Planning and Control 3Document17 pagesJaipuria Institute of Management 1. Course Information MKT402 Marketing Planning and Control 3Sanjeev Kumar Suman Student, Jaipuria LucknowNo ratings yet
- Customer Perception Towards Various DTH Service ProvidersDocument19 pagesCustomer Perception Towards Various DTH Service ProvidersShiva RajetiNo ratings yet
- Hepatology MRCP1Document87 pagesHepatology MRCP1Raouf Ra'fat SolimanNo ratings yet
- Secure Remote AccessDocument7 pagesSecure Remote Accessnupoor naikNo ratings yet
- Primary Sources of ShariahDocument15 pagesPrimary Sources of ShariahAeina FaiiziNo ratings yet
- Activity Week 14 PROJECT 2-9ºDocument3 pagesActivity Week 14 PROJECT 2-9ºTheSeul SNo ratings yet
- VarmaDocument86 pagesVarmanandy39No ratings yet
- 7DSM21019 - 22003 - PPH Building No 7 - 02Document5 pages7DSM21019 - 22003 - PPH Building No 7 - 02FARHANAH AFIQAH RAZMANNo ratings yet
- Water PumpsDocument4 pagesWater PumpsEphremHailuNo ratings yet
- Module2 CWTS 2ndsemDocument4 pagesModule2 CWTS 2ndsemryujinNo ratings yet
- Jacob Dean Curtis Instacart: Consumer Report For Requestor Company StatusDocument6 pagesJacob Dean Curtis Instacart: Consumer Report For Requestor Company StatusJAKE CURTISNo ratings yet
- J OperatorDocument6 pagesJ OperatorManikandan SundararajNo ratings yet
- Major Resource Projects: Western Australia - 2021Document1 pageMajor Resource Projects: Western Australia - 2021royalNo ratings yet
- Fifth SunDocument337 pagesFifth Sundhana sekaran100% (6)
- 1 Introduction To Real Estate Market in DubaiDocument6 pages1 Introduction To Real Estate Market in DubaiAbdul Raqeeb AbidNo ratings yet
- ISTQB Dumps and Mock Tests For Foundation Level Paper 9Document5 pagesISTQB Dumps and Mock Tests For Foundation Level Paper 9Lília Diana Nascimento100% (1)






















































































Download as docx, pdf, or txt
You might also like
- Mini Practice Set 4 QuickBooks Guide PDFDocument4 pagesMini Practice Set 4 QuickBooks Guide PDFJoseph SalidoNo ratings yet
- Chapter 12 - Sh. Based Payments (Part 1)Document6 pagesChapter 12 - Sh. Based Payments (Part 1)Xiena100% (1)
- 18-Checklist For Cardiovascular AssessmentDocument2 pages18-Checklist For Cardiovascular Assessmentgladz25100% (3)
- 50 Nursing Mnemonics and Acronyms You Need To Know NowDocument29 pages50 Nursing Mnemonics and Acronyms You Need To Know Nowtandz100% (19)
- Web It CertDocument1 pageWeb It CertGuna SeelanNo ratings yet
- Cardiovascular AssessmentDocument73 pagesCardiovascular AssessmentmatthewsarfrazbhattiNo ratings yet
- Vital Signs: Temperature: Respiratory Rate: PulseDocument55 pagesVital Signs: Temperature: Respiratory Rate: PulsemiraNo ratings yet
- Cardiovascular Assessment (1) - StudentsDocument70 pagesCardiovascular Assessment (1) - Studentsraima ayazNo ratings yet
- 3&4&5-Assessment of Peripheral Vascular SystemDocument43 pages3&4&5-Assessment of Peripheral Vascular SystemKhaled Mohamed AssemNo ratings yet
- Respiratory Exam DetailedDocument12 pagesRespiratory Exam DetailedAshiniNo ratings yet
- USguidedprocedures EditedDocument7 pagesUSguidedprocedures EditedLex Alejandro Jr.No ratings yet
- CVS Exam (RCT)Document7 pagesCVS Exam (RCT)kenners100% (11)
- 102102234 NCM Checklist Vital SignsDocument18 pages102102234 NCM Checklist Vital SignsFranz Mireahna FeriaNo ratings yet
- Peripheral Arterial Occlusive DiseaseDocument4 pagesPeripheral Arterial Occlusive Diseasekrisfred14100% (1)
- Respiratory Asessment Inroduction: ProcedureDocument8 pagesRespiratory Asessment Inroduction: ProcedureSREEDEVI T SURESHNo ratings yet
- Cardiothoraxic and Vascular ExaminationDocument4 pagesCardiothoraxic and Vascular ExaminationPreetha PANo ratings yet
- NCBI BookshelfDocument9 pagesNCBI Bookshelframzan aliNo ratings yet
- Assessment of CvsDocument70 pagesAssessment of CvsTouseeq ManzoorNo ratings yet
- Respiratory Exam (RCT)Document8 pagesRespiratory Exam (RCT)kenners100% (31)
- Enfermedades Respiratorias, Cardiacas y Venosas de Los BovinosDocument37 pagesEnfermedades Respiratorias, Cardiacas y Venosas de Los BovinosDaniel MartinezNo ratings yet
- Makalah Bahasa InggrisDocument2 pagesMakalah Bahasa InggrisOlga RevalinaNo ratings yet
- Gambar Usg TestisDocument28 pagesGambar Usg TestisIrfan YHNo ratings yet
- Cardiovascular System: By: S@JDocument35 pagesCardiovascular System: By: S@JD TekNo ratings yet
- CardiovascularDocument7 pagesCardiovascularJerry MNo ratings yet
- VSD NotesDocument7 pagesVSD Noteshyamaemartinez101No ratings yet
- Cardiacassessmentppt 170323092148Document48 pagesCardiacassessmentppt 170323092148sasNo ratings yet
- 1-7 Levick and Dwight - CardiovascularDocument7 pages1-7 Levick and Dwight - Cardiovascularrahmawati aliwarmanNo ratings yet
- Abdominal Examination OSCE GuideDocument30 pagesAbdominal Examination OSCE Guideزياد سعيدNo ratings yet
- Semi CoaDocument19 pagesSemi Coa31 PASION, ROCHELLE C.No ratings yet
- Palpation: PBL CVS Week 2: Clinical Finding in Hypertension PatientDocument5 pagesPalpation: PBL CVS Week 2: Clinical Finding in Hypertension PatientHarina HorushiNo ratings yet
- Name: Werly Eka Saputri (21115060) Kartika Apriliyani (21115052)Document4 pagesName: Werly Eka Saputri (21115060) Kartika Apriliyani (21115052)Werly Eka LiaNo ratings yet
- Cardiac-Exam 08 July Article 9Document5 pagesCardiac-Exam 08 July Article 9AlexNo ratings yet
- Us Abdominal AortaDocument16 pagesUs Abdominal AortaRomaNo ratings yet
- Week 9 Laboratory Notes Part 1 StudentsDocument15 pagesWeek 9 Laboratory Notes Part 1 StudentsDaphne Cayaba BeltranNo ratings yet
- CVS OsceDocument19 pagesCVS OsceAbby LiewNo ratings yet
- Ankle-Brachial Index For Assessment of Peripheral Arterial DiseaseDocument3 pagesAnkle-Brachial Index For Assessment of Peripheral Arterial DiseaseKukuh Rizwido PrasetyoNo ratings yet
- Peripheral Vascular Examination: by Doctor Aram Baram MD, MrcsedDocument39 pagesPeripheral Vascular Examination: by Doctor Aram Baram MD, MrcsedMary Christine Estrada CabactulanNo ratings yet
- Peripheral Vascular Disease: Key Teaching PointsDocument9 pagesPeripheral Vascular Disease: Key Teaching PointsMayraPesantezCNo ratings yet
- ShafDocument4 pagesShafAulia CahyaniNo ratings yet
- Cardiovascular Dysfuntion Version 2Document10 pagesCardiovascular Dysfuntion Version 2Jhasseryne Orias SanchezNo ratings yet
- Diseases of Arteries - Arterial OcclusionDocument377 pagesDiseases of Arteries - Arterial OcclusionBhuvana MohanamurthyNo ratings yet
- Cardiovascular System, Questioning and Examination of Patients With Pathology of The Cardiovascular System.Document20 pagesCardiovascular System, Questioning and Examination of Patients With Pathology of The Cardiovascular System.ASAP teleNo ratings yet
- CardiovascularDocument1 pageCardiovascularshellstyneyenyenNo ratings yet
- 4 Respiratory ExaminationsDocument53 pages4 Respiratory Examinationscawsey mohamedNo ratings yet
- 1 Practise Questions Keith Moore 5th Edition Should ReadDocument113 pages1 Practise Questions Keith Moore 5th Edition Should ReadNasan Shehada100% (1)
- ElbowDocument7 pagesElbowapi-302398226No ratings yet
- Vital SignsDocument10 pagesVital SignsMuhammad FahmyNo ratings yet
- Cardiovascular Notes - Paediatrics ExaminationDocument5 pagesCardiovascular Notes - Paediatrics ExaminationPraveenNo ratings yet
- NCM Checklist - Vital SignsDocument18 pagesNCM Checklist - Vital SignsYanna Habib-Mangotara100% (1)
- Physiology Practical Measurement of Blood PressureDocument6 pagesPhysiology Practical Measurement of Blood PressureAli MohamedNo ratings yet
- CHAPTER 8 Neck AssestDocument61 pagesCHAPTER 8 Neck AssestLinlin Lindayani KusnandarNo ratings yet
- A P2 1Document36 pagesA P2 1Priya_Vankovic_7963No ratings yet
- Chest InjuryDocument6 pagesChest InjuryRolando Reyna100% (1)
- The Forearm, Wrist and HandDocument20 pagesThe Forearm, Wrist and HandKatalinNo ratings yet
- Cardiac CatheterizationDocument3 pagesCardiac CatheterizationAmir Ziad100% (1)
- PulseDocument13 pagesPulseArdi EroNo ratings yet
- Respiratory Examination: The Position of The PatientDocument24 pagesRespiratory Examination: The Position of The PatientMuhammed Barznji100% (1)
- University of Santo Tomas Faculty of Medicine & Surgery Department of Medicine Medicine 1 Cardiovascular Examination ChecklistDocument4 pagesUniversity of Santo Tomas Faculty of Medicine & Surgery Department of Medicine Medicine 1 Cardiovascular Examination ChecklistSocorro DuqueNo ratings yet
- Ankle-Brachial Index For Assessment of Peripheral Arterial DiseaseDocument5 pagesAnkle-Brachial Index For Assessment of Peripheral Arterial DiseaseindrawepeNo ratings yet
- Congenital Heart DefectDocument12 pagesCongenital Heart Defectsangkularosmina837No ratings yet
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- Mcdonalds Team Leader Performance Appraisal: Job Performance Evaluation FormDocument19 pagesMcdonalds Team Leader Performance Appraisal: Job Performance Evaluation FormBarbara GrahamNo ratings yet
- Anatomy Compre Exams 2004 2005Document7 pagesAnatomy Compre Exams 2004 2005GLeen Rose Onguda AguiLarNo ratings yet
- Blue and White Illustrative Technology Startup Pitch Deck Responsive PresentationDocument12 pagesBlue and White Illustrative Technology Startup Pitch Deck Responsive PresentationRajesh KumarNo ratings yet
- Ies, Iia and IpDocument46 pagesIes, Iia and IpRosalie E. BalhagNo ratings yet
- 7470 Msx36170switchDocument4 pages7470 Msx36170switchpeterNo ratings yet
- History of Labor LawDocument7 pagesHistory of Labor LawKalela HamimNo ratings yet
- 004 - Four Dimensions of Service ManagementDocument7 pages004 - Four Dimensions of Service ManagementAbdoo AbdooNo ratings yet
- Impact of COVID 19 in Islamic FinanceDocument76 pagesImpact of COVID 19 in Islamic FinanceTaraFKhaira100% (2)
- Plcement Hazel MascarenhasDocument2 pagesPlcement Hazel Mascarenhasapi-309903004No ratings yet
- Student Time Table For 5th To 10th June-2023: Room No. For OfflineDocument2 pagesStudent Time Table For 5th To 10th June-2023: Room No. For OfflineNaitik AdityaNo ratings yet
- Apc-4500ve Seccion 8.1. Profit Controller. Referencia de InstalacionDocument137 pagesApc-4500ve Seccion 8.1. Profit Controller. Referencia de InstalacionNorberto PeñaNo ratings yet
- Jaipuria Institute of Management 1. Course Information MKT402 Marketing Planning and Control 3Document17 pagesJaipuria Institute of Management 1. Course Information MKT402 Marketing Planning and Control 3Sanjeev Kumar Suman Student, Jaipuria LucknowNo ratings yet
- Customer Perception Towards Various DTH Service ProvidersDocument19 pagesCustomer Perception Towards Various DTH Service ProvidersShiva RajetiNo ratings yet
- Hepatology MRCP1Document87 pagesHepatology MRCP1Raouf Ra'fat SolimanNo ratings yet
- Secure Remote AccessDocument7 pagesSecure Remote Accessnupoor naikNo ratings yet
- Primary Sources of ShariahDocument15 pagesPrimary Sources of ShariahAeina FaiiziNo ratings yet
- Activity Week 14 PROJECT 2-9ºDocument3 pagesActivity Week 14 PROJECT 2-9ºTheSeul SNo ratings yet
- VarmaDocument86 pagesVarmanandy39No ratings yet
- 7DSM21019 - 22003 - PPH Building No 7 - 02Document5 pages7DSM21019 - 22003 - PPH Building No 7 - 02FARHANAH AFIQAH RAZMANNo ratings yet
- Water PumpsDocument4 pagesWater PumpsEphremHailuNo ratings yet
- Module2 CWTS 2ndsemDocument4 pagesModule2 CWTS 2ndsemryujinNo ratings yet
- Jacob Dean Curtis Instacart: Consumer Report For Requestor Company StatusDocument6 pagesJacob Dean Curtis Instacart: Consumer Report For Requestor Company StatusJAKE CURTISNo ratings yet
- J OperatorDocument6 pagesJ OperatorManikandan SundararajNo ratings yet
- Major Resource Projects: Western Australia - 2021Document1 pageMajor Resource Projects: Western Australia - 2021royalNo ratings yet
- Fifth SunDocument337 pagesFifth Sundhana sekaran100% (6)
- 1 Introduction To Real Estate Market in DubaiDocument6 pages1 Introduction To Real Estate Market in DubaiAbdul Raqeeb AbidNo ratings yet
- ISTQB Dumps and Mock Tests For Foundation Level Paper 9Document5 pagesISTQB Dumps and Mock Tests For Foundation Level Paper 9Lília Diana Nascimento100% (1)