Download as pdf or txt
You might also like
- New Patient FormDocument8 pagesNew Patient Forme-MedTools100% (5)
- Initial Case History FormDocument3 pagesInitial Case History Formapi-245579214No ratings yet
- Adolescent Biopsychosocial AssessmentDocument10 pagesAdolescent Biopsychosocial AssessmentFar Sultan100% (2)
- Aphasia Adult Evaluation FormDocument7 pagesAphasia Adult Evaluation FormUju IwujiNo ratings yet
- Draft QuestionsDocument2 pagesDraft QuestionsYvetteNavarroNo ratings yet
- Intake DocumentsDocument5 pagesIntake Documentsapi-458840312No ratings yet
- Onfidential Data Form: T L O S CDocument8 pagesOnfidential Data Form: T L O S Cnatpal100% (1)
- Client Intake Form: (Last) (First) (MI)Document20 pagesClient Intake Form: (Last) (First) (MI)Prabha Gupta0% (1)
- Appletree NP Forms FillableDocument2 pagesAppletree NP Forms FillableFabian SvrNo ratings yet
- AD Guide Entire Checklist v4Document37 pagesAD Guide Entire Checklist v4FAKESIGNUPACCOUNTNo ratings yet
- Job Application FormDocument3 pagesJob Application Formsupri0% (1)
- Ateneo de Zamboanga Som - ApplicationDocument5 pagesAteneo de Zamboanga Som - ApplicationKai BenlotNo ratings yet
- Brown Hearing Centers: Personal InformationDocument2 pagesBrown Hearing Centers: Personal InformationEddie TooheyNo ratings yet
- Client BiodataDocument1 pageClient BiodataDS Nan SalimNo ratings yet
- Application Form: FSL, 18 Waldstock Road, London, SE28 8SF Section 1Document5 pagesApplication Form: FSL, 18 Waldstock Road, London, SE28 8SF Section 1Niaz KhanNo ratings yet
- FEBC Info Sheet - NEWDocument5 pagesFEBC Info Sheet - NEWnigel alinsug0% (1)
- MTI - Wifey AppDocument5 pagesMTI - Wifey AppShandon Campbell100% (1)
- Leetaloo Pediatric Therapy: General InformationDocument7 pagesLeetaloo Pediatric Therapy: General InformationrabiyaNo ratings yet
- College Individual Inventory SheetDocument2 pagesCollege Individual Inventory SheetjonaxxisthequeenNo ratings yet
- CSDD-O-2114 ANNEXES Counseling and References - 12162020Document14 pagesCSDD-O-2114 ANNEXES Counseling and References - 12162020Steff Musni-QuiballoNo ratings yet
- Main - Girlfriend Application FormDocument4 pagesMain - Girlfriend Application FormariezcathydNo ratings yet
- New Patient Paperwork WebsiteDocument4 pagesNew Patient Paperwork WebsiteAnonymous P43hpCNo ratings yet
- Employment Application FormDocument6 pagesEmployment Application FormAMYSOPHIANI BINTI ADENI MoeNo ratings yet
- Msa PsychDocument6 pagesMsa PsychpauleneNo ratings yet
- Foster ApplicationDocument6 pagesFoster ApplicationHerb100% (5)
- DENR Health Survey Form and Contact Person Form Page 2Document2 pagesDENR Health Survey Form and Contact Person Form Page 2Mary Jane BarrientosNo ratings yet
- Intake Form 2020 PDFDocument2 pagesIntake Form 2020 PDFShanjni malaNo ratings yet
- Suicide Risk Asst ToolDocument3 pagesSuicide Risk Asst ToolkasmiantoabadiNo ratings yet
- AKB Childcare-Worker-Application FormDocument7 pagesAKB Childcare-Worker-Application FormgiftnyahungaNo ratings yet
- MWCH Card2Document4 pagesMWCH Card2nikkaNo ratings yet
- Personal Inventory Form Informatics Version 2Document3 pagesPersonal Inventory Form Informatics Version 2charles199326No ratings yet
- Demographic QuestionsDocument6 pagesDemographic QuestionsCynthia Ann Stephanie SapladNo ratings yet
- Student Information FormDocument2 pagesStudent Information FormcandacerobinetteNo ratings yet
- God Is Not Dead Tour ApplicationDocument5 pagesGod Is Not Dead Tour Applicationteresa_agreNo ratings yet
- Nursing Health Assessment Guide: San Pedro CollegeDocument3 pagesNursing Health Assessment Guide: San Pedro CollegeRue Cheng MaNo ratings yet
- Nursing Health Assessment Guide: San Pedro CollegeDocument3 pagesNursing Health Assessment Guide: San Pedro CollegeKim ZNo ratings yet
- Dating ApplicationDocument4 pagesDating Applicationlord_PruittNo ratings yet
- Individual Inventory ReportDocument2 pagesIndividual Inventory ReportGabriel Ramos100% (1)
- Nursing Care Health Assessment FormDocument5 pagesNursing Care Health Assessment FormMelanie Bagasol SisonNo ratings yet
- Dental History: Personal InformationDocument6 pagesDental History: Personal InformationSharaz AhmedNo ratings yet
- Health Statement FormDocument1 pageHealth Statement FormALT IkedaNo ratings yet
- Aesthetic Clinic FileDocument11 pagesAesthetic Clinic FileScribdTranslationsNo ratings yet
- Friend RefDocument2 pagesFriend RefNathan ChaceNo ratings yet
- AppForm 11111HSDocument6 pagesAppForm 11111HSvainly4u8155No ratings yet
- Report Format-1Document9 pagesReport Format-1Hira JavedNo ratings yet
- Laboratory Request Form Laboratory Request FormDocument1 pageLaboratory Request Form Laboratory Request FormAina Haravata0% (1)
- Children's Audiological HistoryDocument7 pagesChildren's Audiological HistoryScribdTranslationsNo ratings yet
- Prospective Client Interview 0967Document1 pageProspective Client Interview 0967Henry Jacob Baker JrNo ratings yet
- Nursing Care Health Assessment Form: Instructions For CompletionDocument6 pagesNursing Care Health Assessment Form: Instructions For CompletionJM RomiasNo ratings yet
- Adult Case History Form2Document6 pagesAdult Case History Form2Josè Miguel Amador SantibañezNo ratings yet
- Doctor FormsDocument3 pagesDoctor Formsmirnoori35No ratings yet
- ApplicationDocument3 pagesApplicationapi-386103732No ratings yet
- Child or Adolescent Client FormsDocument7 pagesChild or Adolescent Client FormsSodfa EttafakshiNo ratings yet
- Franchise Application Form 2021Document8 pagesFranchise Application Form 2021Jean Lois Condeza GelmoNo ratings yet
- Employee Information Sheet: Joining ReportDocument9 pagesEmployee Information Sheet: Joining ReportumamaheswarantmNo ratings yet
- SOM Application FormDocument5 pagesSOM Application FormMark MejiaNo ratings yet
- Attachment P.EDocument2 pagesAttachment P.EMichelle Wendy Y. VenturaNo ratings yet
- CN TablesDocument4 pagesCN TablesAnne Clarisse DionisioNo ratings yet
- 386-Article Text-1343-1-10-20221102Document12 pages386-Article Text-1343-1-10-20221102Anne Clarisse DionisioNo ratings yet
- Pricing EquipmentDocument31 pagesPricing EquipmentAnne Clarisse DionisioNo ratings yet
- Runoff EstimatesDocument152 pagesRunoff EstimatesAnne Clarisse DionisioNo ratings yet
- Earthquake Engineering124Document5 pagesEarthquake Engineering124Anne Clarisse DionisioNo ratings yet
- Unified Application Form For Building PermitDocument2 pagesUnified Application Form For Building PermitAnne Clarisse DionisioNo ratings yet
- Civil Structural Permit Front and BackDocument2 pagesCivil Structural Permit Front and BackAnne Clarisse DionisioNo ratings yet
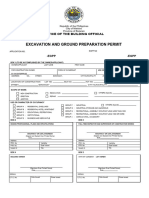
- Excavation Permit Front and BackDocument2 pagesExcavation Permit Front and BackAnne Clarisse DionisioNo ratings yet
- CVE 311 Earthquake Engineering Module Part 4Document40 pagesCVE 311 Earthquake Engineering Module Part 4Anne Clarisse DionisioNo ratings yet
- CVE 311 Earthquake Engineering Module Part 2Document25 pagesCVE 311 Earthquake Engineering Module Part 2Anne Clarisse DionisioNo ratings yet
- Chapter I PPT Engineering Management Lesson 1.1 1.2Document19 pagesChapter I PPT Engineering Management Lesson 1.1 1.2Anne Clarisse DionisioNo ratings yet
- Construction Materials and Testing. 01. Introduction (Part 1)Document38 pagesConstruction Materials and Testing. 01. Introduction (Part 1)Anne Clarisse DionisioNo ratings yet
- CIR Vs Toshiba Information Equipment (Phils) IncDocument12 pagesCIR Vs Toshiba Information Equipment (Phils) Incsamaral bentesinkoNo ratings yet
- SVP 2006 Annual ReportDocument18 pagesSVP 2006 Annual ReportRobert LedermanNo ratings yet
- 2 The Philippines in The 19th CenturyDocument12 pages2 The Philippines in The 19th Centuryisaiah menesesNo ratings yet
- Abusive Behavior InventoryDocument3 pagesAbusive Behavior InventorySebestyén ErikaNo ratings yet
- Employment Law AssignmentDocument37 pagesEmployment Law AssignmentSahanNivantha0% (1)
- Worksheet RizalDocument3 pagesWorksheet RizalIce CreemiNo ratings yet
- Checklists Duke TurbineDocument11 pagesChecklists Duke Turbinejuan marchiNo ratings yet
- Module 2. Analysis of Historical Events Primary and Secondary SourcesDocument24 pagesModule 2. Analysis of Historical Events Primary and Secondary SourcesJinecy Docilidad100% (1)
- Bedford Flag UnfurledDocument116 pagesBedford Flag UnfurledHal ShurtleffNo ratings yet
- Araling Panlipunan: Quarter 4 - Module 3Document18 pagesAraling Panlipunan: Quarter 4 - Module 3nabila macaraob75% (8)
- PD 953 - Requiring Planting of Tree in Certain PlacesDocument3 pagesPD 953 - Requiring Planting of Tree in Certain PlacesJomerNo ratings yet
- The Multi-Layered CitizenDocument20 pagesThe Multi-Layered CitizenJudalineNo ratings yet
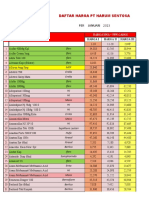
- HARGAHARSENJAN23Document48 pagesHARGAHARSENJAN23apotek telagasariNo ratings yet
- Important Information About Brian and Michelle and Evidence For GirlsDocument6 pagesImportant Information About Brian and Michelle and Evidence For GirlssistermarylisaNo ratings yet
- Denver Police Department ManualDocument807 pagesDenver Police Department ManualEthan IseNo ratings yet
- Government To Stop Divisive' Town Hall Boycotts & SanctionsDocument4 pagesGovernment To Stop Divisive' Town Hall Boycotts & SanctionsCBakerNo ratings yet
- 2022 Asylum Report ENDocument385 pages2022 Asylum Report ENpaulapimentamnNo ratings yet
- Initial Contact and Asylum Registration QuestionnaireDocument16 pagesInitial Contact and Asylum Registration QuestionnaireFerdows QasimeNo ratings yet
- 1892, Rizal Organized The La Liga Filipina, This: Confronting Colonialism: Katipunan and The Revolution of 1896Document13 pages1892, Rizal Organized The La Liga Filipina, This: Confronting Colonialism: Katipunan and The Revolution of 1896Julie Ann Barsalote GubaNo ratings yet
- Project On MahabhartaDocument10 pagesProject On Mahabhartaimpraveen4u100% (1)
- People V Quiaoit Jr. GR No. 175222Document2 pagesPeople V Quiaoit Jr. GR No. 175222Duko Alcala EnjambreNo ratings yet
- 2023-09-28 St. Mary's County TimesDocument40 pages2023-09-28 St. Mary's County TimesSouthern Maryland OnlineNo ratings yet
- United States of America v. Matt CalicchioDocument4 pagesUnited States of America v. Matt CalicchioMile Square ViewNo ratings yet
- Frontier LimitationsDocument5 pagesFrontier LimitationsdenicotienoNo ratings yet
- Docena v. LapesuraDocument1 pageDocena v. LapesuraJam ZaldivarNo ratings yet
- Hoover Digest, 2018, No. 4, FallDocument212 pagesHoover Digest, 2018, No. 4, FallHoover Institution100% (3)
- Doj Rey ReviewDocument28 pagesDoj Rey ReviewOly VerNo ratings yet
- Almario v. Alba, GR No. L-66068Document2 pagesAlmario v. Alba, GR No. L-66068Gab EstiadaNo ratings yet
- Reguland Irreg VerbsDocument5 pagesReguland Irreg VerbsJose Victor Loayza AcostaNo ratings yet
- Devolution of Power in PakistanDocument4 pagesDevolution of Power in PakistanZeeshan BalochNo ratings yet