Download as pdf or txt
You might also like
- Pharmacology of OxaliplatinDocument16 pagesPharmacology of OxaliplatinAliza JafriNo ratings yet
- Review Article: Cellular Responses To Cisplatin-Induced DNA DamageDocument17 pagesReview Article: Cellular Responses To Cisplatin-Induced DNA DamageBilal TahirNo ratings yet
- Cisplatin Nephrotoxicity PDFDocument10 pagesCisplatin Nephrotoxicity PDFChaa CiieCuiitt AfrNo ratings yet
- Calcineurin Inhibitors and Sirolimus - Mechanisms of Action and Applications in DermatologyDocument7 pagesCalcineurin Inhibitors and Sirolimus - Mechanisms of Action and Applications in Dermatology陈梓强No ratings yet
- Zeolite StudyDocument4 pagesZeolite StudyAdeel AhmedNo ratings yet
- The Synergistic Effects of Oxaliplatin and Piperlongumine On Colorectal Cancer Are Mediated by Oxidative StressDocument12 pagesThe Synergistic Effects of Oxaliplatin and Piperlongumine On Colorectal Cancer Are Mediated by Oxidative StressRAJAN KUMARNo ratings yet
- Porte Tal 18Document18 pagesPorte Tal 18alfredoibcNo ratings yet
- Anti Neoplastic AgentsDocument23 pagesAnti Neoplastic AgentsHawkar QadirNo ratings yet
- Curcumin Pyrazole and Its Derivative N-3-NitrophenDocument16 pagesCurcumin Pyrazole and Its Derivative N-3-NitrophenjuanesglvzNo ratings yet
- Cisplatin Cause NephrotoxicityDocument11 pagesCisplatin Cause NephrotoxicityZiRong TsengNo ratings yet
- Jordan 2000Document7 pagesJordan 2000Thomas RobinsonNo ratings yet
- Raon 53 148Document11 pagesRaon 53 148Heru SigitNo ratings yet
- LeptocarpinaDocument7 pagesLeptocarpinaJ Nicolas MJNo ratings yet
- Acschemneuro 5b00134 PDFDocument10 pagesAcschemneuro 5b00134 PDFAnonymous Bh6y0TuVHiNo ratings yet
- Antineoplastic AgentsDocument10 pagesAntineoplastic AgentsMuhamed ArsalanNo ratings yet
- Recent Findings On The Mechanism of Cisplatin-Induced Renal Cytotoxicity and Therapeutic Potential of Natural CompoundsDocument22 pagesRecent Findings On The Mechanism of Cisplatin-Induced Renal Cytotoxicity and Therapeutic Potential of Natural CompoundsSamantha AdrianneNo ratings yet
- Donkor 2000Document18 pagesDonkor 2000Marli CorreaNo ratings yet
- Alkylating Agents and Related DrugsDocument35 pagesAlkylating Agents and Related Drugsgrace caasiNo ratings yet
- Use of CisplatinDocument14 pagesUse of CisplatinsmijatovicibissNo ratings yet
- Cisplatin As An Anti Cancer DrugDocument10 pagesCisplatin As An Anti Cancer DrugMahima KamraNo ratings yet
- CisplatinDocument15 pagesCisplatinBrantas Pra AzariNo ratings yet
- Muhammad Ali ArticlesDocument87 pagesMuhammad Ali ArticlesMuhammad AliAliNo ratings yet
- Abstracts Free Radical Biology and Medicine 165 (2021) 26 - 59Document1 pageAbstracts Free Radical Biology and Medicine 165 (2021) 26 - 59Irina ASNo ratings yet
- C Jeffery Tig 2003Document3 pagesC Jeffery Tig 2003Camila EscobarNo ratings yet
- Role of Nadph:Cytochrome C Reducã-Aseand Dt-Diaphorase in The Biotransformation of Mitomycin C1Document7 pagesRole of Nadph:Cytochrome C Reducã-Aseand Dt-Diaphorase in The Biotransformation of Mitomycin C1Krys tallNo ratings yet
- Curr Med Chem 16182235-22602009Document26 pagesCurr Med Chem 16182235-22602009ZozoNo ratings yet
- Antitumour Activity On Extrinsic ApoptotDocument11 pagesAntitumour Activity On Extrinsic ApoptotLeoncio LucenaNo ratings yet
- Anticancer Drugs Med ChemDocument215 pagesAnticancer Drugs Med ChemCurex QANo ratings yet
- Lipoplatin Formulation Review ArticleDocument11 pagesLipoplatin Formulation Review Articleandi hasri ainunNo ratings yet
- 603e721daa4d993c974fc941 Potential Risk of Cationic Lipid in The Pfizer-BioNTech VaccineDocument3 pages603e721daa4d993c974fc941 Potential Risk of Cationic Lipid in The Pfizer-BioNTech VaccineBruno MNo ratings yet
- Necrosis (A Programmed Cell Death) : Presented By: Nisarg (11097) Bhumika (11157) Ashish (11135)Document16 pagesNecrosis (A Programmed Cell Death) : Presented By: Nisarg (11097) Bhumika (11157) Ashish (11135)Ashish EzhuvaNo ratings yet
- ACSChemBiol 2011 6 234 PDFDocument18 pagesACSChemBiol 2011 6 234 PDFDavid BorhaniNo ratings yet
- Austin Journal of Analytical and Pharmaceutical ChemistryDocument6 pagesAustin Journal of Analytical and Pharmaceutical ChemistryAustin Publishing GroupNo ratings yet
- Tugas EPDocument20 pagesTugas EPkartikachandraaNo ratings yet
- CMCDocument32 pagesCMCMonalisa BritoNo ratings yet
- Using Virtual Screening Methods To Identify Small Molecule Inhibitors of PCSK9 and Prevent Heart DiseaseDocument40 pagesUsing Virtual Screening Methods To Identify Small Molecule Inhibitors of PCSK9 and Prevent Heart DiseaseRohan Arora3% (34)
- Suicidal Inhibition or Reaction Based Inhibition PDFDocument7 pagesSuicidal Inhibition or Reaction Based Inhibition PDFMuhammad JameelNo ratings yet
- Li Weber2013Document9 pagesLi Weber2013Hector Javier BurgosNo ratings yet
- Conventional Anticancer Chemotherapy Part 1Document57 pagesConventional Anticancer Chemotherapy Part 1Jia YingNo ratings yet
- The Contribution of Lysosomes To DNA ReplicationDocument14 pagesThe Contribution of Lysosomes To DNA ReplicationErnesto RojoNo ratings yet
- 2015.05.00 MB - Caspase Methylene Blue Inhibits CaspasesDocument13 pages2015.05.00 MB - Caspase Methylene Blue Inhibits Caspasesragod2No ratings yet
- Full Text 01Document16 pagesFull Text 01mustafaNo ratings yet
- A Naturally Occurring Isoform-Specific Probe For Highly Selective and Sensitive Detection of Human Cytochrome P450 3A5Document10 pagesA Naturally Occurring Isoform-Specific Probe For Highly Selective and Sensitive Detection of Human Cytochrome P450 3A5陈梓强No ratings yet
- TNBC Oxali MoaDocument1 pageTNBC Oxali MoaAliza JafriNo ratings yet
- Clopidogrel Pharmacogenetics: Metabolism and Drug InteractionsDocument7 pagesClopidogrel Pharmacogenetics: Metabolism and Drug InteractionsUmmuNo ratings yet
- Anticancer Drugs NotesDocument112 pagesAnticancer Drugs Notesdnyanshri bhamareNo ratings yet
- Therapy: Cyclophosphamide (Cytoxan )Document12 pagesTherapy: Cyclophosphamide (Cytoxan )hasri ainunNo ratings yet
- Brahmachari Et Al - JPD-2017Document13 pagesBrahmachari Et Al - JPD-2017Saurav BrahmachariNo ratings yet
- Mol Cancer Ther-2011-Zhao-2415-25Document12 pagesMol Cancer Ther-2011-Zhao-2415-25Rahul B SNo ratings yet
- Role of Reactive Oxygen Species in p53 Activation During Cisplatin-Induced Apoptosis of Rat Mesangial CellsDocument7 pagesRole of Reactive Oxygen Species in p53 Activation During Cisplatin-Induced Apoptosis of Rat Mesangial CellsPandji 'Utuh'No ratings yet
- tmp24F6 TMPDocument20 pagestmp24F6 TMPFrontiersNo ratings yet
- Photosynthesis Process in Animals S41586-022-05499-YDocument33 pagesPhotosynthesis Process in Animals S41586-022-05499-YIjaz KhanNo ratings yet
- Mascia Amici Et Al - Neuronal Calcium Sensors and Synaptic PlasticityDocument5 pagesMascia Amici Et Al - Neuronal Calcium Sensors and Synaptic PlasticityFedrmNo ratings yet
- Tyrosine Kinases As Targets For Cancer TherapyDocument16 pagesTyrosine Kinases As Targets For Cancer TherapyfranciscoNo ratings yet
- Oxaliplatin: Drug Delivery Systems IiDocument30 pagesOxaliplatin: Drug Delivery Systems Iimerve yamanNo ratings yet
- The CamptothecinsDocument8 pagesThe CamptothecinsSanduni WickramaratneNo ratings yet
- Epand 2010Document9 pagesEpand 2010Victor MunhozNo ratings yet
- Acsami 5b06076 PDFDocument11 pagesAcsami 5b06076 PDFMandy MontgomeryNo ratings yet
- BioorgMedChem 2007 McKay Modelling - BZPDocument12 pagesBioorgMedChem 2007 McKay Modelling - BZPFred DaviersNo ratings yet
- 7.daftar Pustaka (55-56)Document2 pages7.daftar Pustaka (55-56)Rijalullah Muhammad QayyumNo ratings yet
- Contrast Radiography in Head and Neck PathologiesDocument1 pageContrast Radiography in Head and Neck PathologiesDoctor Yersong100% (1)
- Immobilization DevicesDocument59 pagesImmobilization DevicesNornia KhanNo ratings yet
- BS BuzzDocument8 pagesBS BuzzBS Central, Inc. "The Buzz"No ratings yet
- Virtual Colonoscopy: in Colorectal Cancer ScreeningDocument27 pagesVirtual Colonoscopy: in Colorectal Cancer ScreeningEwhied RuslamNo ratings yet
- Grossing, Staging, and Reporting: An Integrated Manual of Modern Surgical PathologyDocument6 pagesGrossing, Staging, and Reporting: An Integrated Manual of Modern Surgical PathologySOUMYA DEYNo ratings yet
- Department of Pathology: Histopathology Report Specimen/Site Gross DescriptionDocument1 pageDepartment of Pathology: Histopathology Report Specimen/Site Gross Descriptionamir sultanNo ratings yet
- Cancer Immunotherapy PosterDocument1 pageCancer Immunotherapy PostermisganaNo ratings yet
- 2024 International Evidence Based Kyoto Guidelines For The Management of Intraductal Papillary MucinouDocument16 pages2024 International Evidence Based Kyoto Guidelines For The Management of Intraductal Papillary MucinouLina PiñerosNo ratings yet
- Understanding Colonoscopy ENG VERSIONDocument2 pagesUnderstanding Colonoscopy ENG VERSIONto van quyenNo ratings yet
- Essay On City LifeDocument7 pagesEssay On City Lifeafibjdvvghebod100% (2)
- Radiology Concept WorkbookDocument140 pagesRadiology Concept Workbook7ywtyc8rr7No ratings yet
- Swog 8794Document7 pagesSwog 8794yingming zhuNo ratings yet
- C6.1clasificare LimfoameDocument10 pagesC6.1clasificare LimfoameRădulescu AndreeaNo ratings yet
- Embryonal Tumors of The Central Nervous System: Robert Y. Shih, LTC, MC, USA Kelly K. Koeller, MDDocument17 pagesEmbryonal Tumors of The Central Nervous System: Robert Y. Shih, LTC, MC, USA Kelly K. Koeller, MDAkhileshNo ratings yet
- Breast Cancer PresentationDocument59 pagesBreast Cancer PresentationAzilla AbdullahNo ratings yet
- Engineered Nanoparticles For Drug Delivery in CancerDocument46 pagesEngineered Nanoparticles For Drug Delivery in CancerBrunaNo ratings yet
- Tratamiento Del Carcinoma Basocelular Con Metotrexato IntralesionalDocument12 pagesTratamiento Del Carcinoma Basocelular Con Metotrexato IntralesionaltisadermaNo ratings yet
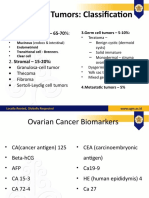
- Tumor Marker DENDocument12 pagesTumor Marker DENArtheswara SidhajatiNo ratings yet
- Oral Neoplasma IDocument31 pagesOral Neoplasma INandika 'ndek' DewaraNo ratings yet
- Cancer Research Paper Thesis StatementDocument7 pagesCancer Research Paper Thesis Statementijxnwybnd100% (1)
- 81.2 Reading - Attempt ReviewbgnjmDocument3 pages81.2 Reading - Attempt ReviewbgnjmYALEYDIS JOSELEN IGLESIAS PUMANo ratings yet
- ADANI Medical MAMMOSCAN Leaflet A3 Eng 020916Document2 pagesADANI Medical MAMMOSCAN Leaflet A3 Eng 020916eduardoNo ratings yet
- 7.016 Recitation 17 - Fall 2018: Summary of Lectures 25 (11/9) & 26 (11/14)Document9 pages7.016 Recitation 17 - Fall 2018: Summary of Lectures 25 (11/9) & 26 (11/14)Shubham singhNo ratings yet
- SolidtumorsinchildrenDocument24 pagesSolidtumorsinchildrenPriyaNo ratings yet
- Quantitative and Qualitative Analysis of P16 in HPV Positive and HPV Negative Oral Squamous Cell Carcinoma - An Immunohistochemical StudyDocument10 pagesQuantitative and Qualitative Analysis of P16 in HPV Positive and HPV Negative Oral Squamous Cell Carcinoma - An Immunohistochemical StudyIJAR JOURNALNo ratings yet
- Laparoscopic Colorectal Cancer Surgery: Makio MikeDocument107 pagesLaparoscopic Colorectal Cancer Surgery: Makio MikeBeatriz BelottiNo ratings yet
- Onco Intensive Nursing ReviewerDocument14 pagesOnco Intensive Nursing ReviewerAllysa PrestonNo ratings yet
- The Paris System For Reporting Urinary CytologyDocument9 pagesThe Paris System For Reporting Urinary Cytologyrafasp.arqtNo ratings yet
- High Dose Rate Interstitial Brachytherapy Using Two Weekly SessionsDocument1 pageHigh Dose Rate Interstitial Brachytherapy Using Two Weekly SessionsZuriNo ratings yet