Download as docx, pdf, or txt
You might also like
- Test Bank For Pathophysiology 6th Edition Jacquelyn L BanasikDocument7 pagesTest Bank For Pathophysiology 6th Edition Jacquelyn L Banasikedwardfrostxpybgdctkr100% (31)
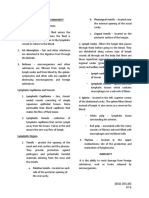
- Lymphatic SystemDocument4 pagesLymphatic Systempriya garciaNo ratings yet
- FinalsDocument5 pagesFinalsThe GreatNo ratings yet
- Is Week 1Document3 pagesIs Week 1kimmynemil80No ratings yet
- Anaphy ImmuneDocument7 pagesAnaphy ImmuneFraiza BirowaNo ratings yet
- Immune System and LymphaticsDocument7 pagesImmune System and LymphaticsCharmaine ShiellerNo ratings yet
- Chapter 1 - MicrobioDocument5 pagesChapter 1 - MicrobioFaith ManiquisNo ratings yet
- 14 Lymphatic SystemDocument3 pages14 Lymphatic SystemGracia Dela CruzNo ratings yet
- Isabela State University: Inflammatory and Immunologic ResponseDocument8 pagesIsabela State University: Inflammatory and Immunologic ResponseAbigail Basco100% (1)
- IMMUNODocument12 pagesIMMUNOwarren delizoNo ratings yet
- MSN Communicable DiseaseDocument29 pagesMSN Communicable DiseaseLuis LazaroNo ratings yet
- Immunosero (02-15-2024)Document7 pagesImmunosero (02-15-2024)Errenz Jett UlepNo ratings yet
- DRG - Dwi Leni YDocument31 pagesDRG - Dwi Leni YFaizah Ayulia NawitaNo ratings yet
- Pedia CompilationDocument44 pagesPedia Compilationlaurie.charlynjaneNo ratings yet
- The Lymphatic System and ImmunityDocument7 pagesThe Lymphatic System and ImmunityAbi ArellanoNo ratings yet
- Lymphatic System & ImmunityDocument45 pagesLymphatic System & ImmunityRika PascualNo ratings yet
- Micro NotesDocument4 pagesMicro Notesapi-680924193No ratings yet
- Biochemistry Topic 3: Concept of Immunology and InflammationDocument5 pagesBiochemistry Topic 3: Concept of Immunology and InflammationChilled Moo MooNo ratings yet
- Immune SystemDocument36 pagesImmune SystemAyessa Yvonne PanganibanNo ratings yet
- AllergenDocument2 pagesAllergenMyline TimcangNo ratings yet
- Imunologi Gizi 2016-Innate ImmuneDocument43 pagesImunologi Gizi 2016-Innate Immunemanik ayuNo ratings yet
- Kabahan Kana Notes For Exam FinalDocument33 pagesKabahan Kana Notes For Exam FinalAndree GalloNo ratings yet
- Review of Immunology: ImmunityDocument8 pagesReview of Immunology: ImmunityChan SorianoNo ratings yet
- II. Immune ResponseDocument7 pagesII. Immune ResponseMaej Marie OragaNo ratings yet
- Immunology NotesDocument26 pagesImmunology Notesmildred alidonNo ratings yet
- Suggested ResponsesDocument3 pagesSuggested ResponsesVrutika PatelNo ratings yet
- Body DefensesDocument2 pagesBody DefensesKeihla NiebresNo ratings yet
- Allergen Sensitization: Primary MediatorsDocument14 pagesAllergen Sensitization: Primary Mediatorsjelly bean100% (1)
- Inflammatory ImmunologicDocument35 pagesInflammatory Immunologickaren dapalNo ratings yet
- Anatomy & Physiology (Chapter 14 - Lymphatic System)Document18 pagesAnatomy & Physiology (Chapter 14 - Lymphatic System)Eliezer NuenayNo ratings yet
- Micro F2.Chapter 4 - 2022Document3 pagesMicro F2.Chapter 4 - 2022عبدالرحمن عابدNo ratings yet
- Non Specific and Specific Host Defense MechanismDocument7 pagesNon Specific and Specific Host Defense Mechanismcheskhadomingo33No ratings yet
- Pertaining To Extracellular Fluid Such As Plasma and Lymph. The Term Humoral Immunity Is Used To Denote Antibody Mediated Immune ResponsesDocument4 pagesPertaining To Extracellular Fluid Such As Plasma and Lymph. The Term Humoral Immunity Is Used To Denote Antibody Mediated Immune ResponsesZhon CabitacNo ratings yet
- Defense System Week 3Document28 pagesDefense System Week 3Georgette MatinNo ratings yet
- Immune SystemDocument8 pagesImmune SystemMarielle Liwanag AcostaNo ratings yet
- Week 3 Session1Document35 pagesWeek 3 Session1Khan ArishaNo ratings yet
- The Immune System: Morphofunctional Peculiarities, Methods of Examination, Semiology of DiseasesDocument45 pagesThe Immune System: Morphofunctional Peculiarities, Methods of Examination, Semiology of DiseasesHIDE & ATTACKNo ratings yet
- Topic 11 - Hypersensitivity and Autoimmuninty ProblemsDocument7 pagesTopic 11 - Hypersensitivity and Autoimmuninty ProblemsMatt Andrei P. SongcuanNo ratings yet
- BB Week 2Document7 pagesBB Week 2Claudille GawaranNo ratings yet
- Bio 2 Quiz ReviewerDocument2 pagesBio 2 Quiz ReviewerAlexandra RoderoNo ratings yet
- Lymphatic SystemDocument2 pagesLymphatic Systemmeg leeNo ratings yet
- Immuno-Sero Handout For Seminar1Document31 pagesImmuno-Sero Handout For Seminar1Jeanel Anne JovellanoNo ratings yet
- Microbiology 19 PDFDocument6 pagesMicrobiology 19 PDFLyka Villagracia AsiloNo ratings yet
- Concept of Inflammatory and Immune SystemDocument15 pagesConcept of Inflammatory and Immune SystemUchiha Dominic100% (1)
- Defense System (IMMUNITY)Document33 pagesDefense System (IMMUNITY)Restu DwikelanaNo ratings yet
- Pathophysiology of Sepsis Jcca 2022Document33 pagesPathophysiology of Sepsis Jcca 2022Ryan GusnaintinNo ratings yet
- System Immune: Dr. Dr. Zinatul Hayati, M.Kes., SP - MKDocument59 pagesSystem Immune: Dr. Dr. Zinatul Hayati, M.Kes., SP - MKRizky Nanda PutraNo ratings yet
- Serology Section in Principles of Medical Laboratory ScienceDocument3 pagesSerology Section in Principles of Medical Laboratory ScienceElle ENo ratings yet
- The Lymphatic and Immune SystemsDocument4 pagesThe Lymphatic and Immune SystemsHua YueNo ratings yet
- Specific and Non Specifc Defense of The BodyDocument38 pagesSpecific and Non Specifc Defense of The BodycedrickjamesarestaNo ratings yet
- BIO202!19!23 Immune SystemDocument55 pagesBIO202!19!23 Immune SystemAbhilash Kumar MuthuramanNo ratings yet
- ImmunoDocument2 pagesImmunoStephanie Mhae TabasaNo ratings yet
- IMMUNITY - (Allied Health Sciences) - Complete - March 2024Document51 pagesIMMUNITY - (Allied Health Sciences) - Complete - March 2024Anania EmmanuelNo ratings yet
- Infectious Disorders HandoutsDocument35 pagesInfectious Disorders Handoutsfebie pachecoNo ratings yet
- Prelims - GMJ Lecture - Module 2 III DisorderDocument5 pagesPrelims - GMJ Lecture - Module 2 III DisorderjuiceNo ratings yet
- Concept On Immune Response and Inflammation REVISEDDocument163 pagesConcept On Immune Response and Inflammation REVISEDKirk08100% (1)
- ImmunologyDocument16 pagesImmunologyShyenNo ratings yet
- 1 Handout Immunology Part 1 Barrier Immunity Innate ImmunityDocument53 pages1 Handout Immunology Part 1 Barrier Immunity Innate ImmunityIrishlyn D. DimaandalNo ratings yet
- Introduction To Immune SystemDocument37 pagesIntroduction To Immune SystemPatrick MukosoNo ratings yet
- Immunosero Trans3Document6 pagesImmunosero Trans3Jan Francis Kevin YasisNo ratings yet
- Transfer Factors: Properties, Mechanism of Action and Its Clinical ApplicationsFrom EverandTransfer Factors: Properties, Mechanism of Action and Its Clinical ApplicationsNo ratings yet
- Respi-Hema DisordersDocument10 pagesRespi-Hema DisordersggukNo ratings yet
- Fundamentals of NursingDocument11 pagesFundamentals of NursingggukNo ratings yet
- Fe & EndoDocument14 pagesFe & EndoggukNo ratings yet
- Cataract - GlaucomaDocument2 pagesCataract - GlaucomaggukNo ratings yet
- Emergency Nursing CompleteDocument9 pagesEmergency Nursing CompleteggukNo ratings yet
- Geriatric NursingDocument3 pagesGeriatric NursingggukNo ratings yet
- PALMRDocument10 pagesPALMRggukNo ratings yet
- Clinical Case Asthma WONCA 2019 RevDocument51 pagesClinical Case Asthma WONCA 2019 RevMarvi LashariNo ratings yet
- Allergy, An Atlas of Investigation and DiagnosisDocument189 pagesAllergy, An Atlas of Investigation and DiagnosisVarun Shetty100% (2)
- DR Darin Ingels - 7-28-10Document37 pagesDR Darin Ingels - 7-28-10NAA NYC Metro ChapterNo ratings yet
- Allergic Fungal Rhinosinusitis: Clinical Commentary ReviewDocument6 pagesAllergic Fungal Rhinosinusitis: Clinical Commentary ReviewPutri YunandaNo ratings yet
- Forensic Science International: Ugo Da Broi, Carlo MoreschiDocument5 pagesForensic Science International: Ugo Da Broi, Carlo MoreschiAlifiah Putri BaharuddinNo ratings yet
- (Advances in Food and Nutrition Research Volume 73) Kim, Se-Kwon-Marine Carbohydrates - Fundamentals and Applications, Part B-ADocument291 pages(Advances in Food and Nutrition Research Volume 73) Kim, Se-Kwon-Marine Carbohydrates - Fundamentals and Applications, Part B-ASugiyanto GunadiNo ratings yet
- 12 Immune System PhysiologyDocument48 pages12 Immune System PhysiologyKaye Alyssa EnriquezNo ratings yet
- New Insights Into The Pathophysiology of Allergic Rhinitis: SymposiumDocument6 pagesNew Insights Into The Pathophysiology of Allergic Rhinitis: SymposiumHarry KurniaNo ratings yet
- 4th Year Semmelweis University Itay NotesDocument41 pages4th Year Semmelweis University Itay Notesאיתי עוזרNo ratings yet
- Microbiology Final Exam MaterialDocument37 pagesMicrobiology Final Exam MaterialEdgar Mandeng100% (1)
- Allergic RhinitisDocument10 pagesAllergic Rhinitisjaikishan marathe 69No ratings yet
- 1-крок-1-ЛС-KROK 2007-2017-English - microbiologyDocument58 pages1-крок-1-ЛС-KROK 2007-2017-English - microbiologyAbhani MøhitNo ratings yet
- Nishant Respiratory SecondDocument10 pagesNishant Respiratory SecondNishantNo ratings yet
- Product Catalog 2014: Allergy & AutoimmunityDocument56 pagesProduct Catalog 2014: Allergy & AutoimmunityPeki SevicNo ratings yet
- ACCP Amiodarone Incidence Hypersensitivity To Documented ADR 2012Document5 pagesACCP Amiodarone Incidence Hypersensitivity To Documented ADR 2012Michael FreudigerNo ratings yet
- Immunoglobulins ClassDocument16 pagesImmunoglobulins ClassKoushali BanerjeeNo ratings yet
- Web 1 - Dr. Wahyuni Indawati, Sp. A (K) - Diagnosis and Management of Allergic Rhinitis in ChildrenDocument27 pagesWeb 1 - Dr. Wahyuni Indawati, Sp. A (K) - Diagnosis and Management of Allergic Rhinitis in Childrenbungkang elsaNo ratings yet
- Allergic Rhinitis: PathophysiologyDocument28 pagesAllergic Rhinitis: Pathophysiologysneh1509No ratings yet
- Kim 2019 Models of Atopic DermatitisDocument14 pagesKim 2019 Models of Atopic DermatitisBrigitta SzöllősiNo ratings yet
- Dissertation - NadineDöge - V2Document79 pagesDissertation - NadineDöge - V2rahimNo ratings yet
- Anaphylactic Death FinalDocument73 pagesAnaphylactic Death Finalkhaled eissaNo ratings yet
- A Case of Possible Hypersensitivity Reactions To Human InsulinDocument6 pagesA Case of Possible Hypersensitivity Reactions To Human Insulingandik danu pramigaNo ratings yet
- Pharmacotherapy Handbook - ALLERGIC RHINITISDocument8 pagesPharmacotherapy Handbook - ALLERGIC RHINITISstella.gillesania.chenNo ratings yet
- Antibody Structure & Function AtfDocument6 pagesAntibody Structure & Function Atfnofov45585No ratings yet
- Medical Immunology - Lecture Notes, Study Material and Important Questions, AnswersDocument99 pagesMedical Immunology - Lecture Notes, Study Material and Important Questions, AnswersM.V. TVNo ratings yet
- AllerjamDocument60 pagesAllerjamgpawankumar@rediffmail.com100% (2)
- Allergo-Immunology Hour: Food AllergyDocument32 pagesAllergo-Immunology Hour: Food AllergyJill PNo ratings yet
- Good Food, Good Mood - Gary NullDocument210 pagesGood Food, Good Mood - Gary NullJohnny Atman100% (1)
- MD - Medical Devices-8Document203 pagesMD - Medical Devices-8qvc.regulatory 2No ratings yet