Download as pdf or txt
You might also like
- Michael Tonry - Punishing Race - A Continuing American Dilemma (2011, Oxford University Press)Document221 pagesMichael Tonry - Punishing Race - A Continuing American Dilemma (2011, Oxford University Press)Par PoundzNo ratings yet
- KAREN NUÑEZ v. NORMA MOISES-PALMADocument4 pagesKAREN NUÑEZ v. NORMA MOISES-PALMARizza Angela MangallenoNo ratings yet
- What Is The Optimum Method of Weaning Intra-Aortic Balloon Pumps?Document4 pagesWhat Is The Optimum Method of Weaning Intra-Aortic Balloon Pumps?Attilio Del RossoNo ratings yet
- High-Dose vs. Low-Dose Proton Pump Inhibitors Post-Endoscopic Hemostasis in Patients With Bleeding Peptic Ulcer. A Meta-Analysis and Meta-Regression AnalysisDocument10 pagesHigh-Dose vs. Low-Dose Proton Pump Inhibitors Post-Endoscopic Hemostasis in Patients With Bleeding Peptic Ulcer. A Meta-Analysis and Meta-Regression Analysis200742 Elya AmaliaNo ratings yet
- Comparison of Surgical Outcome and Complications Between Spinal and General Anaesthesia For Patients Undergoing Percutaneous NephrolithotomyDocument5 pagesComparison of Surgical Outcome and Complications Between Spinal and General Anaesthesia For Patients Undergoing Percutaneous Nephrolithotomynaufal12345No ratings yet
- 10 - (Rahman) The Relationship Between Chest Tube Size and Clinical Outcome in Pleural InfectionDocument8 pages10 - (Rahman) The Relationship Between Chest Tube Size and Clinical Outcome in Pleural InfectionfaisaldanyaniNo ratings yet
- s12872 021 01930 WDocument11 pagess12872 021 01930 WOana DrăganNo ratings yet
- Ablacao Plexos FADocument25 pagesAblacao Plexos FAhelberttomeNo ratings yet
- 2003-Academic Emergency MedicineDocument154 pages2003-Academic Emergency MedicinealiceNo ratings yet
- What Is The Role of Screening in The Management of Abdominal Aortic AneurysmDocument7 pagesWhat Is The Role of Screening in The Management of Abdominal Aortic AneurysmShaastieNo ratings yet
- Diagnostic Assessment BeforeDocument4 pagesDiagnostic Assessment BeforeBinod KumarNo ratings yet
- Spinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDocument5 pagesSpinal vs. General Anesthesia For Percutaneous Nephrolithotomy: A Prospective Randomized TrialDella Puspita SariNo ratings yet
- Retrospective Study of The Efectiveness of REBOA For Traumatic Haemorrhagic ShockDocument6 pagesRetrospective Study of The Efectiveness of REBOA For Traumatic Haemorrhagic ShockChristianFelipePorrasCastroNo ratings yet
- The Effect of Early Canalith Repositioning On Benign Paroxysmal Positional Vertigo On RecurrenceDocument5 pagesThe Effect of Early Canalith Repositioning On Benign Paroxysmal Positional Vertigo On RecurrencezanafiraNo ratings yet
- Perioperative Reliability of An On-Site Prothrombin Time Assay Under Different Haemostatic ConditionsDocument4 pagesPerioperative Reliability of An On-Site Prothrombin Time Assay Under Different Haemostatic Conditionsbelqis ratuNo ratings yet
- Blyth 1994Document3 pagesBlyth 1994campinasovNo ratings yet
- Timing of Surgery For Congenital Diaphragmatic Hernia: Is Emergency Operation Necessary?Document4 pagesTiming of Surgery For Congenital Diaphragmatic Hernia: Is Emergency Operation Necessary?Agus PrimaNo ratings yet
- Zheng 2016Document6 pagesZheng 2016Arindya RezekiNo ratings yet
- Jagsi 2014Document9 pagesJagsi 2014Arlette M.No ratings yet
- Clinical Implications of Thrombocytopenia Among Patients Undergoing Intra Aortic BalloonDocument6 pagesClinical Implications of Thrombocytopenia Among Patients Undergoing Intra Aortic BalloonweikuohauNo ratings yet
- Record 1 - THRDocument11 pagesRecord 1 - THRNorhamdan Mohd YahayaNo ratings yet
- Chest Physiotherapy After Coronary Artery Bypass Graft Surgery-A Comparison of Three Different Deep Breathing TechniquesDocument6 pagesChest Physiotherapy After Coronary Artery Bypass Graft Surgery-A Comparison of Three Different Deep Breathing TechniquesmadeNo ratings yet
- Hemodynamic Effects of Chest-Knee Position: Comparison of Perioperative Propofol and Sevoflurane AnesthesiaDocument6 pagesHemodynamic Effects of Chest-Knee Position: Comparison of Perioperative Propofol and Sevoflurane AnesthesiaAprilico Fadhil PangestuNo ratings yet
- International Journal of Surgery Open: Sedigheh Nadri, Arash Karimi, Farzad Mohammadi, Hormoz MahmoudvandDocument7 pagesInternational Journal of Surgery Open: Sedigheh Nadri, Arash Karimi, Farzad Mohammadi, Hormoz MahmoudvandLuis ReynaNo ratings yet
- Saager2019 RECITE-US +++Document9 pagesSaager2019 RECITE-US +++Zinar PehlivanNo ratings yet
- SINPHONIDocument11 pagesSINPHONIvistamaniacNo ratings yet
- ISPR8-1143: E278 Posters (First Part) / Annals of Physical and Rehabilitation Medicine 61S (2018) E103-E308Document1 pageISPR8-1143: E278 Posters (First Part) / Annals of Physical and Rehabilitation Medicine 61S (2018) E103-E308TRIA ANo ratings yet
- Gene Therapy and The Future of Orthopaedics: J. Bone Joint Surg. AmDocument9 pagesGene Therapy and The Future of Orthopaedics: J. Bone Joint Surg. AmChrysi TsiouriNo ratings yet
- The Journal of ArthroplastyDocument8 pagesThe Journal of Arthroplasty阿欧有怪兽No ratings yet
- Aneurysm Brain and Hyperbaric Chamber AIT - Art - 37989-10Document7 pagesAneurysm Brain and Hyperbaric Chamber AIT - Art - 37989-10cooleraid884No ratings yet
- Special ArticlesDocument12 pagesSpecial ArticlesMichael Vincent MercadoNo ratings yet
- Retrospective Investigation About Anesthetic ManageDocument5 pagesRetrospective Investigation About Anesthetic ManageMariana GNo ratings yet
- Ondan Hipo 3Document5 pagesOndan Hipo 3putri maharani andesNo ratings yet
- Metanalisis 2010Document11 pagesMetanalisis 2010Elmer chavezNo ratings yet
- Nejmoa 042473Document10 pagesNejmoa 042473Sanchit PeriwalNo ratings yet
- 9829 CE (Ra) F (SH) PF1 (SNAK) PFA (P)Document4 pages9829 CE (Ra) F (SH) PF1 (SNAK) PFA (P)razaqhussain00No ratings yet
- High-Frequency Oscillation For Acute Respiratory Distress SyndromeDocument8 pagesHigh-Frequency Oscillation For Acute Respiratory Distress SyndromeLintang SuroyaNo ratings yet
- Effect of Short-Acting Beta Blocker On The Cardiac Recovery After Cardiopulmonary BypassDocument4 pagesEffect of Short-Acting Beta Blocker On The Cardiac Recovery After Cardiopulmonary BypasshobbitNo ratings yet
- The Effect of Intraoperative Alkali Treatment On Recovery From Atracurium-Induced Neuromuscular Blockade in Renal Transplantation: A Randomized TrialDocument4 pagesThe Effect of Intraoperative Alkali Treatment On Recovery From Atracurium-Induced Neuromuscular Blockade in Renal Transplantation: A Randomized Trialakhirul_733759154No ratings yet
- Trial CPRDocument12 pagesTrial CPRgabriella_jabirNo ratings yet
- Sumber DuaDocument6 pagesSumber DuaadiNo ratings yet
- 1 s2.0 S0929664617300487 MainDocument8 pages1 s2.0 S0929664617300487 MainSuryati HusinNo ratings yet
- Transversus Abdominis Plane Block: Eview RticleDocument17 pagesTransversus Abdominis Plane Block: Eview RticleAYŞE GÜLŞAH ATASEVERNo ratings yet
- Plante 2010Document5 pagesPlante 2010William KamarullahNo ratings yet
- Doshi 2005Document6 pagesDoshi 2005Luba D'AndreaNo ratings yet
- A Randomized Controlled Trial of Endovascular Aneurysm Repair Versus Open Surgery For Abdominal Aortic Aneurysms in Low - To Moderate-Risk PatientsDocument8 pagesA Randomized Controlled Trial of Endovascular Aneurysm Repair Versus Open Surgery For Abdominal Aortic Aneurysms in Low - To Moderate-Risk Patientsvfd08051996No ratings yet
- Inhibition of Nitrate Tolerance Without Reducing Vascular Response During Eccentric Dosing of NitratesDocument8 pagesInhibition of Nitrate Tolerance Without Reducing Vascular Response During Eccentric Dosing of Nitrates568974No ratings yet
- Jos 2015 01655Document14 pagesJos 2015 01655Arvin Anwar SamanteNo ratings yet
- 00003Document8 pages00003Anonymous zPwXqwNo ratings yet
- Mehu107 U2 T1 RCP Artículo 2Document8 pagesMehu107 U2 T1 RCP Artículo 2Stefani AtlleNo ratings yet
- Yilmaz, 2006Document7 pagesYilmaz, 2006titaNo ratings yet
- AC After StrokeDocument6 pagesAC After StrokeDileepa chathurangaNo ratings yet
- Wheeler 2016Document4 pagesWheeler 2016Alvaro Fabian Córdova WhiteleyNo ratings yet
- Intravenous Thrombolytic Therapy For Acute Ischemic StrokeDocument12 pagesIntravenous Thrombolytic Therapy For Acute Ischemic Strokeidno1008100% (1)
- Schneider 2017Document7 pagesSchneider 2017RafailiaNo ratings yet
- Anestesi Umum Dan Regional Untuk Operasi Fraktur Hip: Ameta-Analisis Uji Coba Secara AcakDocument13 pagesAnestesi Umum Dan Regional Untuk Operasi Fraktur Hip: Ameta-Analisis Uji Coba Secara AcakmardianaNo ratings yet
- Tenecteplase To Replace Alteplase Comparing ThromDocument2 pagesTenecteplase To Replace Alteplase Comparing ThromAlex DegraciaNo ratings yet
- New England Journal Medicine: The ofDocument10 pagesNew England Journal Medicine: The ofNatalia ArizaNo ratings yet
- Epinephrine During Resuscitation of Traumatic Cardiac Arrest and Increased Mortality: A Post Hoc Analysis of Prospective Observational StudyDocument9 pagesEpinephrine During Resuscitation of Traumatic Cardiac Arrest and Increased Mortality: A Post Hoc Analysis of Prospective Observational StudymaithilicharanNo ratings yet
- Skoretz 2014Document8 pagesSkoretz 2014Gonzalo FragaNo ratings yet
- Evolving Paradigm Shifts: Acute PE ManagementDocument53 pagesEvolving Paradigm Shifts: Acute PE Managementadamu mohammadNo ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- Ciep 257 - Turma 1017Document14 pagesCiep 257 - Turma 1017Rafael LimaNo ratings yet
- Admission Form Eleven Class Mar 2016Document3 pagesAdmission Form Eleven Class Mar 2016Aaqib AliNo ratings yet
- MRP PDFDocument45 pagesMRP PDFSamNo ratings yet
- War and Peace in Outer Space Law Policy and Ethics 1St Edition Cassandra Steer Editor Ebook Full ChapterDocument35 pagesWar and Peace in Outer Space Law Policy and Ethics 1St Edition Cassandra Steer Editor Ebook Full Chaptergarry.giordano804100% (7)
- E-Auctions - MSTC Limited-TATA POWER HALDIADocument7 pagesE-Auctions - MSTC Limited-TATA POWER HALDIAmannakauNo ratings yet
- For The Full Essay Please WHATSAPP 010-2504287: Assignment / TugasanDocument16 pagesFor The Full Essay Please WHATSAPP 010-2504287: Assignment / TugasanSimon RajNo ratings yet
- Simulation AssignmentDocument10 pagesSimulation Assignmentsyeda maryemNo ratings yet
- Hard TimesDocument3 pagesHard TimesPaola LamannaNo ratings yet
- Bicilavadora-Ideas05 PedlingDocument11 pagesBicilavadora-Ideas05 PedlingAnonymous GEHeEQlajbNo ratings yet
- Albanian Armenian CelticDocument25 pagesAlbanian Armenian CelticdavayNo ratings yet
- The Christian in Complete Armour or A Treatise On The Saint's War With The Devil William Gurnall 1655 Vol 2Document453 pagesThe Christian in Complete Armour or A Treatise On The Saint's War With The Devil William Gurnall 1655 Vol 2Spirit of William Tyndale50% (2)
- Tax267 Ss Feb2022Document10 pagesTax267 Ss Feb20228kbnhhkwppNo ratings yet
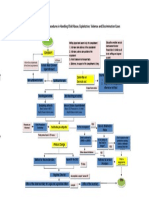
- Rules and Procedures in Handling Child Abuse CasesDocument1 pageRules and Procedures in Handling Child Abuse CasesJoyce Carreon50% (2)
- Analysis of Overlay For Airport Pavements CEAT Interrim ReportDocument54 pagesAnalysis of Overlay For Airport Pavements CEAT Interrim ReportJimmy ThomasNo ratings yet
- Simatic Step7 Graph7Document212 pagesSimatic Step7 Graph7loadsach100% (1)
- FencingDocument2 pagesFencingBounna PhoumalavongNo ratings yet
- A Flangeless Complete Denture Prosthesis A Case Report April 2017 7862206681 3603082Document2 pagesA Flangeless Complete Denture Prosthesis A Case Report April 2017 7862206681 3603082wdyNo ratings yet
- Lecture Note 5 - BSB315 - LIFE CYCLE COST CALCULATIONDocument24 pagesLecture Note 5 - BSB315 - LIFE CYCLE COST CALCULATIONnur sheNo ratings yet
- From Demon To Deity Kang Wang in Thirteenth-Century Jizhou and BeyondDocument31 pagesFrom Demon To Deity Kang Wang in Thirteenth-Century Jizhou and BeyondLiping ZhuNo ratings yet
- Conjugarea Verbului Manifesta: Indicativ PrezentDocument4 pagesConjugarea Verbului Manifesta: Indicativ PrezentAndrei PleșaNo ratings yet
- Partograph 3Document49 pagesPartograph 3Geeta BhardwajNo ratings yet
- Advanced Presentation Skills WorkshopDocument34 pagesAdvanced Presentation Skills WorkshopJade Cemre ErciyesNo ratings yet
- Test Bank For Child Development A Thematic Approach 6th EditionDocument6 pagesTest Bank For Child Development A Thematic Approach 6th EditionCharles Pando100% (44)
- A. Scriabin - MysteriumDocument18 pagesA. Scriabin - MysteriumAleksandar GrgićNo ratings yet
- Module 4Document15 pagesModule 4trishia marie monteraNo ratings yet
- Setting Up A Home VPN Server Using A Raspberry Pi - SitepointDocument33 pagesSetting Up A Home VPN Server Using A Raspberry Pi - SitepointSteve AttwoodNo ratings yet
- Literature Review of Water Level SensorDocument4 pagesLiterature Review of Water Level Sensorc5mr3mxf100% (1)
- Ajit ResumeDocument3 pagesAjit ResumeSreeluNo ratings yet