
Economics of Stem Cell Transplantation For Lymphoma: Counting The Cost of Living
Economics of Stem Cell Transplantation For Lymphoma: Counting The Cost of Living
You might also like
- History of Present IllnessDocument7 pagesHistory of Present IllnessBena GichiaNo ratings yet
- Hepb y RTX PDFDocument3 pagesHepb y RTX PDFYeli VeMeNo ratings yet
- Medical and Pediatric Oncology Volume 34 Issue 2 2000 (Doi 10.1002 - (Sici) 1096-911x (200002) 34!2!92 - Aid-Mpo3 - 3.0.co 2-q) Bennett, Charles L. Stinson, Tammy J. Lane, David AmyloDocument5 pagesMedical and Pediatric Oncology Volume 34 Issue 2 2000 (Doi 10.1002 - (Sici) 1096-911x (200002) 34!2!92 - Aid-Mpo3 - 3.0.co 2-q) Bennett, Charles L. Stinson, Tammy J. Lane, David AmyloNisha RehmanNo ratings yet
- Koay 2020Document30 pagesKoay 2020Laura QuirozNo ratings yet
- Cost-Minimization Analysis of Adjuvant Chemotherapy Regimens Given To Patients With Colorectal Cancer in JapanDocument9 pagesCost-Minimization Analysis of Adjuvant Chemotherapy Regimens Given To Patients With Colorectal Cancer in JapanRizki MartaNo ratings yet
- 2021 Consolidation Theraphy in Esophageal CancerDocument6 pages2021 Consolidation Theraphy in Esophageal CancerykommNo ratings yet
- Thrombolitic TeraphyDocument8 pagesThrombolitic TeraphyFyan FiradyNo ratings yet
- TX CancerDocument5 pagesTX CancerChelsea Reyna TolentinoNo ratings yet
- Curroncol 28 00070 v2Document10 pagesCurroncol 28 00070 v2DARA. AZESTI.No ratings yet
- BR J Haematol - 2019 - Hills - Evaluating Sixty Years of UK Trials Research in Acute Myeloid Leukaemia Lessons For TrialDocument7 pagesBR J Haematol - 2019 - Hills - Evaluating Sixty Years of UK Trials Research in Acute Myeloid Leukaemia Lessons For TrialMarcellia AngelinaNo ratings yet
- Garcia-Contreras F, Del-Angel-Garcia G, Cuenca A R, Malvaez-Valdes M, Yanez A V, Amato DDocument4 pagesGarcia-Contreras F, Del-Angel-Garcia G, Cuenca A R, Malvaez-Valdes M, Yanez A V, Amato DNilo Huamani FloresNo ratings yet
- 1094 FullDocument6 pages1094 FullGuido ABNo ratings yet
- CPCNP MTXDocument9 pagesCPCNP MTXMary CogolloNo ratings yet
- Bodansky-2017-Potential Cost Savings by MinimiDocument4 pagesBodansky-2017-Potential Cost Savings by MinimiGökhanNo ratings yet
- Integrated Care: Peritoneal Dialysis International, Vol. 21 (2001), Supplement 3Document6 pagesIntegrated Care: Peritoneal Dialysis International, Vol. 21 (2001), Supplement 3Remberto RamosNo ratings yet
- Cherukuri Et Al. 2018 - Home Haemodialysis Treatment and Outcomes, Retrospective Analysis of KIHDNEyDocument10 pagesCherukuri Et Al. 2018 - Home Haemodialysis Treatment and Outcomes, Retrospective Analysis of KIHDNEyShareDialysisNo ratings yet
- Article 4Document7 pagesArticle 4nindafathiaNo ratings yet
- Final Arianna Boja Research ProposalDocument6 pagesFinal Arianna Boja Research Proposalapi-612090246No ratings yet
- Aujesky 2005Document2 pagesAujesky 2005Devanti EkaNo ratings yet
- Weeks 2016Document15 pagesWeeks 2016InêsNo ratings yet
- Neoadjuvant Paclitaxel For Operable Breast Cancer: Multicenter Phase II Trial With Clinical OutcomesDocument6 pagesNeoadjuvant Paclitaxel For Operable Breast Cancer: Multicenter Phase II Trial With Clinical OutcomesSubhash SugathanNo ratings yet
- NSCLCMADocument9 pagesNSCLCMAapi-26302710No ratings yet
- 1 s2.0 S1556086415317809 MainDocument7 pages1 s2.0 S1556086415317809 MainBegoña MartinezNo ratings yet
- Antikoagulan Untuk VTEDocument6 pagesAntikoagulan Untuk VTEVendi Cahyadi RiandikaNo ratings yet
- Ni Hms 574605Document17 pagesNi Hms 574605circe5690No ratings yet
- Critical Reviews in Oncology / Hematology: A B C B B B C DDocument7 pagesCritical Reviews in Oncology / Hematology: A B C B B B C DDiogo RodriguesNo ratings yet
- The Journal of Rheumatology Volume 38, No. 8Document4 pagesThe Journal of Rheumatology Volume 38, No. 8Jeff LapianNo ratings yet
- Weycker 2014Document11 pagesWeycker 2014ninaimoyaNo ratings yet
- Chest.126.2.592 MBE EN UCIDocument9 pagesChest.126.2.592 MBE EN UCIJaime RomeroNo ratings yet
- Costs Associated With Complications Are Lower With Capecitabine Than With 5-Fluorouracil in Patients With Colorectal CancerDocument12 pagesCosts Associated With Complications Are Lower With Capecitabine Than With 5-Fluorouracil in Patients With Colorectal CancerDelfina HuangNo ratings yet
- tmp78F6 TMPDocument16 pagestmp78F6 TMPFrontiersNo ratings yet
- Dietary Supplement Use in Ambulatory Cancer Patients: A Survey On Prevalence, Motivation and AttitudesDocument9 pagesDietary Supplement Use in Ambulatory Cancer Patients: A Survey On Prevalence, Motivation and AttitudespilarerasoNo ratings yet
- Jurnal BTKV DodiDocument10 pagesJurnal BTKV DodiAchmad Dodi MeidiantoNo ratings yet
- Cost AvoidanceDocument7 pagesCost AvoidanceAnmol KumarNo ratings yet
- Title: Comparative Effectiveness of First-Line and Alternative Antibiotic Regimens For Non-Severe Community Acquired PneumoniaDocument2 pagesTitle: Comparative Effectiveness of First-Line and Alternative Antibiotic Regimens For Non-Severe Community Acquired PneumoniaBritanyOchoaNo ratings yet
- Anesth Analg-2012-Corcoran-640-51 PDFDocument12 pagesAnesth Analg-2012-Corcoran-640-51 PDFBijay KC100% (1)
- Cost-Utility Analysis of Radiation Treatment ModalitiesDocument14 pagesCost-Utility Analysis of Radiation Treatment ModalitiesMuhammad ilyas ApotekerNo ratings yet
- GapsDocument6 pagesGapsapi-432489466No ratings yet
- Estey 2020Document73 pagesEstey 2020drToikNo ratings yet
- Lung CancerDocument8 pagesLung CancerduonghuyenNo ratings yet
- Diabetic Foot Ulcer: An Evidence-Based Treatment UpdateDocument16 pagesDiabetic Foot Ulcer: An Evidence-Based Treatment UpdateAhmad JamaluddinNo ratings yet
- Effect of A Centralized Clinical Pharmacy Anticoagulation Service On The Outcomes of Anticoagulation TherapyDocument8 pagesEffect of A Centralized Clinical Pharmacy Anticoagulation Service On The Outcomes of Anticoagulation TherapyDyla FaradhylaNo ratings yet
- Cba 2Document2 pagesCba 2Najib Al FatinNo ratings yet
- EffectivenessOfMulti DrugregimDocument11 pagesEffectivenessOfMulti Drugregimruth angelinaNo ratings yet
- 10 1016@j Ejca 2019 10 025Document8 pages10 1016@j Ejca 2019 10 025habib diopNo ratings yet
- Estimating The Costs of Hospital Acquired InfectionDocument19 pagesEstimating The Costs of Hospital Acquired InfectionMatthew KuenzelNo ratings yet
- Determinants and Outcomes of Adherence To Recommendations From A Multidisciplinary Tumour Conference For Hepatocellular CarcinomaDocument7 pagesDeterminants and Outcomes of Adherence To Recommendations From A Multidisciplinary Tumour Conference For Hepatocellular CarcinomahilalNo ratings yet
- Allen2021 Article ChemotherapyVersusChemotherapyDocument8 pagesAllen2021 Article ChemotherapyVersusChemotherapyXavier QuinteroNo ratings yet
- Pan 2014Document5 pagesPan 2014Rafaela Queiroz MascarenhasNo ratings yet
- Economic Evaluation in Critical CareDocument10 pagesEconomic Evaluation in Critical Careapi-3832022No ratings yet
- 2018 Cuidado de La HTA, Rol Del FarmacDocument2 pages2018 Cuidado de La HTA, Rol Del FarmacMóxī AckermanNo ratings yet
- Cost-E Ectiveness Analysis For Midostaurin Versus Standard of Care in Acute Myeloid Leukemia in The United KingdomDocument13 pagesCost-E Ectiveness Analysis For Midostaurin Versus Standard of Care in Acute Myeloid Leukemia in The United KingdomSri MulyaniNo ratings yet
- DC Vaksin For GBM-Jurnal RevisiDocument8 pagesDC Vaksin For GBM-Jurnal Revisiallyssa rahmadittaNo ratings yet
- Treatment of Patients With Small-Cell Lung Cancer From Meta-AnalysesDocument9 pagesTreatment of Patients With Small-Cell Lung Cancer From Meta-AnalysesmaleticjNo ratings yet
- Treatment of The Elderly When Cure Is The GoalDocument8 pagesTreatment of The Elderly When Cure Is The GoalCatia AraujoNo ratings yet
- Circulation 2012 Vieira S145 50Document7 pagesCirculation 2012 Vieira S145 50pasebanjatiNo ratings yet
- Capsule ProposalDocument6 pagesCapsule Proposaltho2793No ratings yet
- Cost-Effectiveness of Supervised Exercise Therapy Compared With Endovascular Revascularization For Intermittent ClaudicationDocument10 pagesCost-Effectiveness of Supervised Exercise Therapy Compared With Endovascular Revascularization For Intermittent ClaudicationUday PrabhuNo ratings yet
- Comparative Efficacy of Different Chemotherapies For Non-Hodgkin Lymphoma: A Network-Meta AnalysisDocument10 pagesComparative Efficacy of Different Chemotherapies For Non-Hodgkin Lymphoma: A Network-Meta AnalysisRicky Cornelius TariganNo ratings yet
- Endpoints in Advanced Breast Cancer: Methodological Aspects & Clinical ImplicationsDocument6 pagesEndpoints in Advanced Breast Cancer: Methodological Aspects & Clinical ImplicationsJauhar FirdausNo ratings yet
- Precision Medicine Oncology: A PrimerFrom EverandPrecision Medicine Oncology: A PrimerLorna Rodriguez-RodriguezNo ratings yet
- Cryo SurgeryDocument21 pagesCryo SurgeryTamarai selviNo ratings yet
- Renal Tubular DisordersDocument40 pagesRenal Tubular DisordersHitesh TanwarNo ratings yet
- Cancer Detection by Machine LearningDocument7 pagesCancer Detection by Machine Learningsiddub1721No ratings yet
- 3.6.2020 Final Final Manual - Logbook For Students For Adult 2Document34 pages3.6.2020 Final Final Manual - Logbook For Students For Adult 2Drmirfat AlkashifNo ratings yet
- Pash Syndrome Co-Existing With Rheumatic Heart Disease and Severe Mitral Valve Regurgitation: A Rare Case ReportDocument3 pagesPash Syndrome Co-Existing With Rheumatic Heart Disease and Severe Mitral Valve Regurgitation: A Rare Case ReportIJAR JOURNALNo ratings yet
- Blu Moderno Scientifico PosterDocument5 pagesBlu Moderno Scientifico Posterlely.ca.94No ratings yet
- AP 1 Transcription Factor As Precursor of PostZika and MS SymptomsDocument22 pagesAP 1 Transcription Factor As Precursor of PostZika and MS SymptomsElton MatsushimaNo ratings yet
- COVID-19 Vaccines For Children and Teens - CDCDocument5 pagesCOVID-19 Vaccines For Children and Teens - CDCFabio PicassoNo ratings yet
- Domestic Violence and AbuseDocument7 pagesDomestic Violence and AbuseKate20100% (1)
- HEALTH 8: Communicable DiseaseDocument31 pagesHEALTH 8: Communicable DiseaseElissah S PabilonaNo ratings yet
- Dka Guide Line Version 3Document8 pagesDka Guide Line Version 3Zainab BasimNo ratings yet
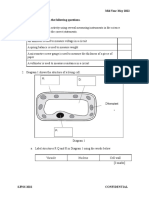
- F2 Mid-Year Exam Section BDocument3 pagesF2 Mid-Year Exam Section BAnne Marian Anak JOSEPHNo ratings yet
- Claire Dahyot Fizelier Ceftriaxone To Prevent EarlyDocument11 pagesClaire Dahyot Fizelier Ceftriaxone To Prevent EarlyFermin LombardiaNo ratings yet
- Insulin PregnancyDocument23 pagesInsulin PregnancymytriciallorinNo ratings yet
- Microsoft Word - DS03 - Paper - 1.1Document8 pagesMicrosoft Word - DS03 - Paper - 1.1kuridisanjeevNo ratings yet
- AnaphylaxisDocument1 pageAnaphylaxisherdind prayogaNo ratings yet
- Ortho Final ExamDocument40 pagesOrtho Final ExamMariane GumbanNo ratings yet
- Superhero AssignmentDocument5 pagesSuperhero Assignmentprathibha asok kumarNo ratings yet
- Natural Homeopathic Medicine For Balanitis - Homeopathy atDocument7 pagesNatural Homeopathic Medicine For Balanitis - Homeopathy atDhandapani VNo ratings yet
- Health Ass.Document6 pagesHealth Ass.Rashmi Devrani VyasNo ratings yet
- Pointers To ReviewDocument18 pagesPointers To ReviewHegi Ann AlcalaNo ratings yet
- Oral Halitosis: Definitions: Breath Malodor, Defined As Foul or Offensive Odor of Expired Air, May BeDocument7 pagesOral Halitosis: Definitions: Breath Malodor, Defined As Foul or Offensive Odor of Expired Air, May BeSnowNo ratings yet
- Neck Trauma DR Hauwa Shitu 1Document40 pagesNeck Trauma DR Hauwa Shitu 1Hauwa shitu.B100% (1)
- Consensus Based Guidelines For The Recognition,.15Document13 pagesConsensus Based Guidelines For The Recognition,.15ms98alissaNo ratings yet
- Indicador Gabs AtualizadoDocument2 pagesIndicador Gabs AtualizadoBiXus Estrategas EmpresarialesNo ratings yet
- Breast Cancer Assessment ChartDocument2 pagesBreast Cancer Assessment ChartNigel Leigh Godfrey GutierrezNo ratings yet
- 1 s2.0 S2473952921007515 MainDocument10 pages1 s2.0 S2473952921007515 MainAndreea RacovitaNo ratings yet
- A Family Case Presentation, SLHDocument27 pagesA Family Case Presentation, SLHRajanNo ratings yet
- Diagnostic Diferential Medicina InternaDocument6 pagesDiagnostic Diferential Medicina InternaLary ArNo ratings yet
























































































Download as pdf or txt
You might also like
- History of Present IllnessDocument7 pagesHistory of Present IllnessBena GichiaNo ratings yet
- Hepb y RTX PDFDocument3 pagesHepb y RTX PDFYeli VeMeNo ratings yet
- Medical and Pediatric Oncology Volume 34 Issue 2 2000 (Doi 10.1002 - (Sici) 1096-911x (200002) 34!2!92 - Aid-Mpo3 - 3.0.co 2-q) Bennett, Charles L. Stinson, Tammy J. Lane, David AmyloDocument5 pagesMedical and Pediatric Oncology Volume 34 Issue 2 2000 (Doi 10.1002 - (Sici) 1096-911x (200002) 34!2!92 - Aid-Mpo3 - 3.0.co 2-q) Bennett, Charles L. Stinson, Tammy J. Lane, David AmyloNisha RehmanNo ratings yet
- Koay 2020Document30 pagesKoay 2020Laura QuirozNo ratings yet
- Cost-Minimization Analysis of Adjuvant Chemotherapy Regimens Given To Patients With Colorectal Cancer in JapanDocument9 pagesCost-Minimization Analysis of Adjuvant Chemotherapy Regimens Given To Patients With Colorectal Cancer in JapanRizki MartaNo ratings yet
- 2021 Consolidation Theraphy in Esophageal CancerDocument6 pages2021 Consolidation Theraphy in Esophageal CancerykommNo ratings yet
- Thrombolitic TeraphyDocument8 pagesThrombolitic TeraphyFyan FiradyNo ratings yet
- TX CancerDocument5 pagesTX CancerChelsea Reyna TolentinoNo ratings yet
- Curroncol 28 00070 v2Document10 pagesCurroncol 28 00070 v2DARA. AZESTI.No ratings yet
- BR J Haematol - 2019 - Hills - Evaluating Sixty Years of UK Trials Research in Acute Myeloid Leukaemia Lessons For TrialDocument7 pagesBR J Haematol - 2019 - Hills - Evaluating Sixty Years of UK Trials Research in Acute Myeloid Leukaemia Lessons For TrialMarcellia AngelinaNo ratings yet
- Garcia-Contreras F, Del-Angel-Garcia G, Cuenca A R, Malvaez-Valdes M, Yanez A V, Amato DDocument4 pagesGarcia-Contreras F, Del-Angel-Garcia G, Cuenca A R, Malvaez-Valdes M, Yanez A V, Amato DNilo Huamani FloresNo ratings yet
- 1094 FullDocument6 pages1094 FullGuido ABNo ratings yet
- CPCNP MTXDocument9 pagesCPCNP MTXMary CogolloNo ratings yet
- Bodansky-2017-Potential Cost Savings by MinimiDocument4 pagesBodansky-2017-Potential Cost Savings by MinimiGökhanNo ratings yet
- Integrated Care: Peritoneal Dialysis International, Vol. 21 (2001), Supplement 3Document6 pagesIntegrated Care: Peritoneal Dialysis International, Vol. 21 (2001), Supplement 3Remberto RamosNo ratings yet
- Cherukuri Et Al. 2018 - Home Haemodialysis Treatment and Outcomes, Retrospective Analysis of KIHDNEyDocument10 pagesCherukuri Et Al. 2018 - Home Haemodialysis Treatment and Outcomes, Retrospective Analysis of KIHDNEyShareDialysisNo ratings yet
- Article 4Document7 pagesArticle 4nindafathiaNo ratings yet
- Final Arianna Boja Research ProposalDocument6 pagesFinal Arianna Boja Research Proposalapi-612090246No ratings yet
- Aujesky 2005Document2 pagesAujesky 2005Devanti EkaNo ratings yet
- Weeks 2016Document15 pagesWeeks 2016InêsNo ratings yet
- Neoadjuvant Paclitaxel For Operable Breast Cancer: Multicenter Phase II Trial With Clinical OutcomesDocument6 pagesNeoadjuvant Paclitaxel For Operable Breast Cancer: Multicenter Phase II Trial With Clinical OutcomesSubhash SugathanNo ratings yet
- NSCLCMADocument9 pagesNSCLCMAapi-26302710No ratings yet
- 1 s2.0 S1556086415317809 MainDocument7 pages1 s2.0 S1556086415317809 MainBegoña MartinezNo ratings yet
- Antikoagulan Untuk VTEDocument6 pagesAntikoagulan Untuk VTEVendi Cahyadi RiandikaNo ratings yet
- Ni Hms 574605Document17 pagesNi Hms 574605circe5690No ratings yet
- Critical Reviews in Oncology / Hematology: A B C B B B C DDocument7 pagesCritical Reviews in Oncology / Hematology: A B C B B B C DDiogo RodriguesNo ratings yet
- The Journal of Rheumatology Volume 38, No. 8Document4 pagesThe Journal of Rheumatology Volume 38, No. 8Jeff LapianNo ratings yet
- Weycker 2014Document11 pagesWeycker 2014ninaimoyaNo ratings yet
- Chest.126.2.592 MBE EN UCIDocument9 pagesChest.126.2.592 MBE EN UCIJaime RomeroNo ratings yet
- Costs Associated With Complications Are Lower With Capecitabine Than With 5-Fluorouracil in Patients With Colorectal CancerDocument12 pagesCosts Associated With Complications Are Lower With Capecitabine Than With 5-Fluorouracil in Patients With Colorectal CancerDelfina HuangNo ratings yet
- tmp78F6 TMPDocument16 pagestmp78F6 TMPFrontiersNo ratings yet
- Dietary Supplement Use in Ambulatory Cancer Patients: A Survey On Prevalence, Motivation and AttitudesDocument9 pagesDietary Supplement Use in Ambulatory Cancer Patients: A Survey On Prevalence, Motivation and AttitudespilarerasoNo ratings yet
- Jurnal BTKV DodiDocument10 pagesJurnal BTKV DodiAchmad Dodi MeidiantoNo ratings yet
- Cost AvoidanceDocument7 pagesCost AvoidanceAnmol KumarNo ratings yet
- Title: Comparative Effectiveness of First-Line and Alternative Antibiotic Regimens For Non-Severe Community Acquired PneumoniaDocument2 pagesTitle: Comparative Effectiveness of First-Line and Alternative Antibiotic Regimens For Non-Severe Community Acquired PneumoniaBritanyOchoaNo ratings yet
- Anesth Analg-2012-Corcoran-640-51 PDFDocument12 pagesAnesth Analg-2012-Corcoran-640-51 PDFBijay KC100% (1)
- Cost-Utility Analysis of Radiation Treatment ModalitiesDocument14 pagesCost-Utility Analysis of Radiation Treatment ModalitiesMuhammad ilyas ApotekerNo ratings yet
- GapsDocument6 pagesGapsapi-432489466No ratings yet
- Estey 2020Document73 pagesEstey 2020drToikNo ratings yet
- Lung CancerDocument8 pagesLung CancerduonghuyenNo ratings yet
- Diabetic Foot Ulcer: An Evidence-Based Treatment UpdateDocument16 pagesDiabetic Foot Ulcer: An Evidence-Based Treatment UpdateAhmad JamaluddinNo ratings yet
- Effect of A Centralized Clinical Pharmacy Anticoagulation Service On The Outcomes of Anticoagulation TherapyDocument8 pagesEffect of A Centralized Clinical Pharmacy Anticoagulation Service On The Outcomes of Anticoagulation TherapyDyla FaradhylaNo ratings yet
- Cba 2Document2 pagesCba 2Najib Al FatinNo ratings yet
- EffectivenessOfMulti DrugregimDocument11 pagesEffectivenessOfMulti Drugregimruth angelinaNo ratings yet
- 10 1016@j Ejca 2019 10 025Document8 pages10 1016@j Ejca 2019 10 025habib diopNo ratings yet
- Estimating The Costs of Hospital Acquired InfectionDocument19 pagesEstimating The Costs of Hospital Acquired InfectionMatthew KuenzelNo ratings yet
- Determinants and Outcomes of Adherence To Recommendations From A Multidisciplinary Tumour Conference For Hepatocellular CarcinomaDocument7 pagesDeterminants and Outcomes of Adherence To Recommendations From A Multidisciplinary Tumour Conference For Hepatocellular CarcinomahilalNo ratings yet
- Allen2021 Article ChemotherapyVersusChemotherapyDocument8 pagesAllen2021 Article ChemotherapyVersusChemotherapyXavier QuinteroNo ratings yet
- Pan 2014Document5 pagesPan 2014Rafaela Queiroz MascarenhasNo ratings yet
- Economic Evaluation in Critical CareDocument10 pagesEconomic Evaluation in Critical Careapi-3832022No ratings yet
- 2018 Cuidado de La HTA, Rol Del FarmacDocument2 pages2018 Cuidado de La HTA, Rol Del FarmacMóxī AckermanNo ratings yet
- Cost-E Ectiveness Analysis For Midostaurin Versus Standard of Care in Acute Myeloid Leukemia in The United KingdomDocument13 pagesCost-E Ectiveness Analysis For Midostaurin Versus Standard of Care in Acute Myeloid Leukemia in The United KingdomSri MulyaniNo ratings yet
- DC Vaksin For GBM-Jurnal RevisiDocument8 pagesDC Vaksin For GBM-Jurnal Revisiallyssa rahmadittaNo ratings yet
- Treatment of Patients With Small-Cell Lung Cancer From Meta-AnalysesDocument9 pagesTreatment of Patients With Small-Cell Lung Cancer From Meta-AnalysesmaleticjNo ratings yet
- Treatment of The Elderly When Cure Is The GoalDocument8 pagesTreatment of The Elderly When Cure Is The GoalCatia AraujoNo ratings yet
- Circulation 2012 Vieira S145 50Document7 pagesCirculation 2012 Vieira S145 50pasebanjatiNo ratings yet
- Capsule ProposalDocument6 pagesCapsule Proposaltho2793No ratings yet
- Cost-Effectiveness of Supervised Exercise Therapy Compared With Endovascular Revascularization For Intermittent ClaudicationDocument10 pagesCost-Effectiveness of Supervised Exercise Therapy Compared With Endovascular Revascularization For Intermittent ClaudicationUday PrabhuNo ratings yet
- Comparative Efficacy of Different Chemotherapies For Non-Hodgkin Lymphoma: A Network-Meta AnalysisDocument10 pagesComparative Efficacy of Different Chemotherapies For Non-Hodgkin Lymphoma: A Network-Meta AnalysisRicky Cornelius TariganNo ratings yet
- Endpoints in Advanced Breast Cancer: Methodological Aspects & Clinical ImplicationsDocument6 pagesEndpoints in Advanced Breast Cancer: Methodological Aspects & Clinical ImplicationsJauhar FirdausNo ratings yet
- Precision Medicine Oncology: A PrimerFrom EverandPrecision Medicine Oncology: A PrimerLorna Rodriguez-RodriguezNo ratings yet
- Cryo SurgeryDocument21 pagesCryo SurgeryTamarai selviNo ratings yet
- Renal Tubular DisordersDocument40 pagesRenal Tubular DisordersHitesh TanwarNo ratings yet
- Cancer Detection by Machine LearningDocument7 pagesCancer Detection by Machine Learningsiddub1721No ratings yet
- 3.6.2020 Final Final Manual - Logbook For Students For Adult 2Document34 pages3.6.2020 Final Final Manual - Logbook For Students For Adult 2Drmirfat AlkashifNo ratings yet
- Pash Syndrome Co-Existing With Rheumatic Heart Disease and Severe Mitral Valve Regurgitation: A Rare Case ReportDocument3 pagesPash Syndrome Co-Existing With Rheumatic Heart Disease and Severe Mitral Valve Regurgitation: A Rare Case ReportIJAR JOURNALNo ratings yet
- Blu Moderno Scientifico PosterDocument5 pagesBlu Moderno Scientifico Posterlely.ca.94No ratings yet
- AP 1 Transcription Factor As Precursor of PostZika and MS SymptomsDocument22 pagesAP 1 Transcription Factor As Precursor of PostZika and MS SymptomsElton MatsushimaNo ratings yet
- COVID-19 Vaccines For Children and Teens - CDCDocument5 pagesCOVID-19 Vaccines For Children and Teens - CDCFabio PicassoNo ratings yet
- Domestic Violence and AbuseDocument7 pagesDomestic Violence and AbuseKate20100% (1)
- HEALTH 8: Communicable DiseaseDocument31 pagesHEALTH 8: Communicable DiseaseElissah S PabilonaNo ratings yet
- Dka Guide Line Version 3Document8 pagesDka Guide Line Version 3Zainab BasimNo ratings yet
- F2 Mid-Year Exam Section BDocument3 pagesF2 Mid-Year Exam Section BAnne Marian Anak JOSEPHNo ratings yet
- Claire Dahyot Fizelier Ceftriaxone To Prevent EarlyDocument11 pagesClaire Dahyot Fizelier Ceftriaxone To Prevent EarlyFermin LombardiaNo ratings yet
- Insulin PregnancyDocument23 pagesInsulin PregnancymytriciallorinNo ratings yet
- Microsoft Word - DS03 - Paper - 1.1Document8 pagesMicrosoft Word - DS03 - Paper - 1.1kuridisanjeevNo ratings yet
- AnaphylaxisDocument1 pageAnaphylaxisherdind prayogaNo ratings yet
- Ortho Final ExamDocument40 pagesOrtho Final ExamMariane GumbanNo ratings yet
- Superhero AssignmentDocument5 pagesSuperhero Assignmentprathibha asok kumarNo ratings yet
- Natural Homeopathic Medicine For Balanitis - Homeopathy atDocument7 pagesNatural Homeopathic Medicine For Balanitis - Homeopathy atDhandapani VNo ratings yet
- Health Ass.Document6 pagesHealth Ass.Rashmi Devrani VyasNo ratings yet
- Pointers To ReviewDocument18 pagesPointers To ReviewHegi Ann AlcalaNo ratings yet
- Oral Halitosis: Definitions: Breath Malodor, Defined As Foul or Offensive Odor of Expired Air, May BeDocument7 pagesOral Halitosis: Definitions: Breath Malodor, Defined As Foul or Offensive Odor of Expired Air, May BeSnowNo ratings yet
- Neck Trauma DR Hauwa Shitu 1Document40 pagesNeck Trauma DR Hauwa Shitu 1Hauwa shitu.B100% (1)
- Consensus Based Guidelines For The Recognition,.15Document13 pagesConsensus Based Guidelines For The Recognition,.15ms98alissaNo ratings yet
- Indicador Gabs AtualizadoDocument2 pagesIndicador Gabs AtualizadoBiXus Estrategas EmpresarialesNo ratings yet
- Breast Cancer Assessment ChartDocument2 pagesBreast Cancer Assessment ChartNigel Leigh Godfrey GutierrezNo ratings yet
- 1 s2.0 S2473952921007515 MainDocument10 pages1 s2.0 S2473952921007515 MainAndreea RacovitaNo ratings yet
- A Family Case Presentation, SLHDocument27 pagesA Family Case Presentation, SLHRajanNo ratings yet
- Diagnostic Diferential Medicina InternaDocument6 pagesDiagnostic Diferential Medicina InternaLary ArNo ratings yet