
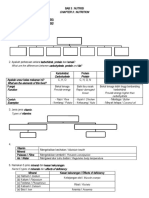
Menstrual Disorders
Menstrual Disorders
You might also like
- The No Fuss Bread Machine CookbookDocument509 pagesThe No Fuss Bread Machine CookbookMoraby Bandhoo WardaNo ratings yet
- Book Excerpt: 'The Secret Life of Fat'Document15 pagesBook Excerpt: 'The Secret Life of Fat'Here & NowNo ratings yet
- Menopause ExerciseDocument8 pagesMenopause ExerciseWittapong SinsoongsudNo ratings yet
- 15663-Article Text-39084-44869-10-20210811Document10 pages15663-Article Text-39084-44869-10-20210811deorivaldi89No ratings yet
- Anthropometric and Cardiovascular Responses To Hypertrophic Resistance Training in Postmenopausal WomenDocument6 pagesAnthropometric and Cardiovascular Responses To Hypertrophic Resistance Training in Postmenopausal WomenRosemary Mareco MartinsNo ratings yet
- A Guide To Fasting For MenopauseDocument12 pagesA Guide To Fasting For MenopauseConce RamirezNo ratings yet
- Comparison of High-Intensity IDocument17 pagesComparison of High-Intensity IIulian-Stefan HOLUBIACNo ratings yet
- Menopause and Exercise: Linking Pathophysiology To Effects: Imedpub JournalsDocument8 pagesMenopause and Exercise: Linking Pathophysiology To Effects: Imedpub Journalsد.موسى التويتيNo ratings yet
- Effects of An 8-Week Aerobic Dance Exercise Programme FinalDocument9 pagesEffects of An 8-Week Aerobic Dance Exercise Programme FinalNíí PereiraNo ratings yet
- Prevention and Treatment of Sarcopenia Obesity (2019)Document24 pagesPrevention and Treatment of Sarcopenia Obesity (2019)Brayam AguilarNo ratings yet
- Uma Comparação de Dieta Versus Programas de Dieta + Exercícios para Melhoria Da Saúde em Mulheres de Meia-Idade Com Sobrepeso - InglêsDocument23 pagesUma Comparação de Dieta Versus Programas de Dieta + Exercícios para Melhoria Da Saúde em Mulheres de Meia-Idade Com Sobrepeso - InglêsJuliana MontovaniNo ratings yet
- Effect of Aerobic Exercises On PrimaryDocument5 pagesEffect of Aerobic Exercises On PrimaryAkariakiraNo ratings yet
- Review Impact of The Menstrual Cycle On Determinants of Energy Balance: A Putative Role in Weight Loss AttemptsDocument9 pagesReview Impact of The Menstrual Cycle On Determinants of Energy Balance: A Putative Role in Weight Loss AttemptsJuan PalomoNo ratings yet
- Osteo 1Document6 pagesOsteo 1Ardhyan ArdhyanNo ratings yet
- 6 Year Changes in Body Composition in Women at Mid-Life Ovarian and Chronological AgingDocument15 pages6 Year Changes in Body Composition in Women at Mid-Life Ovarian and Chronological AgingConstanza MillánNo ratings yet
- Endometriosis and Physical ExercisesDocument5 pagesEndometriosis and Physical ExercisesPaula RangelNo ratings yet
- Sex Differences and Considerations For Female Specific Nutritional Strategies A Narrative ReviewDocument21 pagesSex Differences and Considerations For Female Specific Nutritional Strategies A Narrative Reviewapi-650977999No ratings yet
- Biol Sex Differ 2020 11 1 15Document10 pagesBiol Sex Differ 2020 11 1 15Fernando SousaNo ratings yet
- The Characteristics, Risks, Effects, and Pathophysiology of Eating Disorders - A Review of Anorexia Nervosa and Bulimia NervosaDocument9 pagesThe Characteristics, Risks, Effects, and Pathophysiology of Eating Disorders - A Review of Anorexia Nervosa and Bulimia NervosaIJRASETPublicationsNo ratings yet
- Annotated Bibliography RevisedDocument10 pagesAnnotated Bibliography Revisedapi-743811693No ratings yet
- Annotated Bibliography First DraftDocument9 pagesAnnotated Bibliography First Draftapi-743811693No ratings yet
- Goh - Excess Fat in The Abdomen - 2018Document6 pagesGoh - Excess Fat in The Abdomen - 2018MIRIAM VIDURRIZAGANo ratings yet
- Effectivenes of PA Interventions On Pregnancy Related Outcomes Among Pregnant Women Systematic Review 42 OldDocument42 pagesEffectivenes of PA Interventions On Pregnancy Related Outcomes Among Pregnant Women Systematic Review 42 OldAisleenHNo ratings yet
- Esmaeilinezhad Et Al 2019Document8 pagesEsmaeilinezhad Et Al 2019ahmad azhar marzuqiNo ratings yet
- 17 Eman EtalDocument8 pages17 Eman EtaleditorijmrhsNo ratings yet
- JBMR 3905Document10 pagesJBMR 3905Panagiotes KoutelidakesNo ratings yet
- Artigo - Vegetarianism and Menstrual Cycle Disturbances - Susan I BarrDocument6 pagesArtigo - Vegetarianism and Menstrual Cycle Disturbances - Susan I Barrlayla.oliveiraNo ratings yet
- Ayurvedic Management of Aartava Kshaya W.S.R. Polycystic Ovarian Syndrome - A Critical ReviewDocument14 pagesAyurvedic Management of Aartava Kshaya W.S.R. Polycystic Ovarian Syndrome - A Critical Reviewremya jNo ratings yet
- Marandi 2013Document9 pagesMarandi 2013Sam Steven Hernandez JañaNo ratings yet
- Bales2018-Obesity Interventions For Older Adults - Diet As A Determinant of Physical FunctionDocument9 pagesBales2018-Obesity Interventions For Older Adults - Diet As A Determinant of Physical FunctionJaiane TeixeiraNo ratings yet
- AF THDP SMDocument2 pagesAF THDP SMLussi Wahyu Putri UtamiNo ratings yet
- Dmso 10 513Document7 pagesDmso 10 513Kirana KlarismaNo ratings yet
- The Effects of Dietary Fasting On Physical Balance Among Healthy Young WomenDocument7 pagesThe Effects of Dietary Fasting On Physical Balance Among Healthy Young WomenNur Fitri Widya AstutiNo ratings yet
- InglesDocument6 pagesInglesKuroKy KrausserNo ratings yet
- Physical Activity During Pregnancy Past and Present: Miriam Katz, MDDocument5 pagesPhysical Activity During Pregnancy Past and Present: Miriam Katz, MDAnisNo ratings yet
- Chiu 2017Document9 pagesChiu 2017Sam Steven Hernandez JañaNo ratings yet
- BMC Complementary and Alternative MedicineDocument8 pagesBMC Complementary and Alternative MedicineThiago NunesNo ratings yet
- Diet and Exercise in The Management of Polycystic Ovary Syndrome - Practical Considerations For Person-Centered CareDocument11 pagesDiet and Exercise in The Management of Polycystic Ovary Syndrome - Practical Considerations For Person-Centered CareKatia Sosa VeraNo ratings yet
- Annotated Bibliography IfDocument10 pagesAnnotated Bibliography Ifapi-743811693No ratings yet
- The Effect of Omega-3 Supplementation On Androgen Profile and Menstrual Status in Women With PcosDocument8 pagesThe Effect of Omega-3 Supplementation On Androgen Profile and Menstrual Status in Women With PcosizbaasifNo ratings yet
- Ijerph 20 03991Document11 pagesIjerph 20 03991ravan aramamNo ratings yet
- Determination of Hand Grip Strength in PregnancyDocument13 pagesDetermination of Hand Grip Strength in PregnancyLawal Isa UsmanNo ratings yet
- NutrientsDocument34 pagesNutrientssilvanaNo ratings yet
- Mudanças Na Composição Corporal Com Dieta Hipocalórica Combinada Com Atividade Física Sedentária, Moderada e Intensa - Um Ensaio Clínico Randomizado - InglêsDocument21 pagesMudanças Na Composição Corporal Com Dieta Hipocalórica Combinada Com Atividade Física Sedentária, Moderada e Intensa - Um Ensaio Clínico Randomizado - InglêsJuliana MontovaniNo ratings yet
- JFMK 05 00035 v2Document24 pagesJFMK 05 00035 v2syakira00putriNo ratings yet
- Physical Exercise During Pregnancy A Systematic ReviewDocument10 pagesPhysical Exercise During Pregnancy A Systematic ReviewAisleenHNo ratings yet
- Zavorsky Longo 2011Document17 pagesZavorsky Longo 2011Heidy Bravo RamosNo ratings yet
- Art 256Document6 pagesArt 256IshikaNo ratings yet
- Senobi Breathing Exercise Vs Diafragma Breathing ExerciseDocument6 pagesSenobi Breathing Exercise Vs Diafragma Breathing ExerciseAndreas Paian SiahaanNo ratings yet
- 11 Iajps11102017 PDFDocument9 pages11 Iajps11102017 PDFBaru Chandrasekhar RaoNo ratings yet
- The Effects of Exercise On Pubertal Progression and Reproductive Function in GirlsDocument8 pagesThe Effects of Exercise On Pubertal Progression and Reproductive Function in GirlsNutricion Deportiva NutrainerNo ratings yet
- Novel Insights On Nutrient Management of Sarcopenia in ElderlyDocument15 pagesNovel Insights On Nutrient Management of Sarcopenia in ElderlyMario Ociel MoyaNo ratings yet
- Fritschi 2014 PDFDocument8 pagesFritschi 2014 PDFCinthiaDReisNo ratings yet
- Assessment of Body Fat Composition Parameters in Women of Polycystic Ovary Syndrome (Pcos) : A Case - Control StudyDocument7 pagesAssessment of Body Fat Composition Parameters in Women of Polycystic Ovary Syndrome (Pcos) : A Case - Control StudyIJAR JOURNALNo ratings yet
- Prevalence of Abdominal Obesity and Its Associated Comorbid Condition in Adult Yemeni People of Sana'a CityDocument8 pagesPrevalence of Abdominal Obesity and Its Associated Comorbid Condition in Adult Yemeni People of Sana'a CityMohamed BamashmoosNo ratings yet
- Physiological Aspects of Physical Exercise in WomenDocument5 pagesPhysiological Aspects of Physical Exercise in WomenScribdTranslationsNo ratings yet
- Muscle DysmorphiaDocument6 pagesMuscle DysmorphiaKarla RojasNo ratings yet
- IJTR Intermittent VS Continenous Exercises ObesityDocument5 pagesIJTR Intermittent VS Continenous Exercises ObesityMohamed Serag El-deinNo ratings yet
- Metabolic Risk Management, Physical Exercise and Lifestyle Counselling in Low-Active Adults: Controlled Randomized Trial (BELLUGAT)Document15 pagesMetabolic Risk Management, Physical Exercise and Lifestyle Counselling in Low-Active Adults: Controlled Randomized Trial (BELLUGAT)adrianNo ratings yet
- Resistance Training During Pregnancy Safe And.9Document9 pagesResistance Training During Pregnancy Safe And.9Luis Felipe SilioNo ratings yet
- The Secrets You Should Know About Sexual Medicine; Part One; Obesity and Sexual DysfunctionFrom EverandThe Secrets You Should Know About Sexual Medicine; Part One; Obesity and Sexual DysfunctionNo ratings yet
- Learning To Eat Intuitively: A Qualitative Exploration of The Experience of Mid-Age WomenDocument8 pagesLearning To Eat Intuitively: A Qualitative Exploration of The Experience of Mid-Age WomenYasmim CronembergerNo ratings yet
- Cue Card VocabularyDocument11 pagesCue Card Vocabularysubhasankari saravananNo ratings yet
- 7.Ch-13 Strategies For Enhancement in Food Production (178-195) FinalDocument18 pages7.Ch-13 Strategies For Enhancement in Food Production (178-195) FinalCHAKRI BABLUNo ratings yet
- The Alpine Secret For Healthy Weight Loss at HomeDocument14 pagesThe Alpine Secret For Healthy Weight Loss at HomeAmnwdNo ratings yet
- Classes of Food Carbohydrate Protein Fat Vitamin Mineral Fibre WaterDocument6 pagesClasses of Food Carbohydrate Protein Fat Vitamin Mineral Fibre WaterNoor FadzleezaNo ratings yet
- Chapter 1Document13 pagesChapter 1sangguniangkabataanngbrgywawaNo ratings yet
- TAURINE The Key To Restoring Metabolic Function - Ray Peat ForumDocument12 pagesTAURINE The Key To Restoring Metabolic Function - Ray Peat ForumDarci HallNo ratings yet
- Group 3: Menu Planning and Budget Proposal For The Whole ActivityDocument2 pagesGroup 3: Menu Planning and Budget Proposal For The Whole ActivityGadz JamesNo ratings yet
- Tugas Odl B Ing RayDocument11 pagesTugas Odl B Ing RayRayhan GantengNo ratings yet
- Chapter 1. Sources of FoodDocument10 pagesChapter 1. Sources of FoodCHANDRA DEYNo ratings yet
- Skipping Breakfast Introduction 1 2 2Document39 pagesSkipping Breakfast Introduction 1 2 2Adrian PanlicanNo ratings yet
- BOOKLET 4th - 2024Document88 pagesBOOKLET 4th - 2024marielapriscoNo ratings yet
- PB2 X Maths (041) 2022-2023Document5 pagesPB2 X Maths (041) 2022-2023Shradha Arora 8th ANo ratings yet
- Instantpot NEWDocument1 pageInstantpot NEWSuzana CrăciunNo ratings yet
- 04 Passive VoiceDocument35 pages04 Passive VoiceMehak SrivastavaNo ratings yet
- Health History: Print Your Answers. Please Print ClearlyDocument4 pagesHealth History: Print Your Answers. Please Print Clearlymarwan el deebNo ratings yet
- The Best Damn Cardio For Natural Lifters - T NationDocument11 pagesThe Best Damn Cardio For Natural Lifters - T Nationbmonat92No ratings yet
- Calf Feeding and ManagementDocument24 pagesCalf Feeding and Managementthanh ba matNo ratings yet
- Task 4 3Document3 pagesTask 4 3aleqsandrepingpongNo ratings yet
- ENGWORKfinals BUSINESS PLANDocument15 pagesENGWORKfinals BUSINESS PLANOcubillo Froilan D.No ratings yet
- Anghelys ContrerasDocument2 pagesAnghelys ContrerasAnghelys ContrerasNo ratings yet
- Awareness of The Amount of Water Intake Among College StudentsDocument20 pagesAwareness of The Amount of Water Intake Among College StudentsLan Anh NguyenNo ratings yet
- Durmaz, Keser, Tuncer 2022 PDFDocument10 pagesDurmaz, Keser, Tuncer 2022 PDFelioraNo ratings yet
- Price List AllDocument20 pagesPrice List Allaj salazarNo ratings yet
- Checklist of Experiment SPMDocument2 pagesChecklist of Experiment SPMAqil SeokjinieNo ratings yet
- N036 NSTP Narrative Report Magpantay Melanie S.Document10 pagesN036 NSTP Narrative Report Magpantay Melanie S.Bianca Marithè RejanoNo ratings yet
- Experiment of Vitamin: ProcedureDocument3 pagesExperiment of Vitamin: ProcedureMicah Joy MacalaladNo ratings yet
- BNF PDF - 10828 - 20201123125107161Document23 pagesBNF PDF - 10828 - 20201123125107161Ausi PalsuNo ratings yet
























































































Download as pdf or txt
You might also like
- The No Fuss Bread Machine CookbookDocument509 pagesThe No Fuss Bread Machine CookbookMoraby Bandhoo WardaNo ratings yet
- Book Excerpt: 'The Secret Life of Fat'Document15 pagesBook Excerpt: 'The Secret Life of Fat'Here & NowNo ratings yet
- Menopause ExerciseDocument8 pagesMenopause ExerciseWittapong SinsoongsudNo ratings yet
- 15663-Article Text-39084-44869-10-20210811Document10 pages15663-Article Text-39084-44869-10-20210811deorivaldi89No ratings yet
- Anthropometric and Cardiovascular Responses To Hypertrophic Resistance Training in Postmenopausal WomenDocument6 pagesAnthropometric and Cardiovascular Responses To Hypertrophic Resistance Training in Postmenopausal WomenRosemary Mareco MartinsNo ratings yet
- A Guide To Fasting For MenopauseDocument12 pagesA Guide To Fasting For MenopauseConce RamirezNo ratings yet
- Comparison of High-Intensity IDocument17 pagesComparison of High-Intensity IIulian-Stefan HOLUBIACNo ratings yet
- Menopause and Exercise: Linking Pathophysiology To Effects: Imedpub JournalsDocument8 pagesMenopause and Exercise: Linking Pathophysiology To Effects: Imedpub Journalsد.موسى التويتيNo ratings yet
- Effects of An 8-Week Aerobic Dance Exercise Programme FinalDocument9 pagesEffects of An 8-Week Aerobic Dance Exercise Programme FinalNíí PereiraNo ratings yet
- Prevention and Treatment of Sarcopenia Obesity (2019)Document24 pagesPrevention and Treatment of Sarcopenia Obesity (2019)Brayam AguilarNo ratings yet
- Uma Comparação de Dieta Versus Programas de Dieta + Exercícios para Melhoria Da Saúde em Mulheres de Meia-Idade Com Sobrepeso - InglêsDocument23 pagesUma Comparação de Dieta Versus Programas de Dieta + Exercícios para Melhoria Da Saúde em Mulheres de Meia-Idade Com Sobrepeso - InglêsJuliana MontovaniNo ratings yet
- Effect of Aerobic Exercises On PrimaryDocument5 pagesEffect of Aerobic Exercises On PrimaryAkariakiraNo ratings yet
- Review Impact of The Menstrual Cycle On Determinants of Energy Balance: A Putative Role in Weight Loss AttemptsDocument9 pagesReview Impact of The Menstrual Cycle On Determinants of Energy Balance: A Putative Role in Weight Loss AttemptsJuan PalomoNo ratings yet
- Osteo 1Document6 pagesOsteo 1Ardhyan ArdhyanNo ratings yet
- 6 Year Changes in Body Composition in Women at Mid-Life Ovarian and Chronological AgingDocument15 pages6 Year Changes in Body Composition in Women at Mid-Life Ovarian and Chronological AgingConstanza MillánNo ratings yet
- Endometriosis and Physical ExercisesDocument5 pagesEndometriosis and Physical ExercisesPaula RangelNo ratings yet
- Sex Differences and Considerations For Female Specific Nutritional Strategies A Narrative ReviewDocument21 pagesSex Differences and Considerations For Female Specific Nutritional Strategies A Narrative Reviewapi-650977999No ratings yet
- Biol Sex Differ 2020 11 1 15Document10 pagesBiol Sex Differ 2020 11 1 15Fernando SousaNo ratings yet
- The Characteristics, Risks, Effects, and Pathophysiology of Eating Disorders - A Review of Anorexia Nervosa and Bulimia NervosaDocument9 pagesThe Characteristics, Risks, Effects, and Pathophysiology of Eating Disorders - A Review of Anorexia Nervosa and Bulimia NervosaIJRASETPublicationsNo ratings yet
- Annotated Bibliography RevisedDocument10 pagesAnnotated Bibliography Revisedapi-743811693No ratings yet
- Annotated Bibliography First DraftDocument9 pagesAnnotated Bibliography First Draftapi-743811693No ratings yet
- Goh - Excess Fat in The Abdomen - 2018Document6 pagesGoh - Excess Fat in The Abdomen - 2018MIRIAM VIDURRIZAGANo ratings yet
- Effectivenes of PA Interventions On Pregnancy Related Outcomes Among Pregnant Women Systematic Review 42 OldDocument42 pagesEffectivenes of PA Interventions On Pregnancy Related Outcomes Among Pregnant Women Systematic Review 42 OldAisleenHNo ratings yet
- Esmaeilinezhad Et Al 2019Document8 pagesEsmaeilinezhad Et Al 2019ahmad azhar marzuqiNo ratings yet
- 17 Eman EtalDocument8 pages17 Eman EtaleditorijmrhsNo ratings yet
- JBMR 3905Document10 pagesJBMR 3905Panagiotes KoutelidakesNo ratings yet
- Artigo - Vegetarianism and Menstrual Cycle Disturbances - Susan I BarrDocument6 pagesArtigo - Vegetarianism and Menstrual Cycle Disturbances - Susan I Barrlayla.oliveiraNo ratings yet
- Ayurvedic Management of Aartava Kshaya W.S.R. Polycystic Ovarian Syndrome - A Critical ReviewDocument14 pagesAyurvedic Management of Aartava Kshaya W.S.R. Polycystic Ovarian Syndrome - A Critical Reviewremya jNo ratings yet
- Marandi 2013Document9 pagesMarandi 2013Sam Steven Hernandez JañaNo ratings yet
- Bales2018-Obesity Interventions For Older Adults - Diet As A Determinant of Physical FunctionDocument9 pagesBales2018-Obesity Interventions For Older Adults - Diet As A Determinant of Physical FunctionJaiane TeixeiraNo ratings yet
- AF THDP SMDocument2 pagesAF THDP SMLussi Wahyu Putri UtamiNo ratings yet
- Dmso 10 513Document7 pagesDmso 10 513Kirana KlarismaNo ratings yet
- The Effects of Dietary Fasting On Physical Balance Among Healthy Young WomenDocument7 pagesThe Effects of Dietary Fasting On Physical Balance Among Healthy Young WomenNur Fitri Widya AstutiNo ratings yet
- InglesDocument6 pagesInglesKuroKy KrausserNo ratings yet
- Physical Activity During Pregnancy Past and Present: Miriam Katz, MDDocument5 pagesPhysical Activity During Pregnancy Past and Present: Miriam Katz, MDAnisNo ratings yet
- Chiu 2017Document9 pagesChiu 2017Sam Steven Hernandez JañaNo ratings yet
- BMC Complementary and Alternative MedicineDocument8 pagesBMC Complementary and Alternative MedicineThiago NunesNo ratings yet
- Diet and Exercise in The Management of Polycystic Ovary Syndrome - Practical Considerations For Person-Centered CareDocument11 pagesDiet and Exercise in The Management of Polycystic Ovary Syndrome - Practical Considerations For Person-Centered CareKatia Sosa VeraNo ratings yet
- Annotated Bibliography IfDocument10 pagesAnnotated Bibliography Ifapi-743811693No ratings yet
- The Effect of Omega-3 Supplementation On Androgen Profile and Menstrual Status in Women With PcosDocument8 pagesThe Effect of Omega-3 Supplementation On Androgen Profile and Menstrual Status in Women With PcosizbaasifNo ratings yet
- Ijerph 20 03991Document11 pagesIjerph 20 03991ravan aramamNo ratings yet
- Determination of Hand Grip Strength in PregnancyDocument13 pagesDetermination of Hand Grip Strength in PregnancyLawal Isa UsmanNo ratings yet
- NutrientsDocument34 pagesNutrientssilvanaNo ratings yet
- Mudanças Na Composição Corporal Com Dieta Hipocalórica Combinada Com Atividade Física Sedentária, Moderada e Intensa - Um Ensaio Clínico Randomizado - InglêsDocument21 pagesMudanças Na Composição Corporal Com Dieta Hipocalórica Combinada Com Atividade Física Sedentária, Moderada e Intensa - Um Ensaio Clínico Randomizado - InglêsJuliana MontovaniNo ratings yet
- JFMK 05 00035 v2Document24 pagesJFMK 05 00035 v2syakira00putriNo ratings yet
- Physical Exercise During Pregnancy A Systematic ReviewDocument10 pagesPhysical Exercise During Pregnancy A Systematic ReviewAisleenHNo ratings yet
- Zavorsky Longo 2011Document17 pagesZavorsky Longo 2011Heidy Bravo RamosNo ratings yet
- Art 256Document6 pagesArt 256IshikaNo ratings yet
- Senobi Breathing Exercise Vs Diafragma Breathing ExerciseDocument6 pagesSenobi Breathing Exercise Vs Diafragma Breathing ExerciseAndreas Paian SiahaanNo ratings yet
- 11 Iajps11102017 PDFDocument9 pages11 Iajps11102017 PDFBaru Chandrasekhar RaoNo ratings yet
- The Effects of Exercise On Pubertal Progression and Reproductive Function in GirlsDocument8 pagesThe Effects of Exercise On Pubertal Progression and Reproductive Function in GirlsNutricion Deportiva NutrainerNo ratings yet
- Novel Insights On Nutrient Management of Sarcopenia in ElderlyDocument15 pagesNovel Insights On Nutrient Management of Sarcopenia in ElderlyMario Ociel MoyaNo ratings yet
- Fritschi 2014 PDFDocument8 pagesFritschi 2014 PDFCinthiaDReisNo ratings yet
- Assessment of Body Fat Composition Parameters in Women of Polycystic Ovary Syndrome (Pcos) : A Case - Control StudyDocument7 pagesAssessment of Body Fat Composition Parameters in Women of Polycystic Ovary Syndrome (Pcos) : A Case - Control StudyIJAR JOURNALNo ratings yet
- Prevalence of Abdominal Obesity and Its Associated Comorbid Condition in Adult Yemeni People of Sana'a CityDocument8 pagesPrevalence of Abdominal Obesity and Its Associated Comorbid Condition in Adult Yemeni People of Sana'a CityMohamed BamashmoosNo ratings yet
- Physiological Aspects of Physical Exercise in WomenDocument5 pagesPhysiological Aspects of Physical Exercise in WomenScribdTranslationsNo ratings yet
- Muscle DysmorphiaDocument6 pagesMuscle DysmorphiaKarla RojasNo ratings yet
- IJTR Intermittent VS Continenous Exercises ObesityDocument5 pagesIJTR Intermittent VS Continenous Exercises ObesityMohamed Serag El-deinNo ratings yet
- Metabolic Risk Management, Physical Exercise and Lifestyle Counselling in Low-Active Adults: Controlled Randomized Trial (BELLUGAT)Document15 pagesMetabolic Risk Management, Physical Exercise and Lifestyle Counselling in Low-Active Adults: Controlled Randomized Trial (BELLUGAT)adrianNo ratings yet
- Resistance Training During Pregnancy Safe And.9Document9 pagesResistance Training During Pregnancy Safe And.9Luis Felipe SilioNo ratings yet
- The Secrets You Should Know About Sexual Medicine; Part One; Obesity and Sexual DysfunctionFrom EverandThe Secrets You Should Know About Sexual Medicine; Part One; Obesity and Sexual DysfunctionNo ratings yet
- Learning To Eat Intuitively: A Qualitative Exploration of The Experience of Mid-Age WomenDocument8 pagesLearning To Eat Intuitively: A Qualitative Exploration of The Experience of Mid-Age WomenYasmim CronembergerNo ratings yet
- Cue Card VocabularyDocument11 pagesCue Card Vocabularysubhasankari saravananNo ratings yet
- 7.Ch-13 Strategies For Enhancement in Food Production (178-195) FinalDocument18 pages7.Ch-13 Strategies For Enhancement in Food Production (178-195) FinalCHAKRI BABLUNo ratings yet
- The Alpine Secret For Healthy Weight Loss at HomeDocument14 pagesThe Alpine Secret For Healthy Weight Loss at HomeAmnwdNo ratings yet
- Classes of Food Carbohydrate Protein Fat Vitamin Mineral Fibre WaterDocument6 pagesClasses of Food Carbohydrate Protein Fat Vitamin Mineral Fibre WaterNoor FadzleezaNo ratings yet
- Chapter 1Document13 pagesChapter 1sangguniangkabataanngbrgywawaNo ratings yet
- TAURINE The Key To Restoring Metabolic Function - Ray Peat ForumDocument12 pagesTAURINE The Key To Restoring Metabolic Function - Ray Peat ForumDarci HallNo ratings yet
- Group 3: Menu Planning and Budget Proposal For The Whole ActivityDocument2 pagesGroup 3: Menu Planning and Budget Proposal For The Whole ActivityGadz JamesNo ratings yet
- Tugas Odl B Ing RayDocument11 pagesTugas Odl B Ing RayRayhan GantengNo ratings yet
- Chapter 1. Sources of FoodDocument10 pagesChapter 1. Sources of FoodCHANDRA DEYNo ratings yet
- Skipping Breakfast Introduction 1 2 2Document39 pagesSkipping Breakfast Introduction 1 2 2Adrian PanlicanNo ratings yet
- BOOKLET 4th - 2024Document88 pagesBOOKLET 4th - 2024marielapriscoNo ratings yet
- PB2 X Maths (041) 2022-2023Document5 pagesPB2 X Maths (041) 2022-2023Shradha Arora 8th ANo ratings yet
- Instantpot NEWDocument1 pageInstantpot NEWSuzana CrăciunNo ratings yet
- 04 Passive VoiceDocument35 pages04 Passive VoiceMehak SrivastavaNo ratings yet
- Health History: Print Your Answers. Please Print ClearlyDocument4 pagesHealth History: Print Your Answers. Please Print Clearlymarwan el deebNo ratings yet
- The Best Damn Cardio For Natural Lifters - T NationDocument11 pagesThe Best Damn Cardio For Natural Lifters - T Nationbmonat92No ratings yet
- Calf Feeding and ManagementDocument24 pagesCalf Feeding and Managementthanh ba matNo ratings yet
- Task 4 3Document3 pagesTask 4 3aleqsandrepingpongNo ratings yet
- ENGWORKfinals BUSINESS PLANDocument15 pagesENGWORKfinals BUSINESS PLANOcubillo Froilan D.No ratings yet
- Anghelys ContrerasDocument2 pagesAnghelys ContrerasAnghelys ContrerasNo ratings yet
- Awareness of The Amount of Water Intake Among College StudentsDocument20 pagesAwareness of The Amount of Water Intake Among College StudentsLan Anh NguyenNo ratings yet
- Durmaz, Keser, Tuncer 2022 PDFDocument10 pagesDurmaz, Keser, Tuncer 2022 PDFelioraNo ratings yet
- Price List AllDocument20 pagesPrice List Allaj salazarNo ratings yet
- Checklist of Experiment SPMDocument2 pagesChecklist of Experiment SPMAqil SeokjinieNo ratings yet
- N036 NSTP Narrative Report Magpantay Melanie S.Document10 pagesN036 NSTP Narrative Report Magpantay Melanie S.Bianca Marithè RejanoNo ratings yet
- Experiment of Vitamin: ProcedureDocument3 pagesExperiment of Vitamin: ProcedureMicah Joy MacalaladNo ratings yet
- BNF PDF - 10828 - 20201123125107161Document23 pagesBNF PDF - 10828 - 20201123125107161Ausi PalsuNo ratings yet