Download as docx, pdf, or txt
You might also like
- Homoeopathic Drug Pictures - Margaret L TylerDocument1,042 pagesHomoeopathic Drug Pictures - Margaret L Tyleramishcar100% (11)
- TEST 1, Health Assessment Practice QuestionsDocument35 pagesTEST 1, Health Assessment Practice QuestionsMike75% (12)
- Development of Frog EmbryoDocument13 pagesDevelopment of Frog EmbryoNexieNo ratings yet
- Ex4.2 Development of Frog EmbryoDocument14 pagesEx4.2 Development of Frog EmbryoNexie100% (1)
- Speech Pathology TableDocument9 pagesSpeech Pathology TableMartinez_DO100% (7)
- 5 6082340175571059112Document5 pages5 6082340175571059112Inukaicchi TakumichiNo ratings yet
- Case Study CopdDocument7 pagesCase Study CopdIrveen Joy RamirezNo ratings yet
- Acls MegacodeDocument8 pagesAcls MegacodeRachel PerandoNo ratings yet
- Frog AtlasDocument16 pagesFrog AtlasJAYHANNE PSYCHE MONDIANo ratings yet
- Development of Frog EmbryoDocument13 pagesDevelopment of Frog EmbryoCHRISTIAN LOYD ARUPENo ratings yet
- Spinal Cord TransectionDocument2 pagesSpinal Cord TransectionIsak ShatikaNo ratings yet
- CN Summary FinalDocument2 pagesCN Summary FinalNur NajminaNo ratings yet
- Ferraris Ana213 Week4labsheetDocument32 pagesFerraris Ana213 Week4labsheetZoe FormosoNo ratings yet
- Classification of Velopharyngeal DysfunctionDocument1 pageClassification of Velopharyngeal DysfunctionVictoria Rojas AlvearNo ratings yet
- Anatomy of The Thyroid GlandDocument5 pagesAnatomy of The Thyroid GlandShienna Marie SalvioNo ratings yet
- Cerebral Cortex Cerebral CortexDocument62 pagesCerebral Cortex Cerebral CortexMORGAN LAMBERTNo ratings yet
- Lec 03 - Assessing of Neurological System and Special SensesDocument7 pagesLec 03 - Assessing of Neurological System and Special SensesIRISH MANIAGONo ratings yet
- Otic Ganglion: Schema: Plate 145Document8 pagesOtic Ganglion: Schema: Plate 145Andreea LăzăroiuNo ratings yet
- Anatomy of Facial NerveDocument32 pagesAnatomy of Facial NerveDr. Fatema HajiNo ratings yet
- Facial IsDocument3 pagesFacial IsSrdjan SekularacNo ratings yet
- Brain Seara Bisadicek: Basic Some AlDocument5 pagesBrain Seara Bisadicek: Basic Some AlGarry SoloanNo ratings yet
- Cerebral Cortex Cerebral CortexDocument62 pagesCerebral Cortex Cerebral CortexJ NNo ratings yet
- NeuroscienceDocument5 pagesNeuroscienceChing MacarubboNo ratings yet
- Board Review Blood SupplyDocument6 pagesBoard Review Blood Supplynewguy927No ratings yet
- Color Atlas of BrainDocument8 pagesColor Atlas of BrainMWNo ratings yet
- 14 - NS7 SC Motor Pathways All Sites (Handout) F2022 (Exported)Document25 pages14 - NS7 SC Motor Pathways All Sites (Handout) F2022 (Exported)Lucky NguyenNo ratings yet
- Traumatic Brain Injuries Study GuideDocument18 pagesTraumatic Brain Injuries Study GuideCarl Elexer Cuyugan Ano100% (1)
- EJD Physical Assessment Head To ToeDocument4 pagesEJD Physical Assessment Head To ToeErl DrizNo ratings yet
- Ent Practical (1) - 1Document63 pagesEnt Practical (1) - 1iamvipadityaNo ratings yet
- 09:16 - Back & Spinal Cord PDFDocument24 pages09:16 - Back & Spinal Cord PDFVidya BalaNo ratings yet
- Mandibular NerveDocument1 pageMandibular NerveEileen ChiongNo ratings yet
- Medical TermsDocument1 pageMedical Termsj.y.zhang95No ratings yet
- Aphasia ChartDocument2 pagesAphasia ChartSidra JavedNo ratings yet
- Aphasias: The Koriesh's Extract in Neurological ArtsDocument1 pageAphasias: The Koriesh's Extract in Neurological ArtsDaniela N AnghelNo ratings yet
- Sense OrgansDocument3 pagesSense OrgansAabhaNo ratings yet
- Neuro 1.27.22Document19 pagesNeuro 1.27.22Vhince PiscoNo ratings yet
- Brain Lobes & FunctionsDocument15 pagesBrain Lobes & FunctionsAlyssa PangNo ratings yet
- Page of 1 3 Carotid Arteries L2 Vascular Biology: Musculofascial CollarDocument3 pagesPage of 1 3 Carotid Arteries L2 Vascular Biology: Musculofascial CollarFazreena EleenaNo ratings yet
- 3 Ways To Examine The Larynx: PiriformDocument10 pages3 Ways To Examine The Larynx: PiriformbeautyNo ratings yet
- True Oral CavityDocument3 pagesTrue Oral CavityHanneke Du PlessisNo ratings yet
- Neurorehabilitation 1Document439 pagesNeurorehabilitation 1Duncan D'AmicoNo ratings yet
- Lecture 8Document16 pagesLecture 8Farah YusoffNo ratings yet
- Anatomy PDFDocument29 pagesAnatomy PDFJoydee Liza MarcoNo ratings yet
- Auditory PathwayDocument12 pagesAuditory PathwayEvans chamaNo ratings yet
- Neurological Examination in Spinal Cord Injury NewDocument18 pagesNeurological Examination in Spinal Cord Injury NewPratyush RanjanNo ratings yet
- Table 1. General Somatic Sensory: Tracts Stimulus Function N1 N2 Decussation N3 N4 Additional InfoDocument8 pagesTable 1. General Somatic Sensory: Tracts Stimulus Function N1 N2 Decussation N3 N4 Additional InfoNicole Villaflor FabicoNo ratings yet
- Lecture 11Document5 pagesLecture 11bibifamelaganieNo ratings yet
- Macleod - S - Clinical - Examination - 15th NeuroDocument18 pagesMacleod - S - Clinical - Examination - 15th Neurowxyngtc4n9No ratings yet
- NeuroanatomyDocument72 pagesNeuroanatomyYasar SabirNo ratings yet
- Stroke Syndromes: Hemiparesis (Faciobrachiocrural Weakness)Document7 pagesStroke Syndromes: Hemiparesis (Faciobrachiocrural Weakness)eko aNo ratings yet
- Cap 17 Raices Sist Nervioso y CondcutaDocument2 pagesCap 17 Raices Sist Nervioso y CondcutaSandra OrtizNo ratings yet
- Maxillary nerveDocument1 pageMaxillary nerveEileen ChiongNo ratings yet
- Neurologic SystemDocument6 pagesNeurologic SystemNadia AbdurasidNo ratings yet
- HNF - Parasympathetic GangliaDocument15 pagesHNF - Parasympathetic GangliaSridevi KNo ratings yet
- ZOOLOGYDocument3 pagesZOOLOGYJackelyn SalazarNo ratings yet
- Radiographs Upper LimbDocument7 pagesRadiographs Upper LimbXandws -IOS tips and trick and gamingNo ratings yet
- 3 CNS PDFDocument42 pages3 CNS PDFPutriNo ratings yet
- Modul Neurobehavior RevisiDocument54 pagesModul Neurobehavior RevisiSeno TanubrataNo ratings yet
- DR Agus Sistem Syaraf Spinal ChordDocument50 pagesDR Agus Sistem Syaraf Spinal ChordRifky Al ThariqNo ratings yet
- Head and NeckDocument208 pagesHead and NeckStephanie ThompsonNo ratings yet
- Spinal CordDocument82 pagesSpinal CordAfifah Nur KartikasariNo ratings yet
- Cranial Nerve V2 - Maxillary Nerve - FRCEM SuccessDocument1 pageCranial Nerve V2 - Maxillary Nerve - FRCEM SuccessJohn CoxNo ratings yet
- 1.13.2 Clinical Localization and History in NeurologyDocument42 pages1.13.2 Clinical Localization and History in Neurologyfikrah sharifNo ratings yet
- Differential Diagnosis DysarthriaDocument1 pageDifferential Diagnosis DysarthriaShruti KumarNo ratings yet
- Conduction of HeartDocument21 pagesConduction of Heartangelsundar22100% (1)
- Manage MENOPAUSIA 2020Document299 pagesManage MENOPAUSIA 2020Griselda Pérez Alcántara100% (2)
- Spinal Cord InjuryDocument37 pagesSpinal Cord InjuryMrmonstrosityNo ratings yet
- Pure Biology Chapter 7 Nutrition in PlantsDocument38 pagesPure Biology Chapter 7 Nutrition in Plantshamsterish100% (2)
- NS. Morph. CompoundingDocument22 pagesNS. Morph. CompoundingReqistaAndiniNo ratings yet
- Christina Vong 24244058 - Psychophysics of Vision in Medical Imaging EssayDocument12 pagesChristina Vong 24244058 - Psychophysics of Vision in Medical Imaging EssayChristina VongNo ratings yet
- Basic ScienceDocument2 pagesBasic ScienceMurjanatu Saidu TiggiNo ratings yet
- Experiment 4 ReportDocument25 pagesExperiment 4 ReportFeroze Nizome67% (6)
- Dietary Fruit SbaDocument2 pagesDietary Fruit SbaannmarieNo ratings yet
- Factors Affecting Enzyme ActivityDocument3 pagesFactors Affecting Enzyme ActivityEmi JiHyeon Kim0% (1)
- TNCT Q4 Module5Document22 pagesTNCT Q4 Module5Glenn Mendez100% (1)
- Nervous System Lab WorksheetDocument3 pagesNervous System Lab WorksheetLMNTerriNo ratings yet
- Comparing The Effects of Music and Exercise With Music For Older Adults With InsomniaDocument7 pagesComparing The Effects of Music and Exercise With Music For Older Adults With InsomniaConsuelo VelandiaNo ratings yet
- MultraumaDocument9 pagesMultraumaDaniel Andres ForeroNo ratings yet
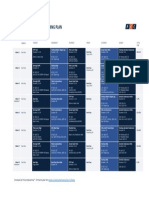
- 8 Weeks Gran Fondo OverivewDocument1 page8 Weeks Gran Fondo OverivewBorkoArsovicNo ratings yet
- Mark Scheme Transport QuestionsDocument3 pagesMark Scheme Transport QuestionsJohn OsborneNo ratings yet
- Concept Map On CVA Bleed Left Thalamo-Ganglionic Bleed Patient Name: Mr. DGDDocument1 pageConcept Map On CVA Bleed Left Thalamo-Ganglionic Bleed Patient Name: Mr. DGDBert Brian Bolido100% (1)
- Exercise 10 13Document5 pagesExercise 10 13Virlin Rose MahinayNo ratings yet
- PheromonesDocument6 pagesPheromoneskailas ambadiNo ratings yet
- Botany 2012-13 PDFDocument78 pagesBotany 2012-13 PDFNurul HaqueNo ratings yet
- Nicar PDFDocument8 pagesNicar PDFkevinNo ratings yet
- Osmosis High-Yield Physiology - Medicalstudyzone - Com (Sürüklenen)Document87 pagesOsmosis High-Yield Physiology - Medicalstudyzone - Com (Sürüklenen)Dilay MercimekNo ratings yet
- Prokaryotes and Eukaryote Venn DiagramDocument1 pageProkaryotes and Eukaryote Venn DiagramZanaia Dorothy G. DuterteNo ratings yet
- Visual Dysfunction in DiabetesDocument395 pagesVisual Dysfunction in DiabetesSergioAcuñaNo ratings yet
- Enriquez Physio Ex3-Act 3Document7 pagesEnriquez Physio Ex3-Act 3Vergel Jigs EnriquezNo ratings yet