Download as pdf or txt
You might also like
- Fixed Prosthesis With Vertical Margin Closure - Ezio Bruna PDFDocument243 pagesFixed Prosthesis With Vertical Margin Closure - Ezio Bruna PDFLorin Columb100% (1)
- Example 1: Dolphin Therapy?: Homework #1 Statistical Concepts Bio/Btec180 Biostatistics Miracosta CollegeDocument2 pagesExample 1: Dolphin Therapy?: Homework #1 Statistical Concepts Bio/Btec180 Biostatistics Miracosta Collegeeasttr090No ratings yet
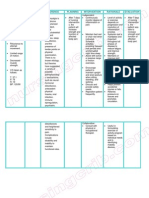
- Nursing Care Plan FibromyalgiaDocument2 pagesNursing Care Plan Fibromyalgiaderic90% (10)
- Biological - Psychiatry. (2.vols) H D Haenen - Et.al. (Wiley.2002) PDFDocument1,468 pagesBiological - Psychiatry. (2.vols) H D Haenen - Et.al. (Wiley.2002) PDFalexandra100% (1)
- Stretching OldDocument5 pagesStretching OldGin CruzNo ratings yet
- Dmmc-Ihs: College of Physical TherapyDocument2 pagesDmmc-Ihs: College of Physical TherapyHannah JavinaNo ratings yet
- Techniques Utilized in Rehabilitation: MobilizationDocument3 pagesTechniques Utilized in Rehabilitation: MobilizationAditya RanjanNo ratings yet
- Stretching For Impaired Mobility: by Ms Erum NazDocument60 pagesStretching For Impaired Mobility: by Ms Erum NazFareha KhanNo ratings yet
- Passive MovementsDocument17 pagesPassive MovementsRoshan rajNo ratings yet
- Procedures For Applying Passive Joint TechniquesDocument29 pagesProcedures For Applying Passive Joint TechniquessamNo ratings yet
- Streching 1Document35 pagesStreching 1SHUMAILA MALIKNo ratings yet
- Mobility Joint and FlexibilityDocument165 pagesMobility Joint and Flexibilityjose alberto100% (1)
- cp1 Week 7 TutorialDocument4 pagescp1 Week 7 Tutorialapi-508474347No ratings yet
- M1 Introduction To Manual TherapyDocument101 pagesM1 Introduction To Manual TherapySylvia LoongNo ratings yet
- Peripheral Joint Mobilization: Dr. Farwah PTDocument20 pagesPeripheral Joint Mobilization: Dr. Farwah PTsamNo ratings yet
- 2 Passive MovementDocument21 pages2 Passive Movementsuderson100% (2)
- Rehabilitation Guidelines Following Compartment Syndrome Release With Open FasciotomyDocument10 pagesRehabilitation Guidelines Following Compartment Syndrome Release With Open FasciotomyFaridatul IsniyahNo ratings yet
- Joint Mobilization What Is Joint Mobilization?Document6 pagesJoint Mobilization What Is Joint Mobilization?taravindnagarajNo ratings yet
- Mobility and Flexibility TrainingDocument52 pagesMobility and Flexibility TrainingMUGISHA GratienNo ratings yet
- Strain Counterstrain Devine - ClinicalSCSSAAODocument88 pagesStrain Counterstrain Devine - ClinicalSCSSAAOpnogrlNo ratings yet
- Kelompok 3: Stretching ExerciseDocument46 pagesKelompok 3: Stretching ExerciseGildarts KunNo ratings yet
- 5) Stretching For Impaired Mobility Part 1Document44 pages5) Stretching For Impaired Mobility Part 1Khushboo IkramNo ratings yet
- Stretching II: Drs. Adnan Wshah & Zaid ModhiDocument14 pagesStretching II: Drs. Adnan Wshah & Zaid ModhiIbraheem MohdNo ratings yet
- Stretching II: Drs. Adnan Wshah & Zaid ModhiDocument14 pagesStretching II: Drs. Adnan Wshah & Zaid ModhiIbraheem MohdNo ratings yet
- Terapi Manipulasi - Rahmi SesariaDocument47 pagesTerapi Manipulasi - Rahmi SesariaNQorianaNo ratings yet
- Passivemovements 171113053327Document18 pagesPassivemovements 171113053327vidyasagar pagillaNo ratings yet
- TractionDocument6 pagesTractiondrhemang100% (1)
- Dr. T.Sunilkumar MPT Assistant Professor SiprDocument16 pagesDr. T.Sunilkumar MPT Assistant Professor Siprvidyasagar pagillaNo ratings yet
- 4-Stretching For Impaired Mobility ADocument47 pages4-Stretching For Impaired Mobility Aphysical therapy channel ptNo ratings yet
- Stretching for-WPS OfficeDocument25 pagesStretching for-WPS OfficeMs. IshaNo ratings yet
- PNFDocument51 pagesPNFMuhamad Hakimi75% (4)
- Is Basic Technique Used For The Examination of Movement and For Initiating Movement Into A Program of Therapeutic InterventionDocument9 pagesIs Basic Technique Used For The Examination of Movement and For Initiating Movement Into A Program of Therapeutic InterventionEric Carlos YumulNo ratings yet
- Facilitatory & Inhibitory Tech PDFDocument59 pagesFacilitatory & Inhibitory Tech PDFShree PatelNo ratings yet
- Body Mechanics: The Importance of Joint MobilizationDocument11 pagesBody Mechanics: The Importance of Joint MobilizationtokionasNo ratings yet
- Rood Approach: Ot Ead 322: Traditional Sensorimotor ApproachesDocument3 pagesRood Approach: Ot Ead 322: Traditional Sensorimotor ApproachesShekinah Gracia T. Mosquera100% (2)
- Orthotics ProstheticDocument13 pagesOrthotics ProstheticAwaisNo ratings yet
- Resisted Exercise Gopi MakingDocument48 pagesResisted Exercise Gopi Makinggopi mistryNo ratings yet
- Passive Movements - KinesiologyDocument18 pagesPassive Movements - KinesiologyKanwal Khan50% (2)
- Kalten BornDocument34 pagesKalten BornjayadevanNo ratings yet
- CECS ProtocolDocument6 pagesCECS ProtocolTsz Kwan CheungNo ratings yet
- Passive Movements Kine - IIDocument20 pagesPassive Movements Kine - IIDr Sania SardarNo ratings yet
- Resisted ExerciseDocument53 pagesResisted ExerciseEliud MbuteNo ratings yet
- Passivce Range of Motion ExercisesDocument29 pagesPassivce Range of Motion Exercisesvidyasagar pagilla100% (1)
- Assessment NeuroDocument2 pagesAssessment NeurodhagallarteNo ratings yet
- PNF FullDocument46 pagesPNF FullHUZAIFA YAMAAN100% (1)
- 20 Taping ExtensorsDocument52 pages20 Taping Extensorsrima rizky nourliaNo ratings yet
- Impaired Physical MobilityDocument3 pagesImpaired Physical Mobilityvidagurl0% (1)
- Passive Movements: BY: Dr. Sonali DesaiDocument21 pagesPassive Movements: BY: Dr. Sonali DesaiBhargavNo ratings yet
- PERIPHERAL Joint MobilizationDocument53 pagesPERIPHERAL Joint MobilizationRaghu NadhNo ratings yet
- Nursing Care Plan: Submitted By: Sabay, Kyle VDocument11 pagesNursing Care Plan: Submitted By: Sabay, Kyle VKYLE SABAYNo ratings yet
- Proprioceptive Neuromuscular Facilitation Laboratory Guide: Manual Contacts TractionDocument5 pagesProprioceptive Neuromuscular Facilitation Laboratory Guide: Manual Contacts TractionJandie SagaynoNo ratings yet
- Manual TherapyDocument87 pagesManual TherapyJen Passilan100% (9)
- Suspension Therapy by Rahul Vapms CopDocument20 pagesSuspension Therapy by Rahul Vapms Copvenkata ramakrishnaiahNo ratings yet
- The Musculoskeletal Examination: Colon H - WilsonDocument5 pagesThe Musculoskeletal Examination: Colon H - WilsonAbdullah Bin SaeedNo ratings yet
- Choosing Mobs Manips ExcercisesDocument15 pagesChoosing Mobs Manips ExcercisesCatalina MusteațaNo ratings yet
- Kaltenborn Evjenth Concept of OMTDocument34 pagesKaltenborn Evjenth Concept of OMTJaan100% (1)
- 3rd Year Neuro Treatment LectureDocument31 pages3rd Year Neuro Treatment LectureSelinah Sslengs SeepeNo ratings yet
- Cyriax's Friction MassageDocument23 pagesCyriax's Friction MassageKrinal ShahNo ratings yet
- StretchingDocument15 pagesStretchingMagd.islamgmail.com MagdislamNo ratings yet
- Introduction To MovementsDocument42 pagesIntroduction To MovementsRamalingam KanagarajNo ratings yet
- Length Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesRating: 3.5 out of 5 stars3.5/5 (3)
- Do Not Give Up Your Favorite Sport For A Shoulder Dislocation !From EverandDo Not Give Up Your Favorite Sport For A Shoulder Dislocation !Rating: 1 out of 5 stars1/5 (1)
- FilgrastimDocument3 pagesFilgrastimapi-3797941No ratings yet
- Pylephlebitis - UpToDateDocument7 pagesPylephlebitis - UpToDateLeandro Tosi UgarteNo ratings yet
- CAPNOGRAPHYDocument10 pagesCAPNOGRAPHYJessica GuzmanNo ratings yet
- A Prospective Audit of Pain Profiles Following General and Urological Surgery in ChildrenDocument10 pagesA Prospective Audit of Pain Profiles Following General and Urological Surgery in ChildrenLakhwinder KaurNo ratings yet
- Muskuloskelatal (English) : Senin Selasa Rabu Kamis JumatDocument3 pagesMuskuloskelatal (English) : Senin Selasa Rabu Kamis JumatArsul RNo ratings yet
- Nephrology TestDocument22 pagesNephrology TestRishi KNair100% (1)
- Ultrasound Skin TighteningDocument7 pagesUltrasound Skin TighteningThe Vancouver Sun100% (1)
- Health Behaviors Enhancing Vs CompromisingDocument7 pagesHealth Behaviors Enhancing Vs CompromisingumibrahimNo ratings yet
- Anesthesia Technician CVDocument1 pageAnesthesia Technician CVmahbbobNo ratings yet
- Cerebrovascular Autoregulation in Pediatric Moyamoya DiseaseDocument11 pagesCerebrovascular Autoregulation in Pediatric Moyamoya DiseasewithoutlifeNo ratings yet
- Cholesterol PDFDocument32 pagesCholesterol PDFAkshad PatilNo ratings yet
- Community & PHD - CurriculumDocument6 pagesCommunity & PHD - CurriculumManish AdhikariNo ratings yet
- Allergy Blood Test (IgE)Document5 pagesAllergy Blood Test (IgE)Muhammad RaheemNo ratings yet
- Kaplan Brett EXSS3072 Initial Client Report.Document3 pagesKaplan Brett EXSS3072 Initial Client Report.BrettNo ratings yet
- NP1 NotesDocument59 pagesNP1 NotesBrianMarBeltranNo ratings yet
- MD India Preauth FormDocument2 pagesMD India Preauth FormM/s MicrotechNo ratings yet
- Penanganan Cedera KepalaDocument28 pagesPenanganan Cedera KepalaRichesio Sapata TomokumoroNo ratings yet
- Csa Form Serology Clearance Certificate s7 Oct 2014Document2 pagesCsa Form Serology Clearance Certificate s7 Oct 2014Thomas EyreNo ratings yet
- Notes: Hypoglycemics: Insulin SecretagoguesDocument6 pagesNotes: Hypoglycemics: Insulin SecretagoguesSalsabila HMNo ratings yet
- Sensory Deprivation and Loss-4Document32 pagesSensory Deprivation and Loss-4Scott Daniel Phillips100% (1)
- Frcpath Part 1 Previous Questions: Document1Document11 pagesFrcpath Part 1 Previous Questions: Document1Ali LaftaNo ratings yet
- Duke University Department of Medicine Annual Report 2013Document21 pagesDuke University Department of Medicine Annual Report 2013Duke Department of MedicineNo ratings yet
- Post HepaticDocument6 pagesPost HepaticBilla NabillaNo ratings yet
- Growth of Analytical Thinking Skills Over Time As Measured With The MATCH TestDocument7 pagesGrowth of Analytical Thinking Skills Over Time As Measured With The MATCH TestFrederico PóvoaNo ratings yet
- Hans Selye. The General Adaptation SyndromeDocument16 pagesHans Selye. The General Adaptation SyndromeCelso Sánchez Ramírez100% (2)
- Gingival Retraction Methods For Fabrication of FixDocument9 pagesGingival Retraction Methods For Fabrication of FixChokri SahbaniNo ratings yet
- PCH N1Document115 pagesPCH N1Shafie Osman AliNo ratings yet