Download as pdf or txt
You might also like
- Shop Manual BF75D - BF90D 2006-2011Document635 pagesShop Manual BF75D - BF90D 2006-2011megclay100% (2)
- Succeed in Trinity-ISE III Self-Study GuideDocument20 pagesSucceed in Trinity-ISE III Self-Study GuideHecthor77No ratings yet
- Series 60 - Section 1.11 Gear Case Cover Exhaust Gas Recirculation (EGR) ModelDocument14 pagesSeries 60 - Section 1.11 Gear Case Cover Exhaust Gas Recirculation (EGR) ModelJuan RiveraNo ratings yet
- Orthopaedics and Trauma for Medical Students and Junior ResidentsFrom EverandOrthopaedics and Trauma for Medical Students and Junior ResidentsRating: 5 out of 5 stars5/5 (3)
- 7 Essene MirrorsDocument3 pages7 Essene Mirrorsupcphln100% (4)
- Preliminary Assessment of Feasibility Study Proposal: Kingfisher School of Business and FinanceDocument5 pagesPreliminary Assessment of Feasibility Study Proposal: Kingfisher School of Business and FinanceJewel Mae MercadoNo ratings yet
- JAAOSNov2017-The Posteromedial Corner of The Knee Anatomy-DOLDDocument11 pagesJAAOSNov2017-The Posteromedial Corner of The Knee Anatomy-DOLDseatrrtleNo ratings yet
- Posterior Oblique Ligament of The Knee - State of The ArtDocument8 pagesPosterior Oblique Ligament of The Knee - State of The Art杨钦杰No ratings yet
- MCL RehaDocument15 pagesMCL RehaH HanNo ratings yet
- Evaluation and Management of PDocument14 pagesEvaluation and Management of PIndra YudhaNo ratings yet
- Lateral Collateral Ligament InjuryDocument8 pagesLateral Collateral Ligament InjuryRaeni Dwi PutriNo ratings yet
- MCL RehaDocument15 pagesMCL RehaIlham Amal MNo ratings yet
- Current Perspectives On Elbow Dislocation and InstabilityDocument15 pagesCurrent Perspectives On Elbow Dislocation and InstabilityAnonymous L9D1I7DZNo ratings yet
- Esquina Posteromedial RodillaDocument9 pagesEsquina Posteromedial RodillaSebastian RamirezNo ratings yet
- Current Concepts Review MCL - A Review On Current Concept and ManagementDocument9 pagesCurrent Concepts Review MCL - A Review On Current Concept and Managementlite.trawler-0xNo ratings yet
- Flores Et Al 2020 Imaging of The Acromioclavicular Joint Anatomy Function Pathologic Features and TreatmentDocument28 pagesFlores Et Al 2020 Imaging of The Acromioclavicular Joint Anatomy Function Pathologic Features and TreatmentIvana SovićNo ratings yet
- What's in and What's Out?: Management of Anterior Cruciate Ligament InjuryDocument13 pagesWhat's in and What's Out?: Management of Anterior Cruciate Ligament InjuryNydia OngaliaNo ratings yet
- Acl TearDocument13 pagesAcl TearAlecjohn FortoNo ratings yet
- Postero Lateral Corner of KneeDocument5 pagesPostero Lateral Corner of KneeAnwar MarthyaNo ratings yet
- Posttraumatic Boutonniere and Swan Neck Deformities Mckeon2015Document10 pagesPosttraumatic Boutonniere and Swan Neck Deformities Mckeon2015yerec51683No ratings yet
- Anatomy and Biomechanics of The Posterior Cruciate Ligament and Posterolateral CornerDocument49 pagesAnatomy and Biomechanics of The Posterior Cruciate Ligament and Posterolateral CornerRoman PopescuNo ratings yet
- Triada Terrible CCR 09lunes14Document15 pagesTriada Terrible CCR 09lunes14Juan Manuel CastilloNo ratings yet
- Anatomy Biomechanics Lateral Side Knee Surgical ImplicationsDocument8 pagesAnatomy Biomechanics Lateral Side Knee Surgical ImplicationsFasilNigusseNo ratings yet
- The Collateral Ligaments and PosterolateralDocument13 pagesThe Collateral Ligaments and Posterolateralyanina vaesNo ratings yet
- Mar2012 CCDocument12 pagesMar2012 CCJavierLarenasNo ratings yet
- Or MCL FinalDocument37 pagesOr MCL FinalKyra Lalaine Angub CervantesNo ratings yet
- Posterior Malleolus Fracture.6Document9 pagesPosterior Malleolus Fracture.6cooperorthopaedicsNo ratings yet
- Adult Brachial Plexus InjuryDocument13 pagesAdult Brachial Plexus Injurysunshine bloomNo ratings yet
- Isolated Medial Collateral Ligament Injuries in The KneeDocument6 pagesIsolated Medial Collateral Ligament Injuries in The KneekenthepaNo ratings yet
- Complex Elbow Instability: Matthew Dipaola, MD, William B. Geissler, MD, A. Lee Osterman, MDDocument14 pagesComplex Elbow Instability: Matthew Dipaola, MD, William B. Geissler, MD, A. Lee Osterman, MDAndrea Z MilanoNo ratings yet
- Biomechanics LcaDocument13 pagesBiomechanics Lcamono1144No ratings yet
- Anatomic Posterolateral Corner ReconstructionDocument10 pagesAnatomic Posterolateral Corner Reconstructionethan.dumontNo ratings yet
- Cme PCLDocument14 pagesCme PCLjkfkongNo ratings yet
- Cme 200905Document4 pagesCme 200905jkfkongNo ratings yet
- MPFL Rehab ProtocolDocument18 pagesMPFL Rehab ProtocolharyskawdNo ratings yet
- Grupo 2 Current Trends in Anterior Cruciate Ligament Reconstruction 1 378755938Document10 pagesGrupo 2 Current Trends in Anterior Cruciate Ligament Reconstruction 1 378755938eduacv2No ratings yet
- Chiropractic Technique Principles and Procedures 3Document22 pagesChiropractic Technique Principles and Procedures 3Colors of LifeNo ratings yet
- Evaluation and Treatment of Acromioclavicular Joint InjuriesDocument14 pagesEvaluation and Treatment of Acromioclavicular Joint InjuriesmichellmariottiNo ratings yet
- Adult Traumatic Brachial Plexus InjuriesDocument15 pagesAdult Traumatic Brachial Plexus Injuriesapi-241264935No ratings yet
- 1 s2.0 S2666061X19300057 MainDocument8 pages1 s2.0 S2666061X19300057 Mainanon_997737934No ratings yet
- Sacral Alae S1 and S2Document11 pagesSacral Alae S1 and S2Aysiah AzhariNo ratings yet
- Applied Radiology Featured Article (Via Radrounds)Document7 pagesApplied Radiology Featured Article (Via Radrounds)radRounds Radiology Network100% (1)
- Abjs 8 332Document11 pagesAbjs 8 332angelluis1980No ratings yet
- Kalawadia 2018Document9 pagesKalawadia 2018سيف فلاح حسنNo ratings yet
- Diagnosis and Treatment of Rotatory Knee InstabilityDocument10 pagesDiagnosis and Treatment of Rotatory Knee Instability杨钦杰No ratings yet
- Cervical Spine InjuryDocument18 pagesCervical Spine InjuryGabriel KlemensNo ratings yet
- Simple Elbow Dislocation: Paul M. Robinson, Emmet Griffiths and Adam C WattsDocument10 pagesSimple Elbow Dislocation: Paul M. Robinson, Emmet Griffiths and Adam C WattsAnnisa HidayatiNo ratings yet
- Amis 2012Document8 pagesAmis 2012abdo houamerNo ratings yet
- MRI of The Posterolateral Corner Injury: A Concise ReviewDocument6 pagesMRI of The Posterolateral Corner Injury: A Concise ReviewIntanNo ratings yet
- Kim Technique MCL and POLDocument5 pagesKim Technique MCL and POLManuel Vergillos LunaNo ratings yet
- Elbow Dislocation Nima Rezaie 2020Document19 pagesElbow Dislocation Nima Rezaie 2020Freddy EnríquezNo ratings yet
- Meniscus Repair Part 1 Biology, Function, Tear.7Document7 pagesMeniscus Repair Part 1 Biology, Function, Tear.7cooperorthopaedicsNo ratings yet
- Medial Malleolar FracturesDocument10 pagesMedial Malleolar FracturesSusan Ly VillalobosNo ratings yet
- Hombro Inlges PDFDocument6 pagesHombro Inlges PDFOscar Segun DoNo ratings yet
- Traumatic Knee Dislocations Evaluation, Management, and Surgical TreatmentDocument15 pagesTraumatic Knee Dislocations Evaluation, Management, and Surgical TreatmentToño Solano NogueraNo ratings yet
- Fraser Et Al (2016) Ne Pas RetenirDocument13 pagesFraser Et Al (2016) Ne Pas RetenirgasNo ratings yet
- Classification of Pelvic Fractures and Its Clinical RelevanceDocument6 pagesClassification of Pelvic Fractures and Its Clinical RelevanceMohamed AzeemNo ratings yet
- SMR 00275 ShoulderDocument15 pagesSMR 00275 ShoulderIulian FrunzăNo ratings yet
- Fraser MoodieDocument11 pagesFraser MoodieWiindaNo ratings yet
- Complex Elbow InstabilityDocument9 pagesComplex Elbow InstabilityAristoteles Plato SocratesNo ratings yet
- Mittlmeier 2018Document17 pagesMittlmeier 2018vijaypatel4282No ratings yet
- Relation in SemiDocument8 pagesRelation in SemiLuisNo ratings yet
- High Ankle Sprain in Athletes Diagnostic Challenges and Review of The LiteratureDocument9 pagesHigh Ankle Sprain in Athletes Diagnostic Challenges and Review of The LiteratureOscar NgNo ratings yet
- Mackenzieetal. 2015 Anevidence BasedreviewofcurrentperceptionswiDocument9 pagesMackenzieetal. 2015 Anevidence BasedreviewofcurrentperceptionswiJamNo ratings yet
- Principles and Management of Acute Orthopaedic Trauma: Third EditionFrom EverandPrinciples and Management of Acute Orthopaedic Trauma: Third EditionNo ratings yet
- The Acetabular Labrum Anatomic and Functional.6Document8 pagesThe Acetabular Labrum Anatomic and Functional.6cooperorthopaedicsNo ratings yet
- Nonsurgical Versus Surgical Management Of.3Document8 pagesNonsurgical Versus Surgical Management Of.3cooperorthopaedicsNo ratings yet
- Unplanned Resection of Sarcoma.3Document10 pagesUnplanned Resection of Sarcoma.3cooperorthopaedicsNo ratings yet
- Stepwise Safe Access in Hip Arthroscopy in The.1Document9 pagesStepwise Safe Access in Hip Arthroscopy in The.1cooperorthopaedicsNo ratings yet
- Cartilage Regeneration.7Document9 pagesCartilage Regeneration.7cooperorthopaedicsNo ratings yet
- Management of Intraoperative Graft Related.3Document9 pagesManagement of Intraoperative Graft Related.3cooperorthopaedicsNo ratings yet
- COA SAEQuestionLibrary 2Document104 pagesCOA SAEQuestionLibrary 2cooperorthopaedicsNo ratings yet
- Musculoskeletal Effects of Cancer and Cancer.5Document13 pagesMusculoskeletal Effects of Cancer and Cancer.5cooperorthopaedicsNo ratings yet
- Principles of Amputation Surgery, Prosthetics, And.7Document12 pagesPrinciples of Amputation Surgery, Prosthetics, And.7cooperorthopaedicsNo ratings yet
- X Is Surgical Resection of The Primary Site.17Document12 pagesX Is Surgical Resection of The Primary Site.17cooperorthopaedicsNo ratings yet
- Sports 2021Document78 pagesSports 2021cooperorthopaedicsNo ratings yet
- X - The Natural History of Benign Bone Tumors of The Extremities in Asymptomatic ChildrenDocument6 pagesX - The Natural History of Benign Bone Tumors of The Extremities in Asymptomatic ChildrencooperorthopaedicsNo ratings yet
- Fellows Reading List - 2017-18Document8 pagesFellows Reading List - 2017-18cooperorthopaedicsNo ratings yet
- Journal Pre-Proof: Arthroscopy: The Journal of Arthroscopic and Related SurgeryDocument29 pagesJournal Pre-Proof: Arthroscopy: The Journal of Arthroscopic and Related SurgerycooperorthopaedicsNo ratings yet
- S6 Upper Cervical Spine TraumaDocument82 pagesS6 Upper Cervical Spine TraumacooperorthopaedicsNo ratings yet
- Joc60156 2451 2459Document9 pagesJoc60156 2451 2459cooperorthopaedicsNo ratings yet
- Next Generation Sequencing Results Require Higher.1239Document8 pagesNext Generation Sequencing Results Require Higher.1239cooperorthopaedicsNo ratings yet
- PIIS1058274622009053Document6 pagesPIIS1058274622009053cooperorthopaedicsNo ratings yet
- Interview Questions in EducationDocument9 pagesInterview Questions in EducationGyasi YamoahNo ratings yet
- Ujian Setara 1 2017 KimiaDocument9 pagesUjian Setara 1 2017 KimiaZulkifli Bin PariNo ratings yet
- Objective:: Feed Tanks Batch ReactorDocument5 pagesObjective:: Feed Tanks Batch Reactorfareeha saeedNo ratings yet
- DSP Glucose OxidaseDocument1 pageDSP Glucose OxidaseJowanna BurceNo ratings yet
- CBEN408 06 Field Operations Inlet ReceivingDocument59 pagesCBEN408 06 Field Operations Inlet ReceivingForcus onNo ratings yet
- Closed Hand Only Reduced Value When Hand Open: 2-Han Hands KEY 1-Han HandsDocument1 pageClosed Hand Only Reduced Value When Hand Open: 2-Han Hands KEY 1-Han Hands8o1kfW9No ratings yet
- Presentation On Solid Waste ManagementDocument14 pagesPresentation On Solid Waste ManagementRajesh HarmukhNo ratings yet
- ELECTROMYOGRAPHYDocument7 pagesELECTROMYOGRAPHYsariNo ratings yet
- Solid State13thDocument19 pagesSolid State13thRaju SinghNo ratings yet
- Powered ExoskeletonDocument22 pagesPowered ExoskeletonSarfaras Ali K100% (1)
- Category C Dog Cat Import Flowchart Apr2018Document4 pagesCategory C Dog Cat Import Flowchart Apr2018J FNo ratings yet
- Literature Review On MotivationDocument6 pagesLiterature Review On MotivationAshma SthaNo ratings yet
- Solution Manual For Mathematical Applications For The Management Life and Social Sciences 12th Edition Ronald J Harshbarger James J ReynoldsDocument36 pagesSolution Manual For Mathematical Applications For The Management Life and Social Sciences 12th Edition Ronald J Harshbarger James J Reynoldsdiclinicauroravsl9100% (53)
- France Food & Drink Report Q4Document62 pagesFrance Food & Drink Report Q4N. H.No ratings yet
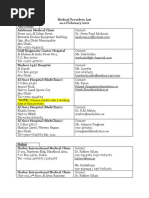
- MetLife Medical Providers List As of 20 Feb 2021 PDFDocument7 pagesMetLife Medical Providers List As of 20 Feb 2021 PDFherra husainNo ratings yet
- Muscle Energy Model 9-30-08.coryDocument4 pagesMuscle Energy Model 9-30-08.coryWilliam BlairNo ratings yet
- Toshani - Jan Feb 1992 Vol11Document16 pagesToshani - Jan Feb 1992 Vol11Ram Kripal MishraNo ratings yet
- A Color Atlas of Poultry Diseases by J L VegadDocument144 pagesA Color Atlas of Poultry Diseases by J L VegadId DyNo ratings yet
- Hypertension FamcoDocument42 pagesHypertension FamcoMusleh Al MusalhiNo ratings yet
- Vertebrates and Non VertDocument13 pagesVertebrates and Non VertLanie Grace Sandhu100% (1)
- Butternut Squash SoupDocument1 pageButternut Squash SouplyllacycusNo ratings yet
- 4-Spare Parts Management 1Document76 pages4-Spare Parts Management 1Mohd Kamil100% (4)
- 3 Reasons You Can't Train Like JuicersDocument6 pages3 Reasons You Can't Train Like JuicersaligaramNo ratings yet
- Endocrine and Urinary SystemDocument5 pagesEndocrine and Urinary SystemShereen ManabilangNo ratings yet
- Reducing Work Related Psychological Ill Health and Sickness AbsenceDocument15 pagesReducing Work Related Psychological Ill Health and Sickness AbsenceBM2062119PDPP Pang Kuok WeiNo ratings yet