Download as pdf or txt
You might also like
- Day of The DragonDocument14 pagesDay of The DragonLauraHenson100% (3)
- RN Fundamentals Online Practice 2016 A Study Online at QuizletDocument14 pagesRN Fundamentals Online Practice 2016 A Study Online at QuizletDerek Scott Tripp100% (1)
- Difference Between Serum and Plasma PDFDocument3 pagesDifference Between Serum and Plasma PDFkisame akatsuki100% (5)
- Anti Hypertensives NEWDocument91 pagesAnti Hypertensives NEWhoor e ainNo ratings yet
- Lecture 24-25 - Antihypertensive AgentsDocument30 pagesLecture 24-25 - Antihypertensive AgentsJedoNo ratings yet
- Hypertension: Hozan Jaza MSC Clinical Pharmacy College of Pharmacy 10/12/2020Document81 pagesHypertension: Hozan Jaza MSC Clinical Pharmacy College of Pharmacy 10/12/2020Alan K MhamadNo ratings yet
- Antihypertensive Drugs RTDocument41 pagesAntihypertensive Drugs RTMaherNo ratings yet
- AntihipertensiDocument39 pagesAntihipertensiHarri HardiNo ratings yet
- Pharmacotherapy of HypertensionDocument52 pagesPharmacotherapy of HypertensionDrVinod Kumar Goud VemulaNo ratings yet
- Vasoactive DrugsDocument61 pagesVasoactive DrugsAde Gustina SiahaanNo ratings yet
- 1 Drugs For HypertensionDocument62 pages1 Drugs For HypertensionSaniNo ratings yet
- Hypertension PDFDocument57 pagesHypertension PDFrahul m dNo ratings yet
- ACE Inhibitors & Angiotensin II Antagonists: October 1997Document4 pagesACE Inhibitors & Angiotensin II Antagonists: October 1997indee533No ratings yet
- Pharmacology 3 - Management of Heart FailureDocument59 pagesPharmacology 3 - Management of Heart Failurealbatros000No ratings yet
- Cardiovascular Drugs Gizi DR DianDocument56 pagesCardiovascular Drugs Gizi DR DianTriana Dessy FitriantiNo ratings yet
- Antihypertensive DrugsDocument64 pagesAntihypertensive DrugsPSC100% (1)
- Farmakologi 1 Antihypertension: NURUL HASANAH (1800085)Document31 pagesFarmakologi 1 Antihypertension: NURUL HASANAH (1800085)MutiaraBintangNo ratings yet
- CVS (HF, HTN) PharmacologyDocument99 pagesCVS (HF, HTN) PharmacologyCherenet TomaNo ratings yet
- Anti HypretensivesDocument18 pagesAnti HypretensivesLeena AlateeqNo ratings yet
- Anti HypretensivesDocument18 pagesAnti HypretensivesLeena AlateeqNo ratings yet
- Chapter 35Document41 pagesChapter 35HannaNo ratings yet
- Tugas DR Yoma AncaDocument30 pagesTugas DR Yoma Ancaaby mayuNo ratings yet
- Antihypertensives Cardiovascular PharmacologyDocument52 pagesAntihypertensives Cardiovascular PharmacologyAlan LealNo ratings yet
- Pharmacological-Management-of-HypertensionDocument35 pagesPharmacological-Management-of-Hypertensiontf.almutairi88No ratings yet
- Pharmacology Semi FinalsDocument269 pagesPharmacology Semi FinalsTrishaNo ratings yet
- CVS Pharmacology For Health ScienceDocument54 pagesCVS Pharmacology For Health ScienceMelesNo ratings yet
- Diabetes HypertensionDocument29 pagesDiabetes HypertensionAnimesh PaulNo ratings yet
- AntihypertensiveDocument94 pagesAntihypertensiveadityarupusrikantaNo ratings yet
- ACE INHIBITORS & ARBsDocument31 pagesACE INHIBITORS & ARBsMaria khurshidNo ratings yet
- Chapter 11 Antihypertensive AgentsDocument11 pagesChapter 11 Antihypertensive AgentsChristine Annmarie TapawanNo ratings yet
- Drugs Used To Treat Cardiovascular Diseases: HypertensionDocument35 pagesDrugs Used To Treat Cardiovascular Diseases: HypertensionAyro Business CenterNo ratings yet
- Anti-Hypertensive 2Document49 pagesAnti-Hypertensive 2pushpaNo ratings yet
- CVS PharmacologyDocument60 pagesCVS PharmacologyGølà Sèèñàà–baale irraaNo ratings yet
- Pathophysiology & Therapeutics IDocument454 pagesPathophysiology & Therapeutics IMuhammad AbdullahiNo ratings yet
- Antihypertensive Drugs: S. Parasuraman, M.Pharm., PH.D.Document44 pagesAntihypertensive Drugs: S. Parasuraman, M.Pharm., PH.D.Shreya SinhaNo ratings yet
- Lec 6 Anti-Hypertensive DrugsDocument31 pagesLec 6 Anti-Hypertensive Drugsph211333No ratings yet
- Ace Inhibutors MailDocument5 pagesAce Inhibutors MailWendy AdaoNo ratings yet
- Antihypertensive AgentsDocument39 pagesAntihypertensive AgentsFuhrer OdebsNo ratings yet
- Management of Hypertenisve Emergencies and Urgency: DR - Supriya 1 Year General MedicineDocument33 pagesManagement of Hypertenisve Emergencies and Urgency: DR - Supriya 1 Year General MedicineRahul NaniNo ratings yet
- Skema HipertensiDocument4 pagesSkema HipertensiAndri wijayaNo ratings yet
- Y7PH0566, Yedla Pradeep Kumar, 4 B.Pharmacy, Cips, Lam, GunturDocument33 pagesY7PH0566, Yedla Pradeep Kumar, 4 B.Pharmacy, Cips, Lam, Gunturప్రదీప్ కుమార్100% (4)
- Cardiac Inotropes in Treatment of Heart Failure Fight (Autosaved)Document32 pagesCardiac Inotropes in Treatment of Heart Failure Fight (Autosaved)Insan IlmanNo ratings yet
- Antihypertensive AgentsDocument17 pagesAntihypertensive AgentsGunjan KalyaniNo ratings yet
- Scenario ThreeDocument25 pagesScenario Threeapi-3831474No ratings yet
- Blood Pressure Medications Lecture 2020 4 Pod CastsDocument46 pagesBlood Pressure Medications Lecture 2020 4 Pod CastsfbjsjdfhNo ratings yet
- Disease Management - HypertensionDocument46 pagesDisease Management - HypertensionMuhammad Basit Mujahid. 105No ratings yet
- HypertensionDocument46 pagesHypertensionElsai EsbNo ratings yet
- HypertensionDocument141 pagesHypertensionAseelNo ratings yet
- AntiHypertensives (Autosaved)Document64 pagesAntiHypertensives (Autosaved)UsamaNo ratings yet
- Acute Kidney InjuryDocument64 pagesAcute Kidney InjuryBIAN ALKHAZMARINo ratings yet
- Hypertension TejaDocument64 pagesHypertension TejaAnushka MaheshwariNo ratings yet
- HypertensionDocument55 pagesHypertensionSr.Jyothy SABSNo ratings yet
- 3 DrugsforHeartFailureDocument60 pages3 DrugsforHeartFailureJov CelNo ratings yet
- Antihypertensive Drugs: DR. DR Umi Kalssum MkesDocument58 pagesAntihypertensive Drugs: DR. DR Umi Kalssum MkesadilaalifnugrahaeniNo ratings yet
- HYPERTENSIONDocument5 pagesHYPERTENSIONRajesh RamanNo ratings yet
- 10-11 Treatment of HypertensionDocument11 pages10-11 Treatment of HypertensionHanif GandohNo ratings yet
- Hypertension: Kieran Mcglade Nov 2001 Department of General Practice QubDocument25 pagesHypertension: Kieran Mcglade Nov 2001 Department of General Practice Qubankitkar9No ratings yet
- Antihypertensive Drugs: Dr/Azza Baraka Prof of Clinical Pharmacology Faculty of Medicine Alexandria UniversityDocument71 pagesAntihypertensive Drugs: Dr/Azza Baraka Prof of Clinical Pharmacology Faculty of Medicine Alexandria UniversityMoonAIRNo ratings yet
- Inhibitors of AngiotensinDocument37 pagesInhibitors of AngiotensinBoyu GrtrNo ratings yet
- Oleh: Bagian Ilmu Penyakit Dalam FK Universitas Sultan Agung Semarang 2012Document40 pagesOleh: Bagian Ilmu Penyakit Dalam FK Universitas Sultan Agung Semarang 2012Mbenk NjoeNo ratings yet
- Anti HypertensionDocument63 pagesAnti HypertensionAngga CahyadiNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- 07 Nucleic Acids Test PDFDocument8 pages07 Nucleic Acids Test PDFUkjun JungNo ratings yet
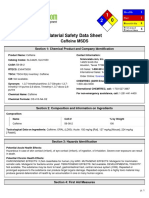
- Msds CaffeineDocument6 pagesMsds CaffeineNovia RegitaNo ratings yet
- Fish Diseases FactsheetDocument2 pagesFish Diseases FactsheetWayneNo ratings yet
- LifeWave X39 Pilot Demuestra Cambios Ligeros ActivadosDocument12 pagesLifeWave X39 Pilot Demuestra Cambios Ligeros Activadosave_fenix_mileniumNo ratings yet
- Coordination and Response in Humans: 12.6 Endocrine SystemDocument16 pagesCoordination and Response in Humans: 12.6 Endocrine Systemwienna1987No ratings yet
- Foot Anatomy Tendons and LigamentsDocument3 pagesFoot Anatomy Tendons and Ligamentsanak_kost_aji_baungNo ratings yet
- Neurological Basis of Emotion, Learning and MemoryDocument6 pagesNeurological Basis of Emotion, Learning and MemoryAditi GaikwadNo ratings yet
- Oligohydramnios 11Document32 pagesOligohydramnios 11Otchi Pudtrie WijayaNo ratings yet
- NexGen Flexion Balancing Instruments Surgical Technique 2897-5967-031-00 Rev1!29!2811 2009 29Document48 pagesNexGen Flexion Balancing Instruments Surgical Technique 2897-5967-031-00 Rev1!29!2811 2009 29flo1987No ratings yet
- Energy and Respiration - 2Document39 pagesEnergy and Respiration - 2Rohan PaneruNo ratings yet
- Alergi Yang Disebabkan KupuDocument7 pagesAlergi Yang Disebabkan KupuDesi Suryani DewiNo ratings yet
- #1 Anatomi Fisiologi Urogenital SystemDocument4 pages#1 Anatomi Fisiologi Urogenital SystemNur azriyati PutriNo ratings yet
- Tonation - Spectro-Chrome MetryDocument5 pagesTonation - Spectro-Chrome MetryitounosNo ratings yet
- 10 RulesDocument3 pages10 Rulesapi-194148222No ratings yet
- Biomechanics of Edentulous StateDocument15 pagesBiomechanics of Edentulous StateNadeemNo ratings yet
- Low Cardiac OutputDocument23 pagesLow Cardiac OutputMohamed ElgayarNo ratings yet
- Secondary SurveyDocument2 pagesSecondary SurveySakta SuryagunaNo ratings yet
- Ursin, H. (1998) The Psychology in PsychoneuroendocrinologyDocument16 pagesUrsin, H. (1998) The Psychology in PsychoneuroendocrinologyCristian jimènezNo ratings yet
- Mra CRDocument87 pagesMra CRyailetc3796No ratings yet
- Department of Agril. Entomology College of Agriculture, DapoliDocument69 pagesDepartment of Agril. Entomology College of Agriculture, DapoliVaibhav DafaleNo ratings yet
- Bergel and Morrison 5-Hydroxyindole. 5-Hydroxyindole.: 5-Methoxyindole-2-Carboxylic 2-Nitro-5-HydroxytolueneDocument1 pageBergel and Morrison 5-Hydroxyindole. 5-Hydroxyindole.: 5-Methoxyindole-2-Carboxylic 2-Nitro-5-HydroxytolueneAnonymous FigYuONxuuNo ratings yet
- Autism SpectrumDocument8 pagesAutism SpectrumNeutron ZionNo ratings yet
- 2020NRN - Perivascular Spaces in The Brain SUPPL PDFDocument2 pages2020NRN - Perivascular Spaces in The Brain SUPPL PDFJuan Carlos LazoNo ratings yet
- HL Paper2Document18 pagesHL Paper2Jane ChangNo ratings yet
- Scientific Signs of Qur'an & SunnahDocument26 pagesScientific Signs of Qur'an & SunnahISLAMICULTURE100% (11)
- Lesson Plan in Cells (Demo)Document3 pagesLesson Plan in Cells (Demo)Gerald Galvez ApostolNo ratings yet
- 10.1007@s11604 019 00901 8Document15 pages10.1007@s11604 019 00901 8sayed hossein hashemiNo ratings yet