
Arrhythmia
Arrhythmia
You might also like
- Complaint Emergency HandbookDocument306 pagesComplaint Emergency HandbookUsman Amjad100% (3)
- PALS Case Scenario Testing ChecklistDocument12 pagesPALS Case Scenario Testing ChecklistJohn David D. ErguizaNo ratings yet
- EKG Findings and Arrhythmias - USMLE Step 2 CK ExamDocument3 pagesEKG Findings and Arrhythmias - USMLE Step 2 CK ExamSamah Khan100% (2)
- ECG WorksheetDocument3 pagesECG WorksheetElaiza UyNo ratings yet
- ACLS For TachycardiaDocument31 pagesACLS For TachycardiaTausif HaqueNo ratings yet
- Atrial FibrillationDocument24 pagesAtrial FibrillationFani Butt50% (2)
- ABCDs During A Code Blue Response in An Adult PatientDocument23 pagesABCDs During A Code Blue Response in An Adult PatientChakra PuspitaNo ratings yet
- ACLS Appendix 3Document32 pagesACLS Appendix 3tostc100% (1)
- Acls - Megacode - UpdatedDocument4 pagesAcls - Megacode - UpdatedDivine Dela Pena100% (1)
- ACLS Pocket GuideDocument5 pagesACLS Pocket Guidedragnu100% (1)
- 1 Management of TachyarrythmiasDocument72 pages1 Management of TachyarrythmiassalsabeelNo ratings yet
- GINA-2023-Full-report-23_07_06-WMS (2)Document61 pagesGINA-2023-Full-report-23_07_06-WMS (2)Lamessa MessiNo ratings yet
- Arrhythmia NewDocument73 pagesArrhythmia Newlohith saiNo ratings yet
- Chapter - 036 Arrhythmias ClassDocument129 pagesChapter - 036 Arrhythmias ClassWisdomIsMiseryNo ratings yet
- Emergency in Medicine 2012Document202 pagesEmergency in Medicine 2012micheal1960No ratings yet
- Arrhythmia in Emergency 111Document21 pagesArrhythmia in Emergency 111Iyas JehadNo ratings yet
- Tachycardiafaez 161221035148Document36 pagesTachycardiafaez 161221035148hartanto_budi6222No ratings yet
- Cardiac Arrythmias in The ED Menbeu Edited From AnaDocument106 pagesCardiac Arrythmias in The ED Menbeu Edited From AnaTemesgen Geleta100% (1)
- Life Threatening Arrhythmia and ManagementDocument40 pagesLife Threatening Arrhythmia and ManagementRuki Hartawan100% (1)
- 28,29 Management of Cardiac ArrhythmiasDocument41 pages28,29 Management of Cardiac ArrhythmiasSL Dr ChEMiSNo ratings yet
- Atrial FibrillationDocument8 pagesAtrial FibrillationduhsknwsNo ratings yet
- Arrhythmia 6 YrDocument72 pagesArrhythmia 6 YrPiyush MalikNo ratings yet
- 41 Paediatric ArrhythmiasDocument4 pages41 Paediatric ArrhythmiasnasibdinNo ratings yet
- Arrhythmia, Pericardial and Myocardial Diseases (DR Praveen) 2Document44 pagesArrhythmia, Pericardial and Myocardial Diseases (DR Praveen) 2hashini1997nisansalaNo ratings yet
- Diagnosis Dan Tatalaksana Awal SVTDocument47 pagesDiagnosis Dan Tatalaksana Awal SVTZuly Vita AulyaNo ratings yet
- Tachy/賸)Document28 pagesTachy/賸)Jason LinNo ratings yet
- ARITMIADocument47 pagesARITMIASarah JR Nur AzizahNo ratings yet
- Arrhythmias: Sing Khien Tiong Gpst1Document34 pagesArrhythmias: Sing Khien Tiong Gpst1preethi preethaNo ratings yet
- ECG Dysrhthmias IIIDocument31 pagesECG Dysrhthmias IIIAmani Kayed100% (1)
- Atrial FibrillationDocument50 pagesAtrial Fibrillationvarun_swmNo ratings yet
- Atrial Fibrillation (AF)Document24 pagesAtrial Fibrillation (AF)farmasi_hm100% (1)
- 3881 - Prosedur Pendaftaran Internship Per November 2016Document57 pages3881 - Prosedur Pendaftaran Internship Per November 2016Munawir_Syam91No ratings yet
- IC1 - Arrhythmia - 2012 EDITEDDocument42 pagesIC1 - Arrhythmia - 2012 EDITEDrazorazNo ratings yet
- Workshop Pit IV THN 2017Document57 pagesWorkshop Pit IV THN 2017anettepardedeNo ratings yet
- Aritmia LetalDocument49 pagesAritmia LetalfebriyakNo ratings yet
- Atrial Fibrillation: Bibek Raj Poudel Intern Pahs-SomDocument34 pagesAtrial Fibrillation: Bibek Raj Poudel Intern Pahs-SomKishor K AdhikariNo ratings yet
- Ecg Class Atrial Fibrillation Power PointDocument21 pagesEcg Class Atrial Fibrillation Power PointRoshilNo ratings yet
- Atrial Fibrillation: Dr. Zirath + Dr. MehtaDocument29 pagesAtrial Fibrillation: Dr. Zirath + Dr. MehtaAjayNo ratings yet
- Atrial FibrillationDocument50 pagesAtrial Fibrillationkapil khanalNo ratings yet
- Curs Engl S Preexcit Corect Nic MPDocument72 pagesCurs Engl S Preexcit Corect Nic MPErland BordNo ratings yet
- A Fib in 60 Yr Old ManDocument32 pagesA Fib in 60 Yr Old ManNurul HikmahNo ratings yet
- Medicine Paper Number 1Document8 pagesMedicine Paper Number 1arvindNo ratings yet
- Supraventricular Tachycardia: Teresa Menendez Hood, MD FACCDocument39 pagesSupraventricular Tachycardia: Teresa Menendez Hood, MD FACCReinsy NoviNo ratings yet
- SVT PresentationDocument39 pagesSVT PresentationReinsy NoviNo ratings yet
- ArrhythmiasDocument48 pagesArrhythmiasHarshan JeyakumarNo ratings yet
- ATRIAL FIBRILLATION Anil KRDocument41 pagesATRIAL FIBRILLATION Anil KRanil sahNo ratings yet
- ArrhythmiasDocument53 pagesArrhythmiasabotreka056No ratings yet
- ECG Class ON VT PowerpointDocument24 pagesECG Class ON VT PowerpointRoshilNo ratings yet
- 5 ArrhythmiaDocument44 pages5 ArrhythmiaDanny DesuNo ratings yet
- Hippo EM Board Review - Bradycardia - A Simplified Approach Written Summary 2Document10 pagesHippo EM Board Review - Bradycardia - A Simplified Approach Written Summary 2alexandertorresreyNo ratings yet
- Cardiac ArrythmiaDocument16 pagesCardiac ArrythmiaHossen AliNo ratings yet
- Practice Essentials: Essential Updates: Distinguishing Between Left-And Right-Sided Atrial TachycardiaDocument28 pagesPractice Essentials: Essential Updates: Distinguishing Between Left-And Right-Sided Atrial TachycardiaRully SyahrizalNo ratings yet
- Cardiac Rhythm and Related Disorders: Marshell Tendean, MD Department of Internal Medicine UKRIDA JakartaDocument39 pagesCardiac Rhythm and Related Disorders: Marshell Tendean, MD Department of Internal Medicine UKRIDA JakartaFatimah Hartina FaradillahNo ratings yet
- Farmakologi Anti AritmiaDocument26 pagesFarmakologi Anti AritmiaAzzam nur TaufikurrahmanNo ratings yet
- Vdocument in Arrhythmia Diagnosis and Management محمد امريضDocument54 pagesVdocument in Arrhythmia Diagnosis and Management محمد امريضHelene AlawamiNo ratings yet
- Cardiac Arrhythmia 171209212142 2Document74 pagesCardiac Arrhythmia 171209212142 2Gunel Sadiqova100% (1)
- Cardiac Rhythm and Related Disorders: - Marshell Tendean, MD - Department of Internal Medicine UKRIDA JakartaDocument50 pagesCardiac Rhythm and Related Disorders: - Marshell Tendean, MD - Department of Internal Medicine UKRIDA JakartavaiyenNo ratings yet
- Atrial Fibrillation HandoutDocument5 pagesAtrial Fibrillation HandoutAlfa AlfinNo ratings yet
- Atrial FibrillationDocument1 pageAtrial FibrillationshakyaNo ratings yet
- ECG Symcard 2016 - Ventricular ArrhythmiaDocument41 pagesECG Symcard 2016 - Ventricular ArrhythmiaRadinal MauludiNo ratings yet
- Supplementary Material 4.3 Cardiac Rhythm Disorders-2Document14 pagesSupplementary Material 4.3 Cardiac Rhythm Disorders-2Andrea Love PalomoNo ratings yet
- Lecture2 3Document44 pagesLecture2 3Amanda HizerNo ratings yet
- Management of Cardiac ArrestDocument40 pagesManagement of Cardiac ArrestMark Francis NaniaNo ratings yet
- BradyarrthmiaDocument73 pagesBradyarrthmiaKuba ArebaNo ratings yet
- Donaldson_VT Diagnosis_TherapyDocument34 pagesDonaldson_VT Diagnosis_Therapygoldenday_hdpNo ratings yet
- Arrhythmias PDFDocument29 pagesArrhythmias PDFbencleeseNo ratings yet
- Approach To PalpitationsDocument74 pagesApproach To PalpitationsDarawan MirzaNo ratings yet
- Microsoft Word - Validation of Risk Score FPR Postoperative Nausea and Vomiting in Patients Undergoing General Anaesthesia at UTHDocument46 pagesMicrosoft Word - Validation of Risk Score FPR Postoperative Nausea and Vomiting in Patients Undergoing General Anaesthesia at UTHUWIMANA Jean ClaudeNo ratings yet
- OO Royal Mirage Coronavirus Management Plan - Master Plan WorkingDocument52 pagesOO Royal Mirage Coronavirus Management Plan - Master Plan WorkingUWIMANA Jean ClaudeNo ratings yet
- Volatile Costs Calculations ZORADocument11 pagesVolatile Costs Calculations ZORAUWIMANA Jean ClaudeNo ratings yet
- Gestational Hypertension and Preeclampsia ACOG.46Document24 pagesGestational Hypertension and Preeclampsia ACOG.46UWIMANA Jean ClaudeNo ratings yet
- CBM Scholarship Call For Applications 2021-2022Document3 pagesCBM Scholarship Call For Applications 2021-2022UWIMANA Jean ClaudeNo ratings yet
- Book 1Document93 pagesBook 1UWIMANA Jean ClaudeNo ratings yet
- Single Best Answer MCQs in Anaesthesia Volume II.14Document1 pageSingle Best Answer MCQs in Anaesthesia Volume II.14UWIMANA Jean ClaudeNo ratings yet
- PALS Nitty Gritty Study Guide FINALDocument11 pagesPALS Nitty Gritty Study Guide FINALuncmikee1997100% (1)
- Arrhythmia CBLDocument7 pagesArrhythmia CBLRyuuzakiDNNo ratings yet
- ACLS AgorithmDocument55 pagesACLS AgorithmkpsuanNo ratings yet
- 9 - Series 2022Document8 pages9 - Series 2022Vijay UNo ratings yet
- Quiz 35, 36, 37Document47 pagesQuiz 35, 36, 37dotleds100% (1)
- NP4 RECALLS5 AnswersDocument31 pagesNP4 RECALLS5 AnswersAhrisJeannine EscuadroNo ratings yet
- R Series Product ManualDocument186 pagesR Series Product ManualppdeepakNo ratings yet
- Basic ECG Interpretation MWDocument211 pagesBasic ECG Interpretation MWLorelie AsisNo ratings yet
- Resident Survival Guide: (Include Ranges of Any Abnormal Vital Signs But Also Include The Current Value For All Vitals.)Document104 pagesResident Survival Guide: (Include Ranges of Any Abnormal Vital Signs But Also Include The Current Value For All Vitals.)scalixto100% (1)
- DysrhythmiasDocument67 pagesDysrhythmiashhh hhhNo ratings yet
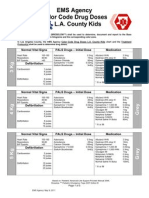
- EMS Agency Color Code Drug Doses L. L.A. County Kids: Normal Vital Signs PALS Drugs - Initial Dose MedicationDocument5 pagesEMS Agency Color Code Drug Doses L. L.A. County Kids: Normal Vital Signs PALS Drugs - Initial Dose MedicationCruz VerdeNo ratings yet
- Reanimacion CardiopulmonarDocument15 pagesReanimacion CardiopulmonarVictoriano ValienteNo ratings yet
- Ecg NotesDocument35 pagesEcg NotesDanielle100% (1)
- Cardiac Arrhythmia in Children PDFDocument50 pagesCardiac Arrhythmia in Children PDFNorhafizah AhmadNo ratings yet
- Ten Traits of Great Physicians - 230228 - 085304Document6 pagesTen Traits of Great Physicians - 230228 - 085304lakshminivas PingaliNo ratings yet
- EKG Crash Course NuRsing 390 SMC - 4Document57 pagesEKG Crash Course NuRsing 390 SMC - 4m1k0e100% (2)
- Ed Facility Interview QuestionsDocument8 pagesEd Facility Interview QuestionsMouli learningNo ratings yet
- NCM 118 - Lesson 11 (Arrhythmia)Document5 pagesNCM 118 - Lesson 11 (Arrhythmia)Bobby Christian DuronNo ratings yet
- DefibrillatorsDocument54 pagesDefibrillatorsAli Al-AhmedyNo ratings yet
- Atrial Fibrillation - Classification, Pathophysiology, Mechanisms and Drug TreatmentDocument8 pagesAtrial Fibrillation - Classification, Pathophysiology, Mechanisms and Drug TreatmentLorentina Den PanjaitanNo ratings yet
- Hopkins Medicine Review Cardiology SectionDocument54 pagesHopkins Medicine Review Cardiology SectiondrsalilsidhqueNo ratings yet
































































































Download as pdf or txt
You might also like
- Complaint Emergency HandbookDocument306 pagesComplaint Emergency HandbookUsman Amjad100% (3)
- PALS Case Scenario Testing ChecklistDocument12 pagesPALS Case Scenario Testing ChecklistJohn David D. ErguizaNo ratings yet
- EKG Findings and Arrhythmias - USMLE Step 2 CK ExamDocument3 pagesEKG Findings and Arrhythmias - USMLE Step 2 CK ExamSamah Khan100% (2)
- ECG WorksheetDocument3 pagesECG WorksheetElaiza UyNo ratings yet
- ACLS For TachycardiaDocument31 pagesACLS For TachycardiaTausif HaqueNo ratings yet
- Atrial FibrillationDocument24 pagesAtrial FibrillationFani Butt50% (2)
- ABCDs During A Code Blue Response in An Adult PatientDocument23 pagesABCDs During A Code Blue Response in An Adult PatientChakra PuspitaNo ratings yet
- ACLS Appendix 3Document32 pagesACLS Appendix 3tostc100% (1)
- Acls - Megacode - UpdatedDocument4 pagesAcls - Megacode - UpdatedDivine Dela Pena100% (1)
- ACLS Pocket GuideDocument5 pagesACLS Pocket Guidedragnu100% (1)
- 1 Management of TachyarrythmiasDocument72 pages1 Management of TachyarrythmiassalsabeelNo ratings yet
- GINA-2023-Full-report-23_07_06-WMS (2)Document61 pagesGINA-2023-Full-report-23_07_06-WMS (2)Lamessa MessiNo ratings yet
- Arrhythmia NewDocument73 pagesArrhythmia Newlohith saiNo ratings yet
- Chapter - 036 Arrhythmias ClassDocument129 pagesChapter - 036 Arrhythmias ClassWisdomIsMiseryNo ratings yet
- Emergency in Medicine 2012Document202 pagesEmergency in Medicine 2012micheal1960No ratings yet
- Arrhythmia in Emergency 111Document21 pagesArrhythmia in Emergency 111Iyas JehadNo ratings yet
- Tachycardiafaez 161221035148Document36 pagesTachycardiafaez 161221035148hartanto_budi6222No ratings yet
- Cardiac Arrythmias in The ED Menbeu Edited From AnaDocument106 pagesCardiac Arrythmias in The ED Menbeu Edited From AnaTemesgen Geleta100% (1)
- Life Threatening Arrhythmia and ManagementDocument40 pagesLife Threatening Arrhythmia and ManagementRuki Hartawan100% (1)
- 28,29 Management of Cardiac ArrhythmiasDocument41 pages28,29 Management of Cardiac ArrhythmiasSL Dr ChEMiSNo ratings yet
- Atrial FibrillationDocument8 pagesAtrial FibrillationduhsknwsNo ratings yet
- Arrhythmia 6 YrDocument72 pagesArrhythmia 6 YrPiyush MalikNo ratings yet
- 41 Paediatric ArrhythmiasDocument4 pages41 Paediatric ArrhythmiasnasibdinNo ratings yet
- Arrhythmia, Pericardial and Myocardial Diseases (DR Praveen) 2Document44 pagesArrhythmia, Pericardial and Myocardial Diseases (DR Praveen) 2hashini1997nisansalaNo ratings yet
- Diagnosis Dan Tatalaksana Awal SVTDocument47 pagesDiagnosis Dan Tatalaksana Awal SVTZuly Vita AulyaNo ratings yet
- Tachy/賸)Document28 pagesTachy/賸)Jason LinNo ratings yet
- ARITMIADocument47 pagesARITMIASarah JR Nur AzizahNo ratings yet
- Arrhythmias: Sing Khien Tiong Gpst1Document34 pagesArrhythmias: Sing Khien Tiong Gpst1preethi preethaNo ratings yet
- ECG Dysrhthmias IIIDocument31 pagesECG Dysrhthmias IIIAmani Kayed100% (1)
- Atrial FibrillationDocument50 pagesAtrial Fibrillationvarun_swmNo ratings yet
- Atrial Fibrillation (AF)Document24 pagesAtrial Fibrillation (AF)farmasi_hm100% (1)
- 3881 - Prosedur Pendaftaran Internship Per November 2016Document57 pages3881 - Prosedur Pendaftaran Internship Per November 2016Munawir_Syam91No ratings yet
- IC1 - Arrhythmia - 2012 EDITEDDocument42 pagesIC1 - Arrhythmia - 2012 EDITEDrazorazNo ratings yet
- Workshop Pit IV THN 2017Document57 pagesWorkshop Pit IV THN 2017anettepardedeNo ratings yet
- Aritmia LetalDocument49 pagesAritmia LetalfebriyakNo ratings yet
- Atrial Fibrillation: Bibek Raj Poudel Intern Pahs-SomDocument34 pagesAtrial Fibrillation: Bibek Raj Poudel Intern Pahs-SomKishor K AdhikariNo ratings yet
- Ecg Class Atrial Fibrillation Power PointDocument21 pagesEcg Class Atrial Fibrillation Power PointRoshilNo ratings yet
- Atrial Fibrillation: Dr. Zirath + Dr. MehtaDocument29 pagesAtrial Fibrillation: Dr. Zirath + Dr. MehtaAjayNo ratings yet
- Atrial FibrillationDocument50 pagesAtrial Fibrillationkapil khanalNo ratings yet
- Curs Engl S Preexcit Corect Nic MPDocument72 pagesCurs Engl S Preexcit Corect Nic MPErland BordNo ratings yet
- A Fib in 60 Yr Old ManDocument32 pagesA Fib in 60 Yr Old ManNurul HikmahNo ratings yet
- Medicine Paper Number 1Document8 pagesMedicine Paper Number 1arvindNo ratings yet
- Supraventricular Tachycardia: Teresa Menendez Hood, MD FACCDocument39 pagesSupraventricular Tachycardia: Teresa Menendez Hood, MD FACCReinsy NoviNo ratings yet
- SVT PresentationDocument39 pagesSVT PresentationReinsy NoviNo ratings yet
- ArrhythmiasDocument48 pagesArrhythmiasHarshan JeyakumarNo ratings yet
- ATRIAL FIBRILLATION Anil KRDocument41 pagesATRIAL FIBRILLATION Anil KRanil sahNo ratings yet
- ArrhythmiasDocument53 pagesArrhythmiasabotreka056No ratings yet
- ECG Class ON VT PowerpointDocument24 pagesECG Class ON VT PowerpointRoshilNo ratings yet
- 5 ArrhythmiaDocument44 pages5 ArrhythmiaDanny DesuNo ratings yet
- Hippo EM Board Review - Bradycardia - A Simplified Approach Written Summary 2Document10 pagesHippo EM Board Review - Bradycardia - A Simplified Approach Written Summary 2alexandertorresreyNo ratings yet
- Cardiac ArrythmiaDocument16 pagesCardiac ArrythmiaHossen AliNo ratings yet
- Practice Essentials: Essential Updates: Distinguishing Between Left-And Right-Sided Atrial TachycardiaDocument28 pagesPractice Essentials: Essential Updates: Distinguishing Between Left-And Right-Sided Atrial TachycardiaRully SyahrizalNo ratings yet
- Cardiac Rhythm and Related Disorders: Marshell Tendean, MD Department of Internal Medicine UKRIDA JakartaDocument39 pagesCardiac Rhythm and Related Disorders: Marshell Tendean, MD Department of Internal Medicine UKRIDA JakartaFatimah Hartina FaradillahNo ratings yet
- Farmakologi Anti AritmiaDocument26 pagesFarmakologi Anti AritmiaAzzam nur TaufikurrahmanNo ratings yet
- Vdocument in Arrhythmia Diagnosis and Management محمد امريضDocument54 pagesVdocument in Arrhythmia Diagnosis and Management محمد امريضHelene AlawamiNo ratings yet
- Cardiac Arrhythmia 171209212142 2Document74 pagesCardiac Arrhythmia 171209212142 2Gunel Sadiqova100% (1)
- Cardiac Rhythm and Related Disorders: - Marshell Tendean, MD - Department of Internal Medicine UKRIDA JakartaDocument50 pagesCardiac Rhythm and Related Disorders: - Marshell Tendean, MD - Department of Internal Medicine UKRIDA JakartavaiyenNo ratings yet
- Atrial Fibrillation HandoutDocument5 pagesAtrial Fibrillation HandoutAlfa AlfinNo ratings yet
- Atrial FibrillationDocument1 pageAtrial FibrillationshakyaNo ratings yet
- ECG Symcard 2016 - Ventricular ArrhythmiaDocument41 pagesECG Symcard 2016 - Ventricular ArrhythmiaRadinal MauludiNo ratings yet
- Supplementary Material 4.3 Cardiac Rhythm Disorders-2Document14 pagesSupplementary Material 4.3 Cardiac Rhythm Disorders-2Andrea Love PalomoNo ratings yet
- Lecture2 3Document44 pagesLecture2 3Amanda HizerNo ratings yet
- Management of Cardiac ArrestDocument40 pagesManagement of Cardiac ArrestMark Francis NaniaNo ratings yet
- BradyarrthmiaDocument73 pagesBradyarrthmiaKuba ArebaNo ratings yet
- Donaldson_VT Diagnosis_TherapyDocument34 pagesDonaldson_VT Diagnosis_Therapygoldenday_hdpNo ratings yet
- Arrhythmias PDFDocument29 pagesArrhythmias PDFbencleeseNo ratings yet
- Approach To PalpitationsDocument74 pagesApproach To PalpitationsDarawan MirzaNo ratings yet
- Microsoft Word - Validation of Risk Score FPR Postoperative Nausea and Vomiting in Patients Undergoing General Anaesthesia at UTHDocument46 pagesMicrosoft Word - Validation of Risk Score FPR Postoperative Nausea and Vomiting in Patients Undergoing General Anaesthesia at UTHUWIMANA Jean ClaudeNo ratings yet
- OO Royal Mirage Coronavirus Management Plan - Master Plan WorkingDocument52 pagesOO Royal Mirage Coronavirus Management Plan - Master Plan WorkingUWIMANA Jean ClaudeNo ratings yet
- Volatile Costs Calculations ZORADocument11 pagesVolatile Costs Calculations ZORAUWIMANA Jean ClaudeNo ratings yet
- Gestational Hypertension and Preeclampsia ACOG.46Document24 pagesGestational Hypertension and Preeclampsia ACOG.46UWIMANA Jean ClaudeNo ratings yet
- CBM Scholarship Call For Applications 2021-2022Document3 pagesCBM Scholarship Call For Applications 2021-2022UWIMANA Jean ClaudeNo ratings yet
- Book 1Document93 pagesBook 1UWIMANA Jean ClaudeNo ratings yet
- Single Best Answer MCQs in Anaesthesia Volume II.14Document1 pageSingle Best Answer MCQs in Anaesthesia Volume II.14UWIMANA Jean ClaudeNo ratings yet
- PALS Nitty Gritty Study Guide FINALDocument11 pagesPALS Nitty Gritty Study Guide FINALuncmikee1997100% (1)
- Arrhythmia CBLDocument7 pagesArrhythmia CBLRyuuzakiDNNo ratings yet
- ACLS AgorithmDocument55 pagesACLS AgorithmkpsuanNo ratings yet
- 9 - Series 2022Document8 pages9 - Series 2022Vijay UNo ratings yet
- Quiz 35, 36, 37Document47 pagesQuiz 35, 36, 37dotleds100% (1)
- NP4 RECALLS5 AnswersDocument31 pagesNP4 RECALLS5 AnswersAhrisJeannine EscuadroNo ratings yet
- R Series Product ManualDocument186 pagesR Series Product ManualppdeepakNo ratings yet
- Basic ECG Interpretation MWDocument211 pagesBasic ECG Interpretation MWLorelie AsisNo ratings yet
- Resident Survival Guide: (Include Ranges of Any Abnormal Vital Signs But Also Include The Current Value For All Vitals.)Document104 pagesResident Survival Guide: (Include Ranges of Any Abnormal Vital Signs But Also Include The Current Value For All Vitals.)scalixto100% (1)
- DysrhythmiasDocument67 pagesDysrhythmiashhh hhhNo ratings yet
- EMS Agency Color Code Drug Doses L. L.A. County Kids: Normal Vital Signs PALS Drugs - Initial Dose MedicationDocument5 pagesEMS Agency Color Code Drug Doses L. L.A. County Kids: Normal Vital Signs PALS Drugs - Initial Dose MedicationCruz VerdeNo ratings yet
- Reanimacion CardiopulmonarDocument15 pagesReanimacion CardiopulmonarVictoriano ValienteNo ratings yet
- Ecg NotesDocument35 pagesEcg NotesDanielle100% (1)
- Cardiac Arrhythmia in Children PDFDocument50 pagesCardiac Arrhythmia in Children PDFNorhafizah AhmadNo ratings yet
- Ten Traits of Great Physicians - 230228 - 085304Document6 pagesTen Traits of Great Physicians - 230228 - 085304lakshminivas PingaliNo ratings yet
- EKG Crash Course NuRsing 390 SMC - 4Document57 pagesEKG Crash Course NuRsing 390 SMC - 4m1k0e100% (2)
- Ed Facility Interview QuestionsDocument8 pagesEd Facility Interview QuestionsMouli learningNo ratings yet
- NCM 118 - Lesson 11 (Arrhythmia)Document5 pagesNCM 118 - Lesson 11 (Arrhythmia)Bobby Christian DuronNo ratings yet
- DefibrillatorsDocument54 pagesDefibrillatorsAli Al-AhmedyNo ratings yet
- Atrial Fibrillation - Classification, Pathophysiology, Mechanisms and Drug TreatmentDocument8 pagesAtrial Fibrillation - Classification, Pathophysiology, Mechanisms and Drug TreatmentLorentina Den PanjaitanNo ratings yet
- Hopkins Medicine Review Cardiology SectionDocument54 pagesHopkins Medicine Review Cardiology SectiondrsalilsidhqueNo ratings yet