Download as pdf or txt
You might also like
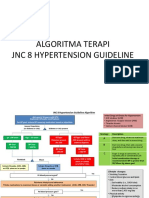
- Algoritma Terapi JNC 8 Hypertension GuidelineDocument3 pagesAlgoritma Terapi JNC 8 Hypertension GuidelineRhenty NarusNo ratings yet
- West Bengal - Hypertension ProtocolDocument1 pageWest Bengal - Hypertension ProtocolDebanjan Basak100% (1)
- Hypertension Guidelines PDFDocument10 pagesHypertension Guidelines PDFARAVINDANo ratings yet
- 2014 JNC 8 HypertensionDocument3 pages2014 JNC 8 HypertensionFernandez-De Ala NicaNo ratings yet
- Chapter 23: Drugs Used To Treat HypertensionDocument14 pagesChapter 23: Drugs Used To Treat HypertensionAziil LiizaNo ratings yet
- Clinical Practice Guideline For Adult Hypertension - Prevention, Screening, Counseling and ManagementDocument6 pagesClinical Practice Guideline For Adult Hypertension - Prevention, Screening, Counseling and ManagementHeppyMeiNo ratings yet
- Blood Pressure Clinician Guide KpcmiDocument11 pagesBlood Pressure Clinician Guide KpcmiMozes SimataaNo ratings yet
- Diabetes Kit HCP PocketDocument2 pagesDiabetes Kit HCP PocketjoepinoxNo ratings yet
- Guia Hipertension Viii 2014Document6 pagesGuia Hipertension Viii 2014Edgar G RoblesNo ratings yet
- 2014 Evidence-Based Guidelines For The Management of High Blood Pressure in AdultsDocument14 pages2014 Evidence-Based Guidelines For The Management of High Blood Pressure in AdultsAchmad HariyantoNo ratings yet
- HTN managment-JNC7Document37 pagesHTN managment-JNC7Vaibhav KaroliyaNo ratings yet
- Medical Management of Adults With Hypertension: Michigan Quality Improvement Consortium GuidelineDocument1 pageMedical Management of Adults With Hypertension: Michigan Quality Improvement Consortium GuidelinedennisNo ratings yet
- QTC Flow Diagram With Medications Final Dec 17 A3 With LogosDocument1 pageQTC Flow Diagram With Medications Final Dec 17 A3 With LogosMelissa MurilloNo ratings yet
- 6.Z8sNyP 6 GHafez HT and Antihypertensive DrugsDocument81 pages6.Z8sNyP 6 GHafez HT and Antihypertensive Drugsyasmin.rahmany03No ratings yet
- Kardiologi Klinik JNC 8Document62 pagesKardiologi Klinik JNC 8Adel Ciiy OcheNo ratings yet
- Assignment 1Document3 pagesAssignment 1SaulNo ratings yet
- 01 Chapter Hypertension32Document12 pages01 Chapter Hypertension32UtkarshNo ratings yet
- 01 Chapter Hypertension32Document12 pages01 Chapter Hypertension32ChristianNo ratings yet
- Stroke GuidelinesDocument49 pagesStroke Guidelinesxmc5505No ratings yet
- Hypertension Pocket Guide: Classification of Blood Pressure Levels For People 18 and OlderDocument2 pagesHypertension Pocket Guide: Classification of Blood Pressure Levels For People 18 and OlderMuhammad Mubeen Iqbal PuriNo ratings yet
- Management of HypertensionDocument67 pagesManagement of Hypertensionainzahir94No ratings yet
- Hypertension ManagementDocument13 pagesHypertension ManagementEjaz AhmedNo ratings yet
- The International Society of Hypertension Guidelines 2020 A New Drug Treatment Recommendation in The Wrong DirectionDocument4 pagesThe International Society of Hypertension Guidelines 2020 A New Drug Treatment Recommendation in The Wrong DirectionXylia TocaoNo ratings yet
- Rajasthan - Hypertension Protocol - 18 YearsDocument1 pageRajasthan - Hypertension Protocol - 18 YearsysjaitawatNo ratings yet
- HT During pandemic-PDUIDocument45 pagesHT During pandemic-PDUIVictor PratamaNo ratings yet
- COVID19 - DexamethasoneDocument2 pagesCOVID19 - DexamethasoneLe Hoang TuanNo ratings yet
- Hypertension AHA 2017Document28 pagesHypertension AHA 2017Iman SaksoukNo ratings yet
- Hypertension and Its Management: by Dr. UmairDocument20 pagesHypertension and Its Management: by Dr. UmairdockmsNo ratings yet
- Panduan Hipertensi JNC 8Document24 pagesPanduan Hipertensi JNC 8Joko RinantoNo ratings yet
- Guidelines TX of HPNDocument3 pagesGuidelines TX of HPNjheyfteeNo ratings yet
- JNC 8Document40 pagesJNC 8Nadira Wulandari100% (1)
- 1210 DIASTOLIC HypertensionDocument44 pages1210 DIASTOLIC HypertensionBoysz TheBestNo ratings yet
- COMMUNITY AssignmenDocument28 pagesCOMMUNITY AssignmenMunizah ArshadNo ratings yet
- Quartet TrialDocument23 pagesQuartet Trialapi-647244341No ratings yet
- CardiovascularDocument28 pagesCardiovascularFarhan AbdiNo ratings yet
- JNC 8 2014 Evidence-Based Guidelines For The Management of High Blood Pressure in AdultsDocument40 pagesJNC 8 2014 Evidence-Based Guidelines For The Management of High Blood Pressure in AdultsArum Nadia HafifiNo ratings yet
- HTA Resistente 2022Document12 pagesHTA Resistente 2022GilbertoNo ratings yet
- Hipertensi BPJS AsepDocument87 pagesHipertensi BPJS AsepAdrianus MedanNo ratings yet
- Prevention, Detection, Evaluation, and Management of High Blood Pressure in AdultsDocument30 pagesPrevention, Detection, Evaluation, and Management of High Blood Pressure in AdultsShazi AliNo ratings yet
- DR Philip Swales - GIM 22 MayDocument34 pagesDR Philip Swales - GIM 22 MaySathvika BNo ratings yet
- AMH Hypertension PrintDocument4 pagesAMH Hypertension PrintMusharaf RehmanNo ratings yet
- Hypertension Guidelines 2014: Jason A. Smith, DO Associated Cardiovascular Consultants at Lourdes Cardiology ServicesDocument33 pagesHypertension Guidelines 2014: Jason A. Smith, DO Associated Cardiovascular Consultants at Lourdes Cardiology ServicesRido MaulanaNo ratings yet
- General Population (No Diabetes or CKD) Diabetes or CKD PresentDocument2 pagesGeneral Population (No Diabetes or CKD) Diabetes or CKD PresentLalu Ranova100% (1)
- Review of New Hypertension Guidelines PDFDocument4 pagesReview of New Hypertension Guidelines PDFOsiithaa CañaszNo ratings yet
- Case Studies in Managing GG Hypertension: Defining The Barriers To ControlDocument37 pagesCase Studies in Managing GG Hypertension: Defining The Barriers To Controlkirubel deribNo ratings yet
- Greater Chennai - Hypertension Protocol - 18 YearsDocument1 pageGreater Chennai - Hypertension Protocol - 18 YearsSiaNo ratings yet
- 2 Algoritma HT JNC 8Document3 pages2 Algoritma HT JNC 8Nais MaghfirohNo ratings yet
- 2 Algoritma HT JNC 8Document3 pages2 Algoritma HT JNC 8Nais Maghfiroh100% (1)
- Literature-ReviewnDocument15 pagesLiterature-ReviewnAymn Mohammed AlaghbariNo ratings yet
- JNC 7 (Klasifikasi Hipertensi) PDFDocument2 pagesJNC 7 (Klasifikasi Hipertensi) PDFAbdur RahmanNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Medical Encyclopedia XXL: Prof. J.P. Schadé, M.D., Ph.D. D.Sc.hcFrom EverandMedical Encyclopedia XXL: Prof. J.P. Schadé, M.D., Ph.D. D.Sc.hcNo ratings yet
- A Simple Guide to Hypertension and Heart DiseasesFrom EverandA Simple Guide to Hypertension and Heart DiseasesRating: 5 out of 5 stars5/5 (1)
- DASH Diet for Beginners: The Ultimate Healthy Eating Solution and Weight Loss Program for Hypertension and Blood Pressure By Learning The Power of the DASH Diet!From EverandDASH Diet for Beginners: The Ultimate Healthy Eating Solution and Weight Loss Program for Hypertension and Blood Pressure By Learning The Power of the DASH Diet!No ratings yet
- The Ideal Prediabetes Diet Cookbook; The Super Diet Guide To Lose Weight, Manage And Reverse Prediabetes With Nutritious RecipesFrom EverandThe Ideal Prediabetes Diet Cookbook; The Super Diet Guide To Lose Weight, Manage And Reverse Prediabetes With Nutritious RecipesNo ratings yet
- EmphysemaDocument44 pagesEmphysematheonlinegeekhubNo ratings yet
- Anti Viral Drugs-IntroductionDocument79 pagesAnti Viral Drugs-IntroductiontheonlinegeekhubNo ratings yet
- DIARRHEAL INFECTIONS TableDocument8 pagesDIARRHEAL INFECTIONS TabletheonlinegeekhubNo ratings yet
- Shock Wps OfficeDocument2 pagesShock Wps OfficetheonlinegeekhubNo ratings yet
- Human PsychologyDocument58 pagesHuman PsychologytheonlinegeekhubNo ratings yet
- 2.0 FungiDocument13 pages2.0 FungitheonlinegeekhubNo ratings yet
- Severe MalnutritionDocument12 pagesSevere MalnutritiontheonlinegeekhubNo ratings yet
- 1.3 Peripheral Nervous SystemDocument116 pages1.3 Peripheral Nervous SystemtheonlinegeekhubNo ratings yet
- PulmonaryDocument54 pagesPulmonarytheonlinegeekhubNo ratings yet
- Inflammation 1Document98 pagesInflammation 1theonlinegeekhubNo ratings yet
- ObesityDocument28 pagesObesitytheonlinegeekhubNo ratings yet
- 7 GangreneDocument43 pages7 GangrenetheonlinegeekhubNo ratings yet
- A Skeletal System - Appendicular SkeletonDocument66 pagesA Skeletal System - Appendicular SkeletontheonlinegeekhubNo ratings yet
- 638366076b152 KMTC Pathology BateriologyDocument8 pages638366076b152 KMTC Pathology BateriologytheonlinegeekhubNo ratings yet
- 2-Skin Conditions - BurnsDocument58 pages2-Skin Conditions - BurnstheonlinegeekhubNo ratings yet
- Spinal InjuryDocument2 pagesSpinal InjurytheonlinegeekhubNo ratings yet
- 002a1 - Concepts in General PathologyDocument38 pages002a1 - Concepts in General PathologytheonlinegeekhubNo ratings yet
- The Central Nervous SystemDocument83 pagesThe Central Nervous SystemtheonlinegeekhubNo ratings yet
- 633805750b2a1 Introduction To The Circulatory System ConsolidatedDocument173 pages633805750b2a1 Introduction To The Circulatory System ConsolidatedtheonlinegeekhubNo ratings yet
- History of MicrobiologyDocument7 pagesHistory of MicrobiologytheonlinegeekhubNo ratings yet
- A. Female Reproductive SystemDocument70 pagesA. Female Reproductive SystemtheonlinegeekhubNo ratings yet
- Gestational Trophoblastic DiseasesDocument36 pagesGestational Trophoblastic DiseasestheonlinegeekhubNo ratings yet
- Cardiovascular SystemDocument71 pagesCardiovascular SystemtheonlinegeekhubNo ratings yet
- 5 - The Concept of Communication Skills in MedicineDocument33 pages5 - The Concept of Communication Skills in MedicinetheonlinegeekhubNo ratings yet
- Clinical Methods General Exam 1Document57 pagesClinical Methods General Exam 1theonlinegeekhubNo ratings yet
- Vital StatisticsDocument13 pagesVital StatisticstheonlinegeekhubNo ratings yet
- Importance of Studying MicrobiologyDocument20 pagesImportance of Studying MicrobiologytheonlinegeekhubNo ratings yet
- Special Senses Ii Auditory SysyemDocument25 pagesSpecial Senses Ii Auditory SysyemtheonlinegeekhubNo ratings yet
- 1 Introduction To ParasitologyDocument24 pages1 Introduction To ParasitologytheonlinegeekhubNo ratings yet
- Dr. AsifDocument30 pagesDr. AsifUsman DastgirNo ratings yet
- Cardiac BiomarkersDocument45 pagesCardiac BiomarkersishratrNo ratings yet
- Jamacardiology Zhang 2021 Oi 210061 1630597090.4739Document8 pagesJamacardiology Zhang 2021 Oi 210061 1630597090.4739AlizaPinkyNo ratings yet
- Heart Failure: Abdul Hafiz AliasDocument19 pagesHeart Failure: Abdul Hafiz AliasAbdul Hafiz Alias100% (5)
- HF2019Document24 pagesHF2019Sima Noviantika100% (2)
- Disorders of The Circulatory System Table-AnswersDocument2 pagesDisorders of The Circulatory System Table-Answersapi-281108263No ratings yet
- Lymphocyte TraffickingDocument8 pagesLymphocyte TraffickingAbhishek KumarNo ratings yet
- Diferential Diagnosis in Internal Medicine 20879 PDFDocument448 pagesDiferential Diagnosis in Internal Medicine 20879 PDFMarcel Cegodar100% (2)
- Hridroga: Dr. Mahesh C KundagolDocument53 pagesHridroga: Dr. Mahesh C Kundagolkundagol100% (1)
- Cardio Vascular System of Prawn.Document3 pagesCardio Vascular System of Prawn.Roy AronNo ratings yet
- Thesis Statement For Research Paper On Heart DiseaseDocument7 pagesThesis Statement For Research Paper On Heart DiseaseafnhinzugpbcgwNo ratings yet
- Manual of Cardiovascular Medicine Thomas Luscher Full ChapterDocument67 pagesManual of Cardiovascular Medicine Thomas Luscher Full Chapterdarlene.silverthorn708100% (8)
- Bailey JMDocument9 pagesBailey JMPedro VillamorNo ratings yet
- Cardiac Cycle Electrical Mechanical EventsDocument49 pagesCardiac Cycle Electrical Mechanical EventsJardee Datsima100% (1)
- CentralVenousCatheter CVCDocument41 pagesCentralVenousCatheter CVCPraveen RavishankaranNo ratings yet
- Pathophysiology of Pericardial DiseaseDocument36 pagesPathophysiology of Pericardial DiseaseivaniNo ratings yet
- EtiologyDocument3 pagesEtiologyVanessa Yvonne GurtizaNo ratings yet
- What Is Extracorporeal Cardiopulmonary Resuscitation?: Federico Pappalardo, Andrea MontisciDocument5 pagesWhat Is Extracorporeal Cardiopulmonary Resuscitation?: Federico Pappalardo, Andrea MontisciPrajogo KusumaNo ratings yet
- Cardiac ArrestDocument7 pagesCardiac ArrestDiana MuañaNo ratings yet
- 2018 ESC-ESH Guidelines For The Management of Arterial HypertensionDocument98 pages2018 ESC-ESH Guidelines For The Management of Arterial HypertensionjulzcatNo ratings yet
- Guias Europeas TEP 2019Document61 pagesGuias Europeas TEP 2019Sebastian PosadaNo ratings yet
- Acute Pericarditis PDFDocument14 pagesAcute Pericarditis PDFMila CcasaniNo ratings yet
- Computer Methods and Programs in Biomedicine: Iqra Shahzadi, S. BilalDocument11 pagesComputer Methods and Programs in Biomedicine: Iqra Shahzadi, S. Bilalp ppNo ratings yet
- SSC 8 Blood Pressure (High) CombinationDocument1 pageSSC 8 Blood Pressure (High) CombinationhimaNo ratings yet
- Cardio DrugsDocument58 pagesCardio DrugsMARIA ROWENA VIA J. LUCENANo ratings yet
- Echo Cardiograph yDocument3 pagesEcho Cardiograph yJisha JanardhanNo ratings yet
- Cardiac Muscle PropertiesDocument4 pagesCardiac Muscle PropertiesSurpreet AroraNo ratings yet
- Pharmacology For Oral RecitDocument16 pagesPharmacology For Oral RecitAngel DiangNo ratings yet
- Diacan ProDocument3 pagesDiacan Proagnes wulandariNo ratings yet
- CHD DDocument47 pagesCHD Dmy Lord JesusNo ratings yet