Download as pdf or txt
You might also like
- American Red CrossDocument484 pagesAmerican Red CrossAngelika LowderNo ratings yet
- Claim Form GeneralDocument1 pageClaim Form GeneralTanya Rose-AppleNo ratings yet
- Form - Bupa Claim FormDocument2 pagesForm - Bupa Claim FormJoe Sayavongsa100% (3)
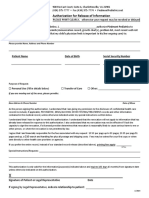
- Authorization For Release of Medical Information BSWHDocument1 pageAuthorization For Release of Medical Information BSWHCarrie FullerNo ratings yet
- Prior Authorization Request FormDocument3 pagesPrior Authorization Request FormvanessaNo ratings yet
- Group Death - Attending Physician's StatementDocument2 pagesGroup Death - Attending Physician's StatementJohn Victor Perez OretoNo ratings yet
- DEA Psilocybin LawsuitDocument15 pagesDEA Psilocybin LawsuitMarijuana MomentNo ratings yet
- Form HA-4631Document2 pagesForm HA-4631GARY SELLSNo ratings yet
- Medical Records Release Partners English PDFDocument2 pagesMedical Records Release Partners English PDFBobbie StJohnNo ratings yet
- CMS20027 0Document1 pageCMS20027 0suasponte2No ratings yet
- FACS ReferralDocument2 pagesFACS Referralsandhupriya1998No ratings yet
- Fort Lyon Referral Application - 2021Document13 pagesFort Lyon Referral Application - 2021carrerasjaxxxNo ratings yet
- East FL HIPAA Authorization FormDocument2 pagesEast FL HIPAA Authorization Formfelix ariasNo ratings yet
- Bupa Global Claim FormDocument8 pagesBupa Global Claim FormALJABERNo ratings yet
- MRRF 11.10.2020Document2 pagesMRRF 11.10.2020oijewNo ratings yet
- Roi PDFDocument4 pagesRoi PDFKNo ratings yet
- Molina FormDocument2 pagesMolina FormscorreaNo ratings yet
- Facesheets 3 - 9 - 21Document4 pagesFacesheets 3 - 9 - 21Rahul ManiNo ratings yet
- Mississippi State Board of Medical Licensure: Complaint FormDocument5 pagesMississippi State Board of Medical Licensure: Complaint FormScott SistersNo ratings yet
- ROI FormDocument3 pagesROI FormKaden MaysNo ratings yet
- Patient Authorization PDFDocument2 pagesPatient Authorization PDFTanessa WilliamsNo ratings yet
- JUUL Medical Authorization Packet - Tarek WegDocument4 pagesJUUL Medical Authorization Packet - Tarek WegTed RustNo ratings yet
- Release of Info UMDocument1 pageRelease of Info UMsalmapratyushNo ratings yet
- Asian Pacific Development Center: Authorization To Release/Request For InformationDocument2 pagesAsian Pacific Development Center: Authorization To Release/Request For InformationchristinasteenhoekNo ratings yet
- VA - Form - 10-5345 - FillableDocument2 pagesVA - Form - 10-5345 - Fillablep1nguin0No ratings yet
- Request For Information FormDocument2 pagesRequest For Information FormHandi FerryandiNo ratings yet
- JFR Claim Form Leonardo PreenchidoDocument3 pagesJFR Claim Form Leonardo PreenchidoNatália André RodriguesNo ratings yet
- PA For ChiroDocument1 pagePA For Chiroyjj856765No ratings yet
- Authorization For Release of Medical InformationDocument1 pageAuthorization For Release of Medical Informationcig3fNo ratings yet
- Patient Access Request - CostcoDocument1 pagePatient Access Request - Costcocorey SgarsNo ratings yet
- CMS20033Document1 pageCMS20033Arun YadavNo ratings yet
- Chola Health Claim FormDocument2 pagesChola Health Claim FormBalaji_Rajaman_2280No ratings yet
- AuthtoDiscloseProtectedPHI NH 900010Document1 pageAuthtoDiscloseProtectedPHI NH 900010brooklynlowe24No ratings yet
- CG-719K - Final Draft To Vendor - 14jun12Document8 pagesCG-719K - Final Draft To Vendor - 14jun12danNo ratings yet
- #58+Authorization+to+Obtain-Release+InfoDocument1 page#58+Authorization+to+Obtain-Release+Infoellen4109No ratings yet
- Isp 2502 ADocument2 pagesIsp 2502 ASNo ratings yet
- RequesttosendmedrecsDocument1 pageRequesttosendmedrecsNiko SalinasNo ratings yet
- Iiisla Benevolent Fund (Ibf) : Claim FormDocument2 pagesIiisla Benevolent Fund (Ibf) : Claim FormSachin PrajapatiNo ratings yet
- If HP Maid Combined Assessor Provider Form ElectronicDocument10 pagesIf HP Maid Combined Assessor Provider Form ElectronicdawnNo ratings yet
- Claim Form: 1 Patient's DetailsDocument7 pagesClaim Form: 1 Patient's DetailsEduskill Learning CentreNo ratings yet
- BAH Bupa Global Claim Form EN APR21 0027975Document8 pagesBAH Bupa Global Claim Form EN APR21 0027975ALJABERNo ratings yet
- START Form EnglishDocument2 pagesSTART Form EnglishkranthikumarimmadiNo ratings yet
- 10 7959f 2 Fill - 012317Document2 pages10 7959f 2 Fill - 012317Princess Mae JaneaNo ratings yet
- 10 7959f 2 Fill - 012317Document2 pages10 7959f 2 Fill - 012317Princess Mae JaneaNo ratings yet
- 3497 FilDocument2 pages3497 Filirenemariehansen7No ratings yet
- LTC Renewal PDFDocument12 pagesLTC Renewal PDFVashisth SoniNo ratings yet
- Axa Reimbursement Claim Form 01Document2 pagesAxa Reimbursement Claim Form 01Tarak FakhfakhNo ratings yet
- BINS Bupa Global Claim Form en 2005 21089Document8 pagesBINS Bupa Global Claim Form en 2005 21089R.Pearlsis SophiNo ratings yet
- AXA Reimbursement Claim FormDocument2 pagesAXA Reimbursement Claim Formrajkamal eshwarNo ratings yet
- Authorization For Release of Information FormDocument2 pagesAuthorization For Release of Information FormWGMENo ratings yet
- Subject Access Revised Application Form 26032018Document6 pagesSubject Access Revised Application Form 26032018Lynn Ross WardNo ratings yet
- Medical Claims Authorisation Form (Single Institution) : A - Particulars of PatientDocument2 pagesMedical Claims Authorisation Form (Single Institution) : A - Particulars of PatientArthur YeungNo ratings yet
- GRS Request and Inquiry FormDocument1 pageGRS Request and Inquiry FormJenecile ParambitaNo ratings yet
- Form BUPADocument4 pagesForm BUPAterusunduhNo ratings yet
- 20210308-0043-B Lur No.: Laboratory / Radiology / Ultrasound Request FormDocument1 page20210308-0043-B Lur No.: Laboratory / Radiology / Ultrasound Request FormMarvin VerdadNo ratings yet
- New Appointment Request Form: For Emergent Requests: Please Contact The Appropriate On Call Provider at (206) 987-7777Document1 pageNew Appointment Request Form: For Emergent Requests: Please Contact The Appropriate On Call Provider at (206) 987-7777ghoshtapan4321No ratings yet
- VHA Form 10-5345a Fill-Revision 07.2021 HIGHLIGHTEDDocument1 pageVHA Form 10-5345a Fill-Revision 07.2021 HIGHLIGHTEDThe B-keepers Documentation ServicesNo ratings yet
- Cross-Training: The Medical Assistant WorkbookFrom EverandCross-Training: The Medical Assistant WorkbookNo ratings yet
- One Step Med: General Medical Information Record Keeping ManualFrom EverandOne Step Med: General Medical Information Record Keeping ManualNo ratings yet
- The Vaccine Court: The Dark Truth of America's Vaccine Injury Compensation ProgramFrom EverandThe Vaccine Court: The Dark Truth of America's Vaccine Injury Compensation ProgramRating: 5 out of 5 stars5/5 (2)
- The Constitutional Case for Religious Exemptions from Federal Vaccine MandatesFrom EverandThe Constitutional Case for Religious Exemptions from Federal Vaccine MandatesNo ratings yet
- TASUED - EduTAMSDocument1 pageTASUED - EduTAMSteresabrandt87No ratings yet
- TASUED - EduTAMSDocument1 pageTASUED - EduTAMSteresabrandt87No ratings yet
- Moniepoint Document 2024-03-23T11 45Document1 pageMoniepoint Document 2024-03-23T11 45teresabrandt87No ratings yet
- Politicalsystemsinpre ColonialandcolonialerasDocument18 pagesPoliticalsystemsinpre Colonialandcolonialerasteresabrandt87No ratings yet
- TASUED - EduTAMSDocument1 pageTASUED - EduTAMSteresabrandt87No ratings yet
- Lingual OrthodonticsDocument36 pagesLingual OrthodonticsRajshekhar BanerjeeNo ratings yet
- Spontaneous Swallowing Frequency in Post-Stroke Patients With and Without Oropharyngeal Dysphagia - An Observational StudyDocument11 pagesSpontaneous Swallowing Frequency in Post-Stroke Patients With and Without Oropharyngeal Dysphagia - An Observational StudyAlvina RusliNo ratings yet
- Flyer SV300 - S (2) - 1Document2 pagesFlyer SV300 - S (2) - 1Abo MaramNo ratings yet
- Awareness Program: Saaketh Sai Legal Services Committee 24 March 2022Document2 pagesAwareness Program: Saaketh Sai Legal Services Committee 24 March 2022saaketh saiNo ratings yet
- Draft Reflection Paper Markers Used Quantitative Qualitative Analysis Herbal Medicinal Products - enDocument6 pagesDraft Reflection Paper Markers Used Quantitative Qualitative Analysis Herbal Medicinal Products - enAshy CooperNo ratings yet
- RC High Efficiency Leucocyte Removal Filter: For Blood TransfusionDocument2 pagesRC High Efficiency Leucocyte Removal Filter: For Blood TransfusionSamir DerriNo ratings yet
- FACE PckeDocument4 pagesFACE PckeSamiksha SarafNo ratings yet
- Weeks 1-3 - Windshield Assessment TemplateDocument17 pagesWeeks 1-3 - Windshield Assessment TemplateQazim Raza50% (2)
- Project Proposal For Blood DonationDocument3 pagesProject Proposal For Blood DonationShayne Cabotaje Delos Santos - Borling100% (1)
- CCO System - Introduction 2Document128 pagesCCO System - Introduction 2Adriana FalconNo ratings yet
- Development of A New Wound Assessment FormDocument7 pagesDevelopment of A New Wound Assessment FormchristoNo ratings yet
- EnemaDocument48 pagesEnemaPrajna TiwariNo ratings yet
- Hubungan Pengetahuan Dan Sikap Perawat Dengan Penatalaksanaan Pembidaian Pasien Fraktur Di RS X Sulawesi TenggaraDocument8 pagesHubungan Pengetahuan Dan Sikap Perawat Dengan Penatalaksanaan Pembidaian Pasien Fraktur Di RS X Sulawesi TenggaraAnes AdestiNo ratings yet
- Route of Drug AdministrationDocument15 pagesRoute of Drug AdministrationKHaN IMaJNo ratings yet
- WINS IEC MaterialsDocument17 pagesWINS IEC MaterialsShirley R. CortezNo ratings yet
- Honorhealth Scottsdale Shea Medical Center: Campus MapDocument1 pageHonorhealth Scottsdale Shea Medical Center: Campus MapFEALABREPORTSNo ratings yet
- Sustaining Quality of Healthcare: Institutionalization of Quality AssuranceDocument60 pagesSustaining Quality of Healthcare: Institutionalization of Quality AssuranceMike TeeNo ratings yet
- Notice Under Section 80, Code 0F Civil Procedure Against Public OfficerDocument4 pagesNotice Under Section 80, Code 0F Civil Procedure Against Public OfficerAditi TNo ratings yet
- Ăß°è ÀΠ¿ë PDFDocument183 pagesĂß°è ÀΠ¿ë PDFhuyenthanh1807No ratings yet
- Medical Services Recruitment Board (MRB)Document22 pagesMedical Services Recruitment Board (MRB)jocky yNo ratings yet
- Doctor Route - Format - AnirbanDocument55 pagesDoctor Route - Format - AnirbanSoumya BanerjeeNo ratings yet
- Tissue Expansion: Grabb & Smith Plastic Surgery 2007Document38 pagesTissue Expansion: Grabb & Smith Plastic Surgery 2007Ramy AbedalazizeNo ratings yet
- CertificateDocument1 pageCertificateZainab KhanNo ratings yet
- Cagayan State University - Lasam Campus Campus Student CouncilDocument4 pagesCagayan State University - Lasam Campus Campus Student CouncilPerla BautistaNo ratings yet
- A Guide For FetotomyDocument4 pagesA Guide For FetotomydancerspazzNo ratings yet
- Sagpat WomenDocument21 pagesSagpat Womenquimwell arcadioNo ratings yet
- Head Circumference-For-Age BOYS: Birth To 5 Years (Percentiles)Document1 pageHead Circumference-For-Age BOYS: Birth To 5 Years (Percentiles)Prathamesh KannaNo ratings yet
- Performing Pulse Oximetry (Pulse Ox) With The Infant Patient: Education For ProvidersDocument1 pagePerforming Pulse Oximetry (Pulse Ox) With The Infant Patient: Education For ProvidersHassan KhanNo ratings yet
- pdfR2Document15 pagespdfR2నా పూకులో సనాతన ధర్మంNo ratings yet