Download as pdf or txt
You might also like
- Normas NES M1019Document12 pagesNormas NES M1019Margarita Torres FloresNo ratings yet
- Jolly Grammar Programme P1-6Document8 pagesJolly Grammar Programme P1-6Mandy Whorlow100% (3)
- Chapter 6 StressDocument9 pagesChapter 6 StressSiti Sarah Zalikha Binti Umar BakiNo ratings yet
- Remembering, Bartlett (1932)Document11 pagesRemembering, Bartlett (1932)andreea4etc100% (1)
- The Civil War - The Universe of War (Episode 5)Document5 pagesThe Civil War - The Universe of War (Episode 5)ShreyaNo ratings yet
- English ReaderDocument10 pagesEnglish ReaderMadhurima BanothNo ratings yet
- Extracorporeal Life Support in Pediatric Cardiac DysfunctionDocument5 pagesExtracorporeal Life Support in Pediatric Cardiac DysfunctionNoor Aida AriyaniNo ratings yet
- 1 s2.0 S0929664608602041 MainDocument9 pages1 s2.0 S0929664608602041 MainEko SiswantoNo ratings yet
- Pulmonary Atresia, Ventricular Septal Defect, and MAPCAs, Neonate Rehab On PADocument7 pagesPulmonary Atresia, Ventricular Septal Defect, and MAPCAs, Neonate Rehab On PAdinaNo ratings yet
- Korean QX Total Pulm Veins 2010Document5 pagesKorean QX Total Pulm Veins 2010Dr. LicónNo ratings yet
- Short - and Long-Term Outcomes at A Single InstitutionDocument7 pagesShort - and Long-Term Outcomes at A Single InstitutionJonathan Frimpong AnsahNo ratings yet
- Modelo 2Document5 pagesModelo 2kodagaNo ratings yet
- Estudio de Endarterectomía CarotídeaDocument9 pagesEstudio de Endarterectomía CarotídeaErnest Pardo RubioNo ratings yet
- JCTVS Myxo Ring Clinical Trial 2008Document9 pagesJCTVS Myxo Ring Clinical Trial 2008Nalini RajamannanNo ratings yet
- The Perioperative Complication Rate of Orthopedic PDFDocument10 pagesThe Perioperative Complication Rate of Orthopedic PDFAnh Nguyen HuuNo ratings yet
- The Bentall Procedure: Is It The Gold Standard? A Series of 597 Consecutive CasesDocument7 pagesThe Bentall Procedure: Is It The Gold Standard? A Series of 597 Consecutive CaseskodagaNo ratings yet
- Outcome After Repair of Tetralogy of Fallot in The First Year of LifeDocument7 pagesOutcome After Repair of Tetralogy of Fallot in The First Year of LifeRadioputro WicaksonoNo ratings yet
- 1 s2.0 S0735109713030854 Main - 1Document7 pages1 s2.0 S0735109713030854 Main - 1Waleed Ismail KamelNo ratings yet
- Carotid StentDocument9 pagesCarotid StentCut FadmalaNo ratings yet
- Predictor Mortality EVARDocument7 pagesPredictor Mortality EVARAnneSaputraNo ratings yet
- New England Journal Medicine: The ofDocument9 pagesNew England Journal Medicine: The ofHesbon MomanyiNo ratings yet
- Endocarditis in The Elderly: Clinical, Echocardiographic, and Prognostic FeaturesDocument8 pagesEndocarditis in The Elderly: Clinical, Echocardiographic, and Prognostic FeaturesMehdi285858No ratings yet
- Safety and Ef Ficacy of An Endovascular-First Approach To Acute Limb IschemiaDocument9 pagesSafety and Ef Ficacy of An Endovascular-First Approach To Acute Limb IschemiaSisca Dwi AgustinaNo ratings yet
- Endovascular Stentgraft Placement in Aortic Dissection A MetaanalysisDocument10 pagesEndovascular Stentgraft Placement in Aortic Dissection A MetaanalysisCiubuc AndrianNo ratings yet
- The Features of ECG and Echocg Functional Parameters in Children With Congenital Heart Disease in The Postoperative PeriodDocument5 pagesThe Features of ECG and Echocg Functional Parameters in Children With Congenital Heart Disease in The Postoperative PeriodCentral Asian StudiesNo ratings yet
- Concomitant Bentall Operation Plus Aortic Arch Replacement SurgeryDocument7 pagesConcomitant Bentall Operation Plus Aortic Arch Replacement Surgeryprofarmah6150No ratings yet
- Jcs 55 2 158Document10 pagesJcs 55 2 158juajimenez55No ratings yet
- Bernard D. Prendergast and Pilar Tornos: Surgery For Infective Endocarditis: Who and When?Document26 pagesBernard D. Prendergast and Pilar Tornos: Surgery For Infective Endocarditis: Who and When?om mkNo ratings yet
- Cardiac Autotransplantation: Cooley Society 15th International SymposiumDocument5 pagesCardiac Autotransplantation: Cooley Society 15th International SymposiumPeter Paul PascualNo ratings yet
- Lan 2010Document6 pagesLan 2010FarhanNo ratings yet
- Efficacy of TTK Chitra Mechanical Heart Valve Versus ST Jude Mechanical Heart Valve in Aortic Valve ReplacementDocument7 pagesEfficacy of TTK Chitra Mechanical Heart Valve Versus ST Jude Mechanical Heart Valve in Aortic Valve ReplacementIJAR JOURNALNo ratings yet
- The Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open ReconstructionDocument10 pagesThe Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open ReconstructionRobert ChristevenNo ratings yet
- The Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open ReconstructionDocument10 pagesThe Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open Reconstructiontmarrero00No ratings yet
- Study 3Document7 pagesStudy 3OstazNo ratings yet
- The Impact of Dominant Ventricular Morphology On The Early Postoperative Course After The Glenn ProcedureDocument7 pagesThe Impact of Dominant Ventricular Morphology On The Early Postoperative Course After The Glenn ProcedureEitan KeizmanNo ratings yet
- Risk Model DialysiddssssDocument7 pagesRisk Model DialysiddssssDumitru GrozaNo ratings yet
- 2000 - Stamm Et Al. - Surgery For Bilateral Outflow Tract Obstruction in Elastin ArteriopathyDocument9 pages2000 - Stamm Et Al. - Surgery For Bilateral Outflow Tract Obstruction in Elastin ArteriopathybanupluNo ratings yet
- Tga Lagi PDFDocument4 pagesTga Lagi PDFMYMANo ratings yet
- Ultrasound diagnosis and management of acquired uterine enhanced myometrial vascularity-arteriovenous malformationsDocument10 pagesUltrasound diagnosis and management of acquired uterine enhanced myometrial vascularity-arteriovenous malformationsgersongc257No ratings yet
- 8-3-353Document6 pages8-3-353houmaishag77No ratings yet
- Percutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaDocument6 pagesPercutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaCotaga IgorNo ratings yet
- Mitral Valve Reconstruction in A Pediatric Population: Late Clinical Results and Predictors of Long-Term OutcomeDocument8 pagesMitral Valve Reconstruction in A Pediatric Population: Late Clinical Results and Predictors of Long-Term OutcomeAkaon NguyễnNo ratings yet
- Jurnal HDDocument6 pagesJurnal HDAdi SuciptoNo ratings yet
- Management of Thoracic Trauma: Experience at Ayub Teaching Hospital, AbbottabadDocument3 pagesManagement of Thoracic Trauma: Experience at Ayub Teaching Hospital, AbbottabadputridwierlindaNo ratings yet
- C2 U5 Williams Et Al Critical Care Clinics 2013Document32 pagesC2 U5 Williams Et Al Critical Care Clinics 2013Diego CrucesNo ratings yet
- Aortic Valve Bypass: Experience From Denmark: Original Article - Adult CardiacDocument5 pagesAortic Valve Bypass: Experience From Denmark: Original Article - Adult CardiacmoplkiNo ratings yet
- Long-Term Survival After Open Repair of Chronic Distal Aortic DissectionDocument9 pagesLong-Term Survival After Open Repair of Chronic Distal Aortic Dissectionapi-160333876No ratings yet
- Usefulness of Stent Implantation For Treatment ofDocument19 pagesUsefulness of Stent Implantation For Treatment ofAngel YapNo ratings yet
- Duplex Guided Balloon Angioplasty and Subintimal DDocument8 pagesDuplex Guided Balloon Angioplasty and Subintimal DJose PiulatsNo ratings yet
- Lemus Rangel 2010Document2 pagesLemus Rangel 2010audiNo ratings yet
- Percutaneous Aortic Valve Implantation: The Anesthesiologist PerspectiveDocument11 pagesPercutaneous Aortic Valve Implantation: The Anesthesiologist Perspectiveserena7205No ratings yet
- Short-And Long-Term Outcomes of Acute Upper Extremity Arterial ThromboembolismDocument4 pagesShort-And Long-Term Outcomes of Acute Upper Extremity Arterial ThromboembolismWilhelm HeinleinNo ratings yet
- Nej M Abbotts TentDocument11 pagesNej M Abbotts TentWKYC.comNo ratings yet
- Midterm Outcomes of Minimally Invasive Mitral Valve Surgery in A Heterogeneous Valve Pathology Cohort: Respect or Resect?Document12 pagesMidterm Outcomes of Minimally Invasive Mitral Valve Surgery in A Heterogeneous Valve Pathology Cohort: Respect or Resect?mony saNo ratings yet
- Pi Is 0022522312015267Document9 pagesPi Is 0022522312015267Riani NazilaNo ratings yet
- Guru 2006Document8 pagesGuru 2006Ahmad AlzawahrehNo ratings yet
- Extracorporeal Membrane Oxygenation Bridge To Adult Heart TransplantationDocument6 pagesExtracorporeal Membrane Oxygenation Bridge To Adult Heart TransplantationОлег ПоздняковNo ratings yet
- PIIS1078588419310755Document7 pagesPIIS1078588419310755zeeshan qurbanNo ratings yet
- Aortic Valve Stenosis - Curr. View On Diagnostics, TRTMT - P. Santavy (Intech, 2011) WWDocument156 pagesAortic Valve Stenosis - Curr. View On Diagnostics, TRTMT - P. Santavy (Intech, 2011) WWAnca AndronicNo ratings yet
- CVS Risk DterimantDocument1 pageCVS Risk DterimantAdel SALLAMNo ratings yet
- 2D 3D TEE Transcatheter Guiding With LAA ThrombusDocument16 pages2D 3D TEE Transcatheter Guiding With LAA ThrombusBosman AriestaNo ratings yet
- Ebrahim 2021Document8 pagesEbrahim 2021wiyay34652ceoshubcomNo ratings yet
- 1 s2.0 S0022522319323566 MainDocument10 pages1 s2.0 S0022522319323566 MainWaleed Ismail KamelNo ratings yet
- Loxdale 2011Document4 pagesLoxdale 2011Thadeu MáximoNo ratings yet
- Hepatic TraumaDocument7 pagesHepatic TraumaRoberto OrtizNo ratings yet
- Critical Care for Potential Liver Transplant CandidatesFrom EverandCritical Care for Potential Liver Transplant CandidatesDmitri BezinoverNo ratings yet
- Frs Whatsapp Chat NotesDocument72 pagesFrs Whatsapp Chat NotesFarai NyaniNo ratings yet
- Dissertation Topics in HindiDocument7 pagesDissertation Topics in HindiPaperWritingCompanyBillings100% (1)
- Direct BriberyDocument4 pagesDirect Briberyjuillien isiderioNo ratings yet
- Internet Banking Java Project ReportDocument68 pagesInternet Banking Java Project ReportKUMAR NILESH100% (1)
- GAS ModelDocument3 pagesGAS ModelDibyendu ShilNo ratings yet
- UNIT 3 Part 1-Propositional LogicDocument11 pagesUNIT 3 Part 1-Propositional LogicVanshika ChauhanNo ratings yet
- Gentrification in Color and TimeDocument38 pagesGentrification in Color and TimeBNo ratings yet
- List Peserta Swab Antigen - 5 Juni 2021Document11 pagesList Peserta Swab Antigen - 5 Juni 2021minhyun hwangNo ratings yet
- CreamsDocument17 pagesCreamsSolomonNo ratings yet
- DS Masteri An PhuDocument174 pagesDS Masteri An PhuPhong PhuNo ratings yet
- Ia 2 Compilation of Quiz and ExercisesDocument16 pagesIa 2 Compilation of Quiz and ExercisesclairedennprztananNo ratings yet
- A Kinsha 2013Document698 pagesA Kinsha 2013alexander2beshkovNo ratings yet
- T-Systems CPNI Policy Statement - Final 022717 PDFDocument2 pagesT-Systems CPNI Policy Statement - Final 022717 PDFFederal Communications Commission (FCC)No ratings yet
- Clinical Emergency Management Program: Advanced WorkshopDocument4 pagesClinical Emergency Management Program: Advanced WorkshopNataraj ThambiNo ratings yet
- PGDRD Mail Assignment 26 Feb PalitDocument8 pagesPGDRD Mail Assignment 26 Feb PalitDeepak PandeyNo ratings yet
- Varahi Krama EnglishDocument20 pagesVarahi Krama Englishmahesh madhavan100% (2)
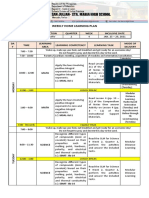
- Weekly Home Learning Plan: Grade Section Quarter Week Inclusive DateDocument3 pagesWeekly Home Learning Plan: Grade Section Quarter Week Inclusive DateMarvin Yebes ArceNo ratings yet
- Autocad Layout Tutorial - EhowDocument3 pagesAutocad Layout Tutorial - EhowdidlakiranNo ratings yet
- Minimal Stimulation IVF Vs Conventional IVFDocument8 pagesMinimal Stimulation IVF Vs Conventional IVFpolygoneNo ratings yet
- Referee Report TemplateDocument2 pagesReferee Report TemplateAna Jufriani100% (1)
- Enya Ukuleles - Enya Music UsaDocument1 pageEnya Ukuleles - Enya Music Usav9zmmt9g7hNo ratings yet
- For Updates Visit orDocument6 pagesFor Updates Visit orJFJannahNo ratings yet
- OSPE DU MedicineDocument101 pagesOSPE DU MedicinesaifNo ratings yet
- OutDocument318 pagesOutBet HalNo ratings yet