
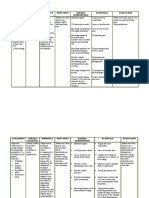
3eassessment Diagnosis Planning Nursing Intervention Rationale Evaluation
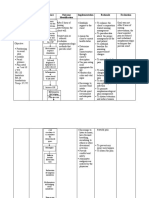
3eassessment Diagnosis Planning Nursing Intervention Rationale Evaluation
You might also like
- The Basics: A Comprehensive Outline of Nursing School ContentFrom EverandThe Basics: A Comprehensive Outline of Nursing School ContentRating: 5 out of 5 stars5/5 (3)
- Labor Pain NCPDocument4 pagesLabor Pain NCPBea Dela Cena60% (5)
- Nursing Care Plan of Breech PresentationDocument14 pagesNursing Care Plan of Breech PresentationDr-Sanjay Singhania100% (3)
- Nursing Care Plan - Acute Pain Related To Surgical IncisionDocument2 pagesNursing Care Plan - Acute Pain Related To Surgical IncisionCamilogs69% (13)
- ICU Orientation ManualDocument107 pagesICU Orientation Manualhery100% (2)
- List of Hormones Hypersecretion and Hyposecretion PDFDocument11 pagesList of Hormones Hypersecretion and Hyposecretion PDFAnil Kumar100% (1)
- ISA Brown Management GuideDocument18 pagesISA Brown Management Guidexman17us100% (3)
- NCP 1Document1 pageNCP 1Khrisha DavilloNo ratings yet
- Nursing Care Plan (Acute Cholecystitis) - NAVARRADocument6 pagesNursing Care Plan (Acute Cholecystitis) - NAVARRAami forevsNo ratings yet
- NCP Gouty ArthritisDocument21 pagesNCP Gouty ArthritisSeanmarie CabralesNo ratings yet
- Nursing Care PlansDocument4 pagesNursing Care Plansapi-19762967No ratings yet
- Assessment Nursing Diagnosis Planning Nursing Interventions Rationale Evaluation Subjective Cues: Short-Term Goal: Goal Met Short-Term GoalDocument3 pagesAssessment Nursing Diagnosis Planning Nursing Interventions Rationale Evaluation Subjective Cues: Short-Term Goal: Goal Met Short-Term GoalJan Lianne BernalesNo ratings yet
- Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument3 pagesAssessment Diagnosis Inference Planning Intervention Rationale EvaluationLaurel Joshua Reyes DauzNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationBUNDA, GLYZE A.No ratings yet
- IndependentDocument2 pagesIndependentQuinonez Anna MarieNo ratings yet
- NCP During LaborDocument6 pagesNCP During LaborJamielyn BassigNo ratings yet
- Nursing Care Plan - Labor PainDocument1 pageNursing Care Plan - Labor PainMarceline Vueen100% (1)
- 11 Nursing Care PlansDocument4 pages11 Nursing Care Planseknok03No ratings yet
- Acute Pain SCMCDocument2 pagesAcute Pain SCMCWik Wik PantuaNo ratings yet
- NCP UploadDocument1 pageNCP UploadAnonymous opu4ls27No ratings yet
- NCP NewDocument16 pagesNCP Newmsfts.No ratings yet
- NCP 3 in ER Module (Bernales, JLE)Document3 pagesNCP 3 in ER Module (Bernales, JLE)Jan Lianne BernalesNo ratings yet
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationDocument4 pagesAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationJobelle Acena100% (1)
- Acute Pain NCP Ob CaDocument5 pagesAcute Pain NCP Ob Caz.balista.537606No ratings yet
- Nursing Care Plan Assessment Nursing Diagnosis Rationale Planning Intervention Rationale EvaluationDocument3 pagesNursing Care Plan Assessment Nursing Diagnosis Rationale Planning Intervention Rationale EvaluationMary SutingcoNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument4 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationRenea Joy ArruejoNo ratings yet
- Assessment Diagnosis Scientific Basis Planning Nursing Interventions Rationale EvaluationDocument3 pagesAssessment Diagnosis Scientific Basis Planning Nursing Interventions Rationale EvaluationGj PaguidianNo ratings yet
- Nursing Care Plan: Assessment Nursing Diagnosis Planning Nursing Interventi ON Rationale EvaluationDocument2 pagesNursing Care Plan: Assessment Nursing Diagnosis Planning Nursing Interventi ON Rationale EvaluationRaidis PangilinanNo ratings yet
- IndependentDocument2 pagesIndependentQuinonez Anna MarieNo ratings yet
- NCP (Geria)Document4 pagesNCP (Geria)florenzoNo ratings yet
- Potts Disease NCP .. JustificationDocument8 pagesPotts Disease NCP .. JustificationMicah SalesNo ratings yet
- Subjective: Sto: Diagnostic:: Assessme NT Explanatio Nofthe Problem Planning Interven Tion Rationale Evaluati ONDocument3 pagesSubjective: Sto: Diagnostic:: Assessme NT Explanatio Nofthe Problem Planning Interven Tion Rationale Evaluati ONRona PieNo ratings yet
- NCP Increased ICPDocument3 pagesNCP Increased ICPMa. Kaile Shyla LlacarNo ratings yet
- NCP ReviseDocument7 pagesNCP ReviseRhobic ManansalaNo ratings yet
- Rafin NCP and Drug StudyDocument7 pagesRafin NCP and Drug StudyCezanne CruzNo ratings yet
- Assessment Nursing Diagnosis Planning/Objectives Nursing Intervention Rationale Evaluation Subjective Cues: IndependentDocument4 pagesAssessment Nursing Diagnosis Planning/Objectives Nursing Intervention Rationale Evaluation Subjective Cues: IndependentLezil Arapoc DeconNo ratings yet
- Corrected NCP Case 3 Intrapartum NCPDocument2 pagesCorrected NCP Case 3 Intrapartum NCPReyzel PahunaoNo ratings yet
- St. Paul University PhilippinesDocument3 pagesSt. Paul University PhilippinesMia Grace GarciaNo ratings yet
- AssessmentDocument4 pagesAssessmentWei CoNo ratings yet
- Module #8 NCP (Bernales, JLE)Document4 pagesModule #8 NCP (Bernales, JLE)Jan Lianne BernalesNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term Goals: Independent: Short Term GoalsDocument1 pageAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term Goals: Independent: Short Term GoalskyawNo ratings yet
- Short Term: Independent:: 7 CM, Stage IV Pressure Ulcer in The SacrumDocument2 pagesShort Term: Independent:: 7 CM, Stage IV Pressure Ulcer in The Sacrumaaron tabernaNo ratings yet
- Pleural EffusionDocument5 pagesPleural EffusionTerizla MobileNo ratings yet
- Case Study: Problems in Reproduction and Sexuality: A Client With GonorrheaDocument8 pagesCase Study: Problems in Reproduction and Sexuality: A Client With GonorrheaShiena Mae PelagioNo ratings yet
- NCP PainDocument2 pagesNCP PainKimNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Planning Implementation Rationale EvaluationDocument6 pagesNursing Care Plan: Assessment Diagnosis Planning Implementation Rationale EvaluationJohn Patrick LegaspinaNo ratings yet
- NCP - Baby Final PDFDocument11 pagesNCP - Baby Final PDFCindy MariscotesNo ratings yet
- NCP Acute PainDocument2 pagesNCP Acute PainNecheal BaayNo ratings yet
- Data Nursing Diagnosis Planning Interventions Rationale EvaluationDocument3 pagesData Nursing Diagnosis Planning Interventions Rationale Evaluationbea pegadNo ratings yet
- Nursing Care Plan Assessment Diagnosis Scientific Basis Planning Interventions Rationale EvaluationDocument2 pagesNursing Care Plan Assessment Diagnosis Scientific Basis Planning Interventions Rationale EvaluationAgnes GeolinaNo ratings yet
- NCP 69-70Document2 pagesNCP 69-70kateleneNo ratings yet
- Nursing Care Plan Mrs. Patao Ob Ward, GSGH Assessment SubjectiveDocument3 pagesNursing Care Plan Mrs. Patao Ob Ward, GSGH Assessment Subjectiveraizelc100% (2)
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument1 pageAssessment Diagnosis Planning Intervention Rationale EvaluationAira AlaroNo ratings yet
- Case Scenario 5 NCPDocument10 pagesCase Scenario 5 NCPkdfhjfhfNo ratings yet
- Page 17 ACUTE PAIN Related To Joint Stiffness Secondary To Aging.Document3 pagesPage 17 ACUTE PAIN Related To Joint Stiffness Secondary To Aging.Senyorita KHayeNo ratings yet
- Otitis Media NCPDocument3 pagesOtitis Media NCPJames AbendanNo ratings yet
- Nursing Diagnosis # 1 Acute Pain Related To Abdominal Incision.Document10 pagesNursing Diagnosis # 1 Acute Pain Related To Abdominal Incision.jhunanax100% (3)
- Assessment Cues Nursing Outcome Planning Nursing Interventions Evaluation Diagnosis Identification Interventions RationaleDocument6 pagesAssessment Cues Nursing Outcome Planning Nursing Interventions Evaluation Diagnosis Identification Interventions RationaleAna LuisaNo ratings yet
- Acutepain RevisedDocument3 pagesAcutepain RevisedAndrea AutorNo ratings yet
- Subjective Cues Long Term Objective Independent: Independent: Long Term: Goal MetDocument3 pagesSubjective Cues Long Term Objective Independent: Independent: Long Term: Goal MetYVETTE CLAIRE BORRESNo ratings yet
- Demonstrate: Pain Coping TechniquesDocument4 pagesDemonstrate: Pain Coping TechniquesMae Therese B. MAGNO100% (1)
- Norbe COMFORT MEASURESDocument10 pagesNorbe COMFORT MEASURESMarlo Dañez NorbeNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: Short Term Goal: Independent: Short Term Goal OutcomeDocument9 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: Short Term Goal: Independent: Short Term Goal OutcomeCindy MariscotesNo ratings yet
- Surgery State Exam Question ListDocument18 pagesSurgery State Exam Question ListJonathanGrahamNo ratings yet
- The Pioneering Work of William J. McCormick, M.D.Document4 pagesThe Pioneering Work of William J. McCormick, M.D.Βόρειο ΣέλαςNo ratings yet
- Medical ManagementDocument6 pagesMedical ManagementSittie Nashieva A. UsmanNo ratings yet
- Kanika Album CasesDocument55 pagesKanika Album Casesmahima guptaNo ratings yet
- Treatment of Malar Mounds With Hyaluronic Acid Fillers - An Anatomical ApproachDocument5 pagesTreatment of Malar Mounds With Hyaluronic Acid Fillers - An Anatomical ApproachArcelino FariasNo ratings yet
- Dara Mola 2016Document5 pagesDara Mola 2016andiniNo ratings yet
- Pandas and StutteringDocument2 pagesPandas and Stutteringdhruvakathuria100% (1)
- Post Marketing SurveillanceDocument19 pagesPost Marketing SurveillanceRamanjeet SinghNo ratings yet
- Preparing InjectionDocument24 pagesPreparing InjectionKumala Mega AselaNo ratings yet
- SentinaDocument10 pagesSentinaakayaNo ratings yet
- WJR 8 656Document13 pagesWJR 8 656aldosaputraNo ratings yet
- Activity 2: "YOU CAN DO IT!"Document4 pagesActivity 2: "YOU CAN DO IT!"Christian VillaNo ratings yet
- Safer - Partying - Pocket - Guide - 2016 PDFDocument16 pagesSafer - Partying - Pocket - Guide - 2016 PDFwebmaster@drugpolicy.orgNo ratings yet
- Invest and Medication 1Document9 pagesInvest and Medication 1RajaNo ratings yet
- Otpf 3RD Edition Work Book PDFDocument4 pagesOtpf 3RD Edition Work Book PDFvielorna fionna fongNo ratings yet
- Anesthesiology Clinics Volume 32 Issue 2 2014 (Doi 10.1016/j.anclin.2014.02.022) Anderson, Jennifer Klock, P. Allan PDFDocument17 pagesAnesthesiology Clinics Volume 32 Issue 2 2014 (Doi 10.1016/j.anclin.2014.02.022) Anderson, Jennifer Klock, P. Allan PDFaprinaNo ratings yet
- Hermetic Reiki: A Complete Practitioner's ManualDocument126 pagesHermetic Reiki: A Complete Practitioner's ManualJames Bulls97% (35)
- API Accu ClearDocument8 pagesAPI Accu ClearPeter HartonoNo ratings yet
- DextroseDocument1 pageDextroseamaliea234No ratings yet
- Gynaecological Diseases in PregnancyDocument76 pagesGynaecological Diseases in PregnancyKarishma Shroff70% (10)
- MMS HCV ProtocolDocument2 pagesMMS HCV Protocolxpat16391100% (1)
- 0.9% Sodium Chloride Injection, USP: Prescribing InformationDocument8 pages0.9% Sodium Chloride Injection, USP: Prescribing InformationarinNo ratings yet
- NIH Aids Info HIV Treatment Guidelines AdultandadolescentglDocument267 pagesNIH Aids Info HIV Treatment Guidelines Adultandadolescentglbmartindoyle6396No ratings yet
- Presented By: Docia Baah Tutor, NMTC - TeshieDocument20 pagesPresented By: Docia Baah Tutor, NMTC - TeshieDociaNo ratings yet
- Characteristics of Waste Water in Sewage Treatment Plant of Bhopal IndiaDocument6 pagesCharacteristics of Waste Water in Sewage Treatment Plant of Bhopal Indiasunaina agarwalNo ratings yet
- Thought Diary 3 PDFDocument2 pagesThought Diary 3 PDFsolNo ratings yet
- Family Therapy Balloon ActivitiesDocument5 pagesFamily Therapy Balloon ActivitiesSocial Services Section100% (1)
























































































Download as docx, pdf, or txt
You might also like
- The Basics: A Comprehensive Outline of Nursing School ContentFrom EverandThe Basics: A Comprehensive Outline of Nursing School ContentRating: 5 out of 5 stars5/5 (3)
- Labor Pain NCPDocument4 pagesLabor Pain NCPBea Dela Cena60% (5)
- Nursing Care Plan of Breech PresentationDocument14 pagesNursing Care Plan of Breech PresentationDr-Sanjay Singhania100% (3)
- Nursing Care Plan - Acute Pain Related To Surgical IncisionDocument2 pagesNursing Care Plan - Acute Pain Related To Surgical IncisionCamilogs69% (13)
- ICU Orientation ManualDocument107 pagesICU Orientation Manualhery100% (2)
- List of Hormones Hypersecretion and Hyposecretion PDFDocument11 pagesList of Hormones Hypersecretion and Hyposecretion PDFAnil Kumar100% (1)
- ISA Brown Management GuideDocument18 pagesISA Brown Management Guidexman17us100% (3)
- NCP 1Document1 pageNCP 1Khrisha DavilloNo ratings yet
- Nursing Care Plan (Acute Cholecystitis) - NAVARRADocument6 pagesNursing Care Plan (Acute Cholecystitis) - NAVARRAami forevsNo ratings yet
- NCP Gouty ArthritisDocument21 pagesNCP Gouty ArthritisSeanmarie CabralesNo ratings yet
- Nursing Care PlansDocument4 pagesNursing Care Plansapi-19762967No ratings yet
- Assessment Nursing Diagnosis Planning Nursing Interventions Rationale Evaluation Subjective Cues: Short-Term Goal: Goal Met Short-Term GoalDocument3 pagesAssessment Nursing Diagnosis Planning Nursing Interventions Rationale Evaluation Subjective Cues: Short-Term Goal: Goal Met Short-Term GoalJan Lianne BernalesNo ratings yet
- Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument3 pagesAssessment Diagnosis Inference Planning Intervention Rationale EvaluationLaurel Joshua Reyes DauzNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationBUNDA, GLYZE A.No ratings yet
- IndependentDocument2 pagesIndependentQuinonez Anna MarieNo ratings yet
- NCP During LaborDocument6 pagesNCP During LaborJamielyn BassigNo ratings yet
- Nursing Care Plan - Labor PainDocument1 pageNursing Care Plan - Labor PainMarceline Vueen100% (1)
- 11 Nursing Care PlansDocument4 pages11 Nursing Care Planseknok03No ratings yet
- Acute Pain SCMCDocument2 pagesAcute Pain SCMCWik Wik PantuaNo ratings yet
- NCP UploadDocument1 pageNCP UploadAnonymous opu4ls27No ratings yet
- NCP NewDocument16 pagesNCP Newmsfts.No ratings yet
- NCP 3 in ER Module (Bernales, JLE)Document3 pagesNCP 3 in ER Module (Bernales, JLE)Jan Lianne BernalesNo ratings yet
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationDocument4 pagesAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationJobelle Acena100% (1)
- Acute Pain NCP Ob CaDocument5 pagesAcute Pain NCP Ob Caz.balista.537606No ratings yet
- Nursing Care Plan Assessment Nursing Diagnosis Rationale Planning Intervention Rationale EvaluationDocument3 pagesNursing Care Plan Assessment Nursing Diagnosis Rationale Planning Intervention Rationale EvaluationMary SutingcoNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument4 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationRenea Joy ArruejoNo ratings yet
- Assessment Diagnosis Scientific Basis Planning Nursing Interventions Rationale EvaluationDocument3 pagesAssessment Diagnosis Scientific Basis Planning Nursing Interventions Rationale EvaluationGj PaguidianNo ratings yet
- Nursing Care Plan: Assessment Nursing Diagnosis Planning Nursing Interventi ON Rationale EvaluationDocument2 pagesNursing Care Plan: Assessment Nursing Diagnosis Planning Nursing Interventi ON Rationale EvaluationRaidis PangilinanNo ratings yet
- IndependentDocument2 pagesIndependentQuinonez Anna MarieNo ratings yet
- NCP (Geria)Document4 pagesNCP (Geria)florenzoNo ratings yet
- Potts Disease NCP .. JustificationDocument8 pagesPotts Disease NCP .. JustificationMicah SalesNo ratings yet
- Subjective: Sto: Diagnostic:: Assessme NT Explanatio Nofthe Problem Planning Interven Tion Rationale Evaluati ONDocument3 pagesSubjective: Sto: Diagnostic:: Assessme NT Explanatio Nofthe Problem Planning Interven Tion Rationale Evaluati ONRona PieNo ratings yet
- NCP Increased ICPDocument3 pagesNCP Increased ICPMa. Kaile Shyla LlacarNo ratings yet
- NCP ReviseDocument7 pagesNCP ReviseRhobic ManansalaNo ratings yet
- Rafin NCP and Drug StudyDocument7 pagesRafin NCP and Drug StudyCezanne CruzNo ratings yet
- Assessment Nursing Diagnosis Planning/Objectives Nursing Intervention Rationale Evaluation Subjective Cues: IndependentDocument4 pagesAssessment Nursing Diagnosis Planning/Objectives Nursing Intervention Rationale Evaluation Subjective Cues: IndependentLezil Arapoc DeconNo ratings yet
- Corrected NCP Case 3 Intrapartum NCPDocument2 pagesCorrected NCP Case 3 Intrapartum NCPReyzel PahunaoNo ratings yet
- St. Paul University PhilippinesDocument3 pagesSt. Paul University PhilippinesMia Grace GarciaNo ratings yet
- AssessmentDocument4 pagesAssessmentWei CoNo ratings yet
- Module #8 NCP (Bernales, JLE)Document4 pagesModule #8 NCP (Bernales, JLE)Jan Lianne BernalesNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term Goals: Independent: Short Term GoalsDocument1 pageAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term Goals: Independent: Short Term GoalskyawNo ratings yet
- Short Term: Independent:: 7 CM, Stage IV Pressure Ulcer in The SacrumDocument2 pagesShort Term: Independent:: 7 CM, Stage IV Pressure Ulcer in The Sacrumaaron tabernaNo ratings yet
- Pleural EffusionDocument5 pagesPleural EffusionTerizla MobileNo ratings yet
- Case Study: Problems in Reproduction and Sexuality: A Client With GonorrheaDocument8 pagesCase Study: Problems in Reproduction and Sexuality: A Client With GonorrheaShiena Mae PelagioNo ratings yet
- NCP PainDocument2 pagesNCP PainKimNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Planning Implementation Rationale EvaluationDocument6 pagesNursing Care Plan: Assessment Diagnosis Planning Implementation Rationale EvaluationJohn Patrick LegaspinaNo ratings yet
- NCP - Baby Final PDFDocument11 pagesNCP - Baby Final PDFCindy MariscotesNo ratings yet
- NCP Acute PainDocument2 pagesNCP Acute PainNecheal BaayNo ratings yet
- Data Nursing Diagnosis Planning Interventions Rationale EvaluationDocument3 pagesData Nursing Diagnosis Planning Interventions Rationale Evaluationbea pegadNo ratings yet
- Nursing Care Plan Assessment Diagnosis Scientific Basis Planning Interventions Rationale EvaluationDocument2 pagesNursing Care Plan Assessment Diagnosis Scientific Basis Planning Interventions Rationale EvaluationAgnes GeolinaNo ratings yet
- NCP 69-70Document2 pagesNCP 69-70kateleneNo ratings yet
- Nursing Care Plan Mrs. Patao Ob Ward, GSGH Assessment SubjectiveDocument3 pagesNursing Care Plan Mrs. Patao Ob Ward, GSGH Assessment Subjectiveraizelc100% (2)
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument1 pageAssessment Diagnosis Planning Intervention Rationale EvaluationAira AlaroNo ratings yet
- Case Scenario 5 NCPDocument10 pagesCase Scenario 5 NCPkdfhjfhfNo ratings yet
- Page 17 ACUTE PAIN Related To Joint Stiffness Secondary To Aging.Document3 pagesPage 17 ACUTE PAIN Related To Joint Stiffness Secondary To Aging.Senyorita KHayeNo ratings yet
- Otitis Media NCPDocument3 pagesOtitis Media NCPJames AbendanNo ratings yet
- Nursing Diagnosis # 1 Acute Pain Related To Abdominal Incision.Document10 pagesNursing Diagnosis # 1 Acute Pain Related To Abdominal Incision.jhunanax100% (3)
- Assessment Cues Nursing Outcome Planning Nursing Interventions Evaluation Diagnosis Identification Interventions RationaleDocument6 pagesAssessment Cues Nursing Outcome Planning Nursing Interventions Evaluation Diagnosis Identification Interventions RationaleAna LuisaNo ratings yet
- Acutepain RevisedDocument3 pagesAcutepain RevisedAndrea AutorNo ratings yet
- Subjective Cues Long Term Objective Independent: Independent: Long Term: Goal MetDocument3 pagesSubjective Cues Long Term Objective Independent: Independent: Long Term: Goal MetYVETTE CLAIRE BORRESNo ratings yet
- Demonstrate: Pain Coping TechniquesDocument4 pagesDemonstrate: Pain Coping TechniquesMae Therese B. MAGNO100% (1)
- Norbe COMFORT MEASURESDocument10 pagesNorbe COMFORT MEASURESMarlo Dañez NorbeNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: Short Term Goal: Independent: Short Term Goal OutcomeDocument9 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: Short Term Goal: Independent: Short Term Goal OutcomeCindy MariscotesNo ratings yet
- Surgery State Exam Question ListDocument18 pagesSurgery State Exam Question ListJonathanGrahamNo ratings yet
- The Pioneering Work of William J. McCormick, M.D.Document4 pagesThe Pioneering Work of William J. McCormick, M.D.Βόρειο ΣέλαςNo ratings yet
- Medical ManagementDocument6 pagesMedical ManagementSittie Nashieva A. UsmanNo ratings yet
- Kanika Album CasesDocument55 pagesKanika Album Casesmahima guptaNo ratings yet
- Treatment of Malar Mounds With Hyaluronic Acid Fillers - An Anatomical ApproachDocument5 pagesTreatment of Malar Mounds With Hyaluronic Acid Fillers - An Anatomical ApproachArcelino FariasNo ratings yet
- Dara Mola 2016Document5 pagesDara Mola 2016andiniNo ratings yet
- Pandas and StutteringDocument2 pagesPandas and Stutteringdhruvakathuria100% (1)
- Post Marketing SurveillanceDocument19 pagesPost Marketing SurveillanceRamanjeet SinghNo ratings yet
- Preparing InjectionDocument24 pagesPreparing InjectionKumala Mega AselaNo ratings yet
- SentinaDocument10 pagesSentinaakayaNo ratings yet
- WJR 8 656Document13 pagesWJR 8 656aldosaputraNo ratings yet
- Activity 2: "YOU CAN DO IT!"Document4 pagesActivity 2: "YOU CAN DO IT!"Christian VillaNo ratings yet
- Safer - Partying - Pocket - Guide - 2016 PDFDocument16 pagesSafer - Partying - Pocket - Guide - 2016 PDFwebmaster@drugpolicy.orgNo ratings yet
- Invest and Medication 1Document9 pagesInvest and Medication 1RajaNo ratings yet
- Otpf 3RD Edition Work Book PDFDocument4 pagesOtpf 3RD Edition Work Book PDFvielorna fionna fongNo ratings yet
- Anesthesiology Clinics Volume 32 Issue 2 2014 (Doi 10.1016/j.anclin.2014.02.022) Anderson, Jennifer Klock, P. Allan PDFDocument17 pagesAnesthesiology Clinics Volume 32 Issue 2 2014 (Doi 10.1016/j.anclin.2014.02.022) Anderson, Jennifer Klock, P. Allan PDFaprinaNo ratings yet
- Hermetic Reiki: A Complete Practitioner's ManualDocument126 pagesHermetic Reiki: A Complete Practitioner's ManualJames Bulls97% (35)
- API Accu ClearDocument8 pagesAPI Accu ClearPeter HartonoNo ratings yet
- DextroseDocument1 pageDextroseamaliea234No ratings yet
- Gynaecological Diseases in PregnancyDocument76 pagesGynaecological Diseases in PregnancyKarishma Shroff70% (10)
- MMS HCV ProtocolDocument2 pagesMMS HCV Protocolxpat16391100% (1)
- 0.9% Sodium Chloride Injection, USP: Prescribing InformationDocument8 pages0.9% Sodium Chloride Injection, USP: Prescribing InformationarinNo ratings yet
- NIH Aids Info HIV Treatment Guidelines AdultandadolescentglDocument267 pagesNIH Aids Info HIV Treatment Guidelines Adultandadolescentglbmartindoyle6396No ratings yet
- Presented By: Docia Baah Tutor, NMTC - TeshieDocument20 pagesPresented By: Docia Baah Tutor, NMTC - TeshieDociaNo ratings yet
- Characteristics of Waste Water in Sewage Treatment Plant of Bhopal IndiaDocument6 pagesCharacteristics of Waste Water in Sewage Treatment Plant of Bhopal Indiasunaina agarwalNo ratings yet
- Thought Diary 3 PDFDocument2 pagesThought Diary 3 PDFsolNo ratings yet
- Family Therapy Balloon ActivitiesDocument5 pagesFamily Therapy Balloon ActivitiesSocial Services Section100% (1)