
1 Attending Physician Form
1 Attending Physician Form
You might also like
- Pre Employment Medical Declaration Form PDFDocument2 pagesPre Employment Medical Declaration Form PDFAshwini Tyagi75% (4)
- MD Imran Welder 2200Document1 pageMD Imran Welder 2200Jeevan RaoNo ratings yet
- Case Investigation Forms - Pidsrmop3ed 1Document16 pagesCase Investigation Forms - Pidsrmop3ed 1RHU Dupax del Sur100% (3)
- Group Death - Attending Physician's StatementDocument2 pagesGroup Death - Attending Physician's StatementJohn Victor Perez OretoNo ratings yet
- 2 Death Abroad FormDocument2 pages2 Death Abroad Formbtwerror478No ratings yet
- Hypertension Questionnaire For Proposed Insured/OwnerDocument1 pageHypertension Questionnaire For Proposed Insured/OwnerSincerely ReynNo ratings yet
- D ReportDocument2 pagesD ReportHihiNo ratings yet
- Hospital StandardQC FormsDocument22 pagesHospital StandardQC FormstotqmNo ratings yet
- Medical Attendants Certificate17062019Document2 pagesMedical Attendants Certificate17062019PrathameshNo ratings yet
- Epilepsy Questionnaire For Proposed Insured/OwnerDocument1 pageEpilepsy Questionnaire For Proposed Insured/OwnerSincerely ReynNo ratings yet
- Non-Neonatal Tetanus: (ICD 10 Code: A35)Document2 pagesNon-Neonatal Tetanus: (ICD 10 Code: A35)CHICKY100% (1)
- Disposition of RemainsDocument1 pageDisposition of Remainsmj digitalNo ratings yet
- Medical Certificate of Fitness: To Be Filled by CandidateDocument2 pagesMedical Certificate of Fitness: To Be Filled by CandidatevenkatNo ratings yet
- DR Langford1Document8 pagesDR Langford1Spencer JacksonNo ratings yet
- Student Health Form - FinalDocument3 pagesStudent Health Form - Finalbrown_chocolate87643No ratings yet
- Medical FormDocument2 pagesMedical FormPritam685No ratings yet
- PT Intake FormDocument4 pagesPT Intake FormChifor FlorinNo ratings yet
- 6446 PDFDocument15 pages6446 PDFGanesh DasaraNo ratings yet
- Acute Flaccid Paralysis: Case Investigation FormDocument2 pagesAcute Flaccid Paralysis: Case Investigation FormPaul Angelo E. Caliva0% (1)
- Claimant Statement Form Death 2016-7-7 10-16-21 498Document5 pagesClaimant Statement Form Death 2016-7-7 10-16-21 498Priya ThakurNo ratings yet
- Attending Physicians Statement-Death ClaimDocument2 pagesAttending Physicians Statement-Death ClaimKen CelesteNo ratings yet
- New Axa FormDocument2 pagesNew Axa FormAzrul Azuar Azrul Azuar100% (1)
- THQ Hospital Naushera District KhushabDocument2 pagesTHQ Hospital Naushera District KhushabSaif Ur RehmanNo ratings yet
- AMAM ApplicationDocument3 pagesAMAM ApplicationSharyar MalikNo ratings yet
- Cif NTDocument2 pagesCif NTIvy marie BonNo ratings yet
- Dr. Eutiquio Ll. Atanacio Jr. Memorial Hospital, Inc: DOH-EB-AEHMD-FWRIPIS-2021-0Document3 pagesDr. Eutiquio Ll. Atanacio Jr. Memorial Hospital, Inc: DOH-EB-AEHMD-FWRIPIS-2021-0deamhi nursing serviceNo ratings yet
- Dental WaiverDocument1 pageDental WaiverMary Grace LemonNo ratings yet
- Arthritis Disorder Questionnaire For Proposed Insured/OwnerDocument1 pageArthritis Disorder Questionnaire For Proposed Insured/OwnerSincerely ReynNo ratings yet
- Medical Cer Ficate of Fitness: To Be Filled by CandidateDocument2 pagesMedical Cer Ficate of Fitness: To Be Filled by CandidateDINESH CHANDRA GANNAVARAPUNo ratings yet
- Case Report Form For HFMDDocument2 pagesCase Report Form For HFMDMendez RhuNo ratings yet
- CRF HFMD AsmghDocument2 pagesCRF HFMD AsmghRyeowook RyeNo ratings yet
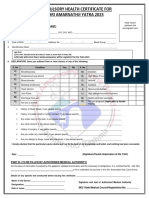
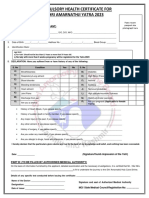
- Compulsory Health Certificate For Shri Amarnathji Yatra 2023Document1 pageCompulsory Health Certificate For Shri Amarnathji Yatra 2023Eknath KoliNo ratings yet
- Kardex: Date Ordere D Additional Orders Date Ordered Additional OrdersDocument14 pagesKardex: Date Ordere D Additional Orders Date Ordered Additional OrdersLRBNo ratings yet
- FWRI Form ReviseDocument3 pagesFWRI Form ReviseJm uniteNo ratings yet
- Form G Health Examination Report International StudentDocument6 pagesForm G Health Examination Report International StudentVictor OjukwuNo ratings yet
- General History and Physical Examination FormDocument2 pagesGeneral History and Physical Examination FormQueen Hera100% (1)
- St. Michael's Preparatory School: Health History FormDocument1 pageSt. Michael's Preparatory School: Health History FormJay309No ratings yet
- Acute Bloody Diarrhea - Ver Oct 12 2012Document2 pagesAcute Bloody Diarrhea - Ver Oct 12 2012rhu silagoNo ratings yet
- 11 Trauma Emergency Form 19102023Document2 pages11 Trauma Emergency Form 19102023Marjorie BricenioNo ratings yet
- Gym Member Registration FormDocument2 pagesGym Member Registration FormChethan Sharma RNo ratings yet
- Aefi CifDocument6 pagesAefi CifVic KwanNo ratings yet
- Pre Employment Medical Declaration Form - 2022Document2 pagesPre Employment Medical Declaration Form - 2022Neel GhoshNo ratings yet
- Physical Restraint Monitoring FormDocument1 pagePhysical Restraint Monitoring FormChandu Pandit100% (4)
- CHC Updated 2023Document1 pageCHC Updated 2023maheshmonu9449No ratings yet
- CHC Updated 2023Document1 pageCHC Updated 2023Vishal Singh ShekhawatNo ratings yet
- Natoza Medical Form For Grade 7 12Document3 pagesNatoza Medical Form For Grade 7 12Deonna AngelineNo ratings yet
- Referral Form Jessa 2021Document1 pageReferral Form Jessa 2021Jessa MaeNo ratings yet
- Lonpac Maid Medical ClaimDocument3 pagesLonpac Maid Medical ClaimYl EdianonNo ratings yet
- Medical CertificateDocument2 pagesMedical CertificatelekacaNo ratings yet
- Kolej Teknologi Darulnaim: Darulnaim College of TechnologyDocument5 pagesKolej Teknologi Darulnaim: Darulnaim College of TechnologyDaryanto SutejiNo ratings yet
- Medical CertificateDocument2 pagesMedical CertificateBalaziEswarNo ratings yet
- Medical Certificate 2Document2 pagesMedical Certificate 2Aditeya Shukla100% (1)
- FWRI 2023 CIF v2Document3 pagesFWRI 2023 CIF v2Terence John ChebatNo ratings yet
- Fwri Cif FormDocument3 pagesFwri Cif FormMHO GloriaNo ratings yet
- HMRM RECORD DoccDocument13 pagesHMRM RECORD DoccBharath BeeNo ratings yet
- One Step Med: General Medical Information Record Keeping ManualFrom EverandOne Step Med: General Medical Information Record Keeping ManualNo ratings yet
- I-C-E in Case of Emergency: Your Essential Medical JournalFrom EverandI-C-E in Case of Emergency: Your Essential Medical JournalNo ratings yet
- No Person Can Dispence Medicnine Other Then Reg PharmacistDocument22 pagesNo Person Can Dispence Medicnine Other Then Reg PharmacistSandeep PandeyNo ratings yet
- Ob Nursing Evaluation ToolDocument4 pagesOb Nursing Evaluation ToolLyra Mae E. MendozaNo ratings yet
- CBT - Nursing Care and Responsibility EditedDocument53 pagesCBT - Nursing Care and Responsibility Editedhimali ranasingheNo ratings yet
- Nothile XhakazaDocument3 pagesNothile XhakazaxhakazanondumisoNo ratings yet
- Master Rotation Plan For GNMDocument9 pagesMaster Rotation Plan For GNMAnanya HatiNo ratings yet
- Independent Medical Education - PfizerDocument6 pagesIndependent Medical Education - PfizerkelvinkinergyNo ratings yet
- Geriatrics 23 BrochureDocument5 pagesGeriatrics 23 BrochureMUHAMMAD09No ratings yet
- Resume & Portofolio Stefanus Nofa 2021Document4 pagesResume & Portofolio Stefanus Nofa 2021khrisnagungNo ratings yet
- Week 7 Primary Care Lecture To StudentsDocument63 pagesWeek 7 Primary Care Lecture To StudentsBoltNo ratings yet
- Lamaran - Produksi (Yusuf)Document3 pagesLamaran - Produksi (Yusuf)Salatiga ParamedicNo ratings yet
- Curriculum VitaeDocument3 pagesCurriculum VitaeOliver OsiroNo ratings yet
- DME Billing Services OverviewDocument6 pagesDME Billing Services OverviewINF HealthcareNo ratings yet
- Airline EssayDocument1 pageAirline EssayJhariel PeregrinaNo ratings yet
- IRDA - Claim Form-2Document1 pageIRDA - Claim Form-2Sunny bNo ratings yet
- Prince PDFDocument9 pagesPrince PDFNK NikhilNo ratings yet
- JacksonDocument2 pagesJacksonapi-641837495No ratings yet
- The United States Health Care System Combining Business Health and Delivery 2nd Edition Austin Test BankDocument11 pagesThe United States Health Care System Combining Business Health and Delivery 2nd Edition Austin Test Banklaylafarleyh3i8j9100% (26)
- 122-Article Text-453-1-10-20200622Document12 pages122-Article Text-453-1-10-20200622Real TetisoraNo ratings yet
- Log Book: Clinical Clerkship ProgramDocument16 pagesLog Book: Clinical Clerkship Programjayen_98No ratings yet
- HospitalDocument7 pagesHospitalJaikapil KachhawaNo ratings yet
- Weaving Traditional and Professional Midwifery - EditedDocument5 pagesWeaving Traditional and Professional Midwifery - EditedMAKOKHA BONFACENo ratings yet
- De-Empanelment 05.01.2023Document1 pageDe-Empanelment 05.01.2023Bhavani RentalaNo ratings yet
- NBHS2513 Professional Issues in HealthcareDocument13 pagesNBHS2513 Professional Issues in HealthcareSimon RajNo ratings yet
- AnnexC PC-HFDocument5 pagesAnnexC PC-HFJirhana Lindagan Karon-KampangNo ratings yet
- Ra-113838 Professional Teacher - Elementary Masbate 3-2023Document88 pagesRa-113838 Professional Teacher - Elementary Masbate 3-2023Jessa Marie JardinNo ratings yet
- Vaccination Sites Per Municipalities of South CotabatoDocument2 pagesVaccination Sites Per Municipalities of South CotabatoHEMS SOCOTNo ratings yet
- Sterling Roberts Resume DoneDocument2 pagesSterling Roberts Resume Doneapi-662884360No ratings yet
- CMS 1500 - 2012 - 0001Document4 pagesCMS 1500 - 2012 - 0001chamuditha dilshanNo ratings yet
- Trend Dan Isue Keperawatan KeluargaDocument15 pagesTrend Dan Isue Keperawatan KeluargaFebby WidiantoNo ratings yet






















































































Download as pdf or txt
You might also like
- Pre Employment Medical Declaration Form PDFDocument2 pagesPre Employment Medical Declaration Form PDFAshwini Tyagi75% (4)
- MD Imran Welder 2200Document1 pageMD Imran Welder 2200Jeevan RaoNo ratings yet
- Case Investigation Forms - Pidsrmop3ed 1Document16 pagesCase Investigation Forms - Pidsrmop3ed 1RHU Dupax del Sur100% (3)
- Group Death - Attending Physician's StatementDocument2 pagesGroup Death - Attending Physician's StatementJohn Victor Perez OretoNo ratings yet
- 2 Death Abroad FormDocument2 pages2 Death Abroad Formbtwerror478No ratings yet
- Hypertension Questionnaire For Proposed Insured/OwnerDocument1 pageHypertension Questionnaire For Proposed Insured/OwnerSincerely ReynNo ratings yet
- D ReportDocument2 pagesD ReportHihiNo ratings yet
- Hospital StandardQC FormsDocument22 pagesHospital StandardQC FormstotqmNo ratings yet
- Medical Attendants Certificate17062019Document2 pagesMedical Attendants Certificate17062019PrathameshNo ratings yet
- Epilepsy Questionnaire For Proposed Insured/OwnerDocument1 pageEpilepsy Questionnaire For Proposed Insured/OwnerSincerely ReynNo ratings yet
- Non-Neonatal Tetanus: (ICD 10 Code: A35)Document2 pagesNon-Neonatal Tetanus: (ICD 10 Code: A35)CHICKY100% (1)
- Disposition of RemainsDocument1 pageDisposition of Remainsmj digitalNo ratings yet
- Medical Certificate of Fitness: To Be Filled by CandidateDocument2 pagesMedical Certificate of Fitness: To Be Filled by CandidatevenkatNo ratings yet
- DR Langford1Document8 pagesDR Langford1Spencer JacksonNo ratings yet
- Student Health Form - FinalDocument3 pagesStudent Health Form - Finalbrown_chocolate87643No ratings yet
- Medical FormDocument2 pagesMedical FormPritam685No ratings yet
- PT Intake FormDocument4 pagesPT Intake FormChifor FlorinNo ratings yet
- 6446 PDFDocument15 pages6446 PDFGanesh DasaraNo ratings yet
- Acute Flaccid Paralysis: Case Investigation FormDocument2 pagesAcute Flaccid Paralysis: Case Investigation FormPaul Angelo E. Caliva0% (1)
- Claimant Statement Form Death 2016-7-7 10-16-21 498Document5 pagesClaimant Statement Form Death 2016-7-7 10-16-21 498Priya ThakurNo ratings yet
- Attending Physicians Statement-Death ClaimDocument2 pagesAttending Physicians Statement-Death ClaimKen CelesteNo ratings yet
- New Axa FormDocument2 pagesNew Axa FormAzrul Azuar Azrul Azuar100% (1)
- THQ Hospital Naushera District KhushabDocument2 pagesTHQ Hospital Naushera District KhushabSaif Ur RehmanNo ratings yet
- AMAM ApplicationDocument3 pagesAMAM ApplicationSharyar MalikNo ratings yet
- Cif NTDocument2 pagesCif NTIvy marie BonNo ratings yet
- Dr. Eutiquio Ll. Atanacio Jr. Memorial Hospital, Inc: DOH-EB-AEHMD-FWRIPIS-2021-0Document3 pagesDr. Eutiquio Ll. Atanacio Jr. Memorial Hospital, Inc: DOH-EB-AEHMD-FWRIPIS-2021-0deamhi nursing serviceNo ratings yet
- Dental WaiverDocument1 pageDental WaiverMary Grace LemonNo ratings yet
- Arthritis Disorder Questionnaire For Proposed Insured/OwnerDocument1 pageArthritis Disorder Questionnaire For Proposed Insured/OwnerSincerely ReynNo ratings yet
- Medical Cer Ficate of Fitness: To Be Filled by CandidateDocument2 pagesMedical Cer Ficate of Fitness: To Be Filled by CandidateDINESH CHANDRA GANNAVARAPUNo ratings yet
- Case Report Form For HFMDDocument2 pagesCase Report Form For HFMDMendez RhuNo ratings yet
- CRF HFMD AsmghDocument2 pagesCRF HFMD AsmghRyeowook RyeNo ratings yet
- Compulsory Health Certificate For Shri Amarnathji Yatra 2023Document1 pageCompulsory Health Certificate For Shri Amarnathji Yatra 2023Eknath KoliNo ratings yet
- Kardex: Date Ordere D Additional Orders Date Ordered Additional OrdersDocument14 pagesKardex: Date Ordere D Additional Orders Date Ordered Additional OrdersLRBNo ratings yet
- FWRI Form ReviseDocument3 pagesFWRI Form ReviseJm uniteNo ratings yet
- Form G Health Examination Report International StudentDocument6 pagesForm G Health Examination Report International StudentVictor OjukwuNo ratings yet
- General History and Physical Examination FormDocument2 pagesGeneral History and Physical Examination FormQueen Hera100% (1)
- St. Michael's Preparatory School: Health History FormDocument1 pageSt. Michael's Preparatory School: Health History FormJay309No ratings yet
- Acute Bloody Diarrhea - Ver Oct 12 2012Document2 pagesAcute Bloody Diarrhea - Ver Oct 12 2012rhu silagoNo ratings yet
- 11 Trauma Emergency Form 19102023Document2 pages11 Trauma Emergency Form 19102023Marjorie BricenioNo ratings yet
- Gym Member Registration FormDocument2 pagesGym Member Registration FormChethan Sharma RNo ratings yet
- Aefi CifDocument6 pagesAefi CifVic KwanNo ratings yet
- Pre Employment Medical Declaration Form - 2022Document2 pagesPre Employment Medical Declaration Form - 2022Neel GhoshNo ratings yet
- Physical Restraint Monitoring FormDocument1 pagePhysical Restraint Monitoring FormChandu Pandit100% (4)
- CHC Updated 2023Document1 pageCHC Updated 2023maheshmonu9449No ratings yet
- CHC Updated 2023Document1 pageCHC Updated 2023Vishal Singh ShekhawatNo ratings yet
- Natoza Medical Form For Grade 7 12Document3 pagesNatoza Medical Form For Grade 7 12Deonna AngelineNo ratings yet
- Referral Form Jessa 2021Document1 pageReferral Form Jessa 2021Jessa MaeNo ratings yet
- Lonpac Maid Medical ClaimDocument3 pagesLonpac Maid Medical ClaimYl EdianonNo ratings yet
- Medical CertificateDocument2 pagesMedical CertificatelekacaNo ratings yet
- Kolej Teknologi Darulnaim: Darulnaim College of TechnologyDocument5 pagesKolej Teknologi Darulnaim: Darulnaim College of TechnologyDaryanto SutejiNo ratings yet
- Medical CertificateDocument2 pagesMedical CertificateBalaziEswarNo ratings yet
- Medical Certificate 2Document2 pagesMedical Certificate 2Aditeya Shukla100% (1)
- FWRI 2023 CIF v2Document3 pagesFWRI 2023 CIF v2Terence John ChebatNo ratings yet
- Fwri Cif FormDocument3 pagesFwri Cif FormMHO GloriaNo ratings yet
- HMRM RECORD DoccDocument13 pagesHMRM RECORD DoccBharath BeeNo ratings yet
- One Step Med: General Medical Information Record Keeping ManualFrom EverandOne Step Med: General Medical Information Record Keeping ManualNo ratings yet
- I-C-E in Case of Emergency: Your Essential Medical JournalFrom EverandI-C-E in Case of Emergency: Your Essential Medical JournalNo ratings yet
- No Person Can Dispence Medicnine Other Then Reg PharmacistDocument22 pagesNo Person Can Dispence Medicnine Other Then Reg PharmacistSandeep PandeyNo ratings yet
- Ob Nursing Evaluation ToolDocument4 pagesOb Nursing Evaluation ToolLyra Mae E. MendozaNo ratings yet
- CBT - Nursing Care and Responsibility EditedDocument53 pagesCBT - Nursing Care and Responsibility Editedhimali ranasingheNo ratings yet
- Nothile XhakazaDocument3 pagesNothile XhakazaxhakazanondumisoNo ratings yet
- Master Rotation Plan For GNMDocument9 pagesMaster Rotation Plan For GNMAnanya HatiNo ratings yet
- Independent Medical Education - PfizerDocument6 pagesIndependent Medical Education - PfizerkelvinkinergyNo ratings yet
- Geriatrics 23 BrochureDocument5 pagesGeriatrics 23 BrochureMUHAMMAD09No ratings yet
- Resume & Portofolio Stefanus Nofa 2021Document4 pagesResume & Portofolio Stefanus Nofa 2021khrisnagungNo ratings yet
- Week 7 Primary Care Lecture To StudentsDocument63 pagesWeek 7 Primary Care Lecture To StudentsBoltNo ratings yet
- Lamaran - Produksi (Yusuf)Document3 pagesLamaran - Produksi (Yusuf)Salatiga ParamedicNo ratings yet
- Curriculum VitaeDocument3 pagesCurriculum VitaeOliver OsiroNo ratings yet
- DME Billing Services OverviewDocument6 pagesDME Billing Services OverviewINF HealthcareNo ratings yet
- Airline EssayDocument1 pageAirline EssayJhariel PeregrinaNo ratings yet
- IRDA - Claim Form-2Document1 pageIRDA - Claim Form-2Sunny bNo ratings yet
- Prince PDFDocument9 pagesPrince PDFNK NikhilNo ratings yet
- JacksonDocument2 pagesJacksonapi-641837495No ratings yet
- The United States Health Care System Combining Business Health and Delivery 2nd Edition Austin Test BankDocument11 pagesThe United States Health Care System Combining Business Health and Delivery 2nd Edition Austin Test Banklaylafarleyh3i8j9100% (26)
- 122-Article Text-453-1-10-20200622Document12 pages122-Article Text-453-1-10-20200622Real TetisoraNo ratings yet
- Log Book: Clinical Clerkship ProgramDocument16 pagesLog Book: Clinical Clerkship Programjayen_98No ratings yet
- HospitalDocument7 pagesHospitalJaikapil KachhawaNo ratings yet
- Weaving Traditional and Professional Midwifery - EditedDocument5 pagesWeaving Traditional and Professional Midwifery - EditedMAKOKHA BONFACENo ratings yet
- De-Empanelment 05.01.2023Document1 pageDe-Empanelment 05.01.2023Bhavani RentalaNo ratings yet
- NBHS2513 Professional Issues in HealthcareDocument13 pagesNBHS2513 Professional Issues in HealthcareSimon RajNo ratings yet
- AnnexC PC-HFDocument5 pagesAnnexC PC-HFJirhana Lindagan Karon-KampangNo ratings yet
- Ra-113838 Professional Teacher - Elementary Masbate 3-2023Document88 pagesRa-113838 Professional Teacher - Elementary Masbate 3-2023Jessa Marie JardinNo ratings yet
- Vaccination Sites Per Municipalities of South CotabatoDocument2 pagesVaccination Sites Per Municipalities of South CotabatoHEMS SOCOTNo ratings yet
- Sterling Roberts Resume DoneDocument2 pagesSterling Roberts Resume Doneapi-662884360No ratings yet
- CMS 1500 - 2012 - 0001Document4 pagesCMS 1500 - 2012 - 0001chamuditha dilshanNo ratings yet
- Trend Dan Isue Keperawatan KeluargaDocument15 pagesTrend Dan Isue Keperawatan KeluargaFebby WidiantoNo ratings yet