Download as pdf or txt
You might also like
- Beta Adrenergic Blockers: SympatholyticDocument12 pagesBeta Adrenergic Blockers: SympatholyticAbdullah asadNo ratings yet
- Adrenoceptor Antagonist Drugs-IIDocument14 pagesAdrenoceptor Antagonist Drugs-IIcelecosibNo ratings yet
- 3-11-2018 Beta Blocking DrugsDocument65 pages3-11-2018 Beta Blocking DrugsDharmendra GohilNo ratings yet
- β - BlockersDocument12 pagesβ - Blockersmohavi8169No ratings yet
- Beta-Blockers For Cardiovascular Conditions:: One Size Does Not Fit All PatientsDocument7 pagesBeta-Blockers For Cardiovascular Conditions:: One Size Does Not Fit All PatientsspalemaxNo ratings yet
- Propranolol Introduced in 1963 Was A Therapeutic BreakthroughDocument5 pagesPropranolol Introduced in 1963 Was A Therapeutic BreakthroughOmkar Singh100% (1)
- Pharma CVS LectureDocument14 pagesPharma CVS Lectureبصيص اليقينNo ratings yet
- Antiadrenergic Drugs - II 24.07.018 PDFDocument25 pagesAntiadrenergic Drugs - II 24.07.018 PDFHitesh karnNo ratings yet
- Antihypertensive Agents: Ayman Khdair Ph.D. Pharmaceutical Sciences Wayne State University, Michigan, USADocument15 pagesAntihypertensive Agents: Ayman Khdair Ph.D. Pharmaceutical Sciences Wayne State University, Michigan, USAJalil HaddadinNo ratings yet
- Adrenergic AntagonistDocument29 pagesAdrenergic AntagonistAreesha ArifNo ratings yet
- YogeshDocument49 pagesYogeshapi-3741769No ratings yet
- Antiadrenergic DrugsDocument44 pagesAntiadrenergic DrugsHUZAIFA YAMAANNo ratings yet
- Sympa T Holy TicsDocument30 pagesSympa T Holy TicsAhaisibwe GordonNo ratings yet
- Sympa T Holy TicsDocument47 pagesSympa T Holy Ticsahmad tariqNo ratings yet
- Beta BlockersDocument3 pagesBeta BlockersWil LesterNo ratings yet
- PFK BisoprololDocument10 pagesPFK BisoprololFelicia Aurelia SurbaktiNo ratings yet
- Adrenergic Blockers by Ms. MaidaDocument23 pagesAdrenergic Blockers by Ms. MaidaShimmering MoonNo ratings yet
- Atenolol: Atenolol Is A Beta Blocker MedicationDocument6 pagesAtenolol: Atenolol Is A Beta Blocker MedicationAbdelrhman AboodaNo ratings yet
- Beta Adrenergic Blockers ArvindDocument12 pagesBeta Adrenergic Blockers ArvindA2Z GyanNo ratings yet
- What Is AtenololDocument9 pagesWhat Is AtenololAbdelrhman AboodaNo ratings yet
- 13 Beta Adrenoceptor BlockersDocument35 pages13 Beta Adrenoceptor BlockersanojanNo ratings yet
- Antiadrenergic 180630054321Document19 pagesAntiadrenergic 180630054321Dinam Gyatso AadHenmooNo ratings yet
- PH 1.13:BETA Blockers: Dr. Lavakumar S Professor Dept of Pharmacology SssmcriDocument31 pagesPH 1.13:BETA Blockers: Dr. Lavakumar S Professor Dept of Pharmacology SssmcriBeena ShajimonNo ratings yet
- Beta Blockers: Dr. Mozna TalpurDocument12 pagesBeta Blockers: Dr. Mozna TalpurShahid HameedNo ratings yet
- Anti Hypertensive Interaction Part 1Document5 pagesAnti Hypertensive Interaction Part 1Abdulhameed MohamedNo ratings yet
- Drugs Without Positive Inotropic Effect Used in HFDocument12 pagesDrugs Without Positive Inotropic Effect Used in HFDana HamarshehNo ratings yet
- Different Calcium Channel BlockersDocument4 pagesDifferent Calcium Channel BlockersArnel Leonard TungbabanNo ratings yet
- Beta-Blockers: Beta-Blocker Options Following Funding Changes To Betaloc CRDocument12 pagesBeta-Blockers: Beta-Blocker Options Following Funding Changes To Betaloc CRDewi Nurul SakinahNo ratings yet
- Pharmacology Reviewer FinalsDocument4 pagesPharmacology Reviewer FinalsCielo SanchezNo ratings yet
- BB in HTN 2007Document69 pagesBB in HTN 2007doctopusNo ratings yet
- Beta BlockersDocument2 pagesBeta BlockersmetkosdNo ratings yet
- 6 SymaptholyticDocument48 pages6 SymaptholyticYoueel IbrahemNo ratings yet
- Beta Blockers BPTHDocument45 pagesBeta Blockers BPTHjyb5kcxbgtNo ratings yet
- Adrenergic AntagonistDocument30 pagesAdrenergic AntagonistOmar AlaamNo ratings yet
- BISOPROLOLDocument4 pagesBISOPROLOLHY Hong YiNo ratings yet
- 6 Beta Adrenergic BlockersDocument19 pages6 Beta Adrenergic Blockersmatchees-gone rogue100% (1)
- Beta BlockersDocument20 pagesBeta BlockersFarhat NaheedNo ratings yet
- Medical Therapy For Reduction of Intraocular PressureDocument42 pagesMedical Therapy For Reduction of Intraocular PressureHawwi IsmailNo ratings yet
- Cardiovascular Drugs - Nurse - DR DianDocument67 pagesCardiovascular Drugs - Nurse - DR DianAndyk Strapilococus Aureus100% (2)
- Major Side Effects of Beta Blockers - UpToDateDocument22 pagesMajor Side Effects of Beta Blockers - UpToDateJoão VictorNo ratings yet
- 64f361db-826c-41de-88c1-8005cada1108Document22 pages64f361db-826c-41de-88c1-8005cada1108Priya ChandelNo ratings yet
- Obat Antihypertensi: DR Med DR - Widharto PH, SPFK Farmakologi Dan Terapi Fak - Kedokteran UgmDocument38 pagesObat Antihypertensi: DR Med DR - Widharto PH, SPFK Farmakologi Dan Terapi Fak - Kedokteran UgmNi Made Dwiki AndriyaniNo ratings yet
- Pharmacology Cardiovascular DrugsDocument120 pagesPharmacology Cardiovascular DrugsDareRaymond100% (1)
- Beta BlockersDocument23 pagesBeta BlockersPriya ChandelNo ratings yet
- Beta Adrenoceptor BlockersDocument30 pagesBeta Adrenoceptor BlockersShihab AlmoliukiNo ratings yet
- Antihypertensives Summary Katzung PharmacologyDocument8 pagesAntihypertensives Summary Katzung PharmacologyRobin TolentinoNo ratings yet
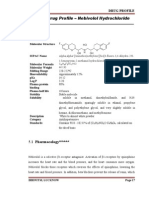
- Drug Profile NebivololDocument6 pagesDrug Profile NebivololKrista ColeNo ratings yet
- Butisol Sodium: (Butabarbital Sodium Tablets, USP and Butabarbital Sodium Oral Solution, USP) Tablets & Oral SolutionDocument5 pagesButisol Sodium: (Butabarbital Sodium Tablets, USP and Butabarbital Sodium Oral Solution, USP) Tablets & Oral SolutionBrian HarrisNo ratings yet
- methotrexate-Anti-Asthmatic Drugs Toxicity-1Document9 pagesmethotrexate-Anti-Asthmatic Drugs Toxicity-1joonabil29No ratings yet
- Beta-Adrenergic Receptor AntagonistsDocument5 pagesBeta-Adrenergic Receptor AntagonistsKabwe BrandonNo ratings yet
- Pharma Unit 8 - Anti - Adrenergic Drugs - 2 of 2Document21 pagesPharma Unit 8 - Anti - Adrenergic Drugs - 2 of 2MIbrahimNo ratings yet
- S 026 LBLDocument23 pagesS 026 LBLAhsan KhanNo ratings yet
- Alpha Blockers PharmacologyDocument23 pagesAlpha Blockers PharmacologyHesbon MomanyiNo ratings yet
- سموم نظري٤Document6 pagesسموم نظري٤مصطفى ابراهيم سعيدNo ratings yet
- Adrenoceptor BlockersDocument53 pagesAdrenoceptor Blockersesra1altahirNo ratings yet
- SympatholyticsDocument46 pagesSympatholyticsHari Kamesh KiranNo ratings yet
- Bisoprolol FumaratDocument12 pagesBisoprolol FumaratSan-Clin-Eq LaboratoryNo ratings yet
- Beta Blockers Nebivolol, C H F NO: Chemical StructureDocument3 pagesBeta Blockers Nebivolol, C H F NO: Chemical StructurechatofficialNo ratings yet
- Nebivolol. Does the key lie in β3 agonismDocument6 pagesNebivolol. Does the key lie in β3 agonismAzad MəmmədovNo ratings yet
- Nada Lincomycyn and Espectynomycin Solubleucm061812Document4 pagesNada Lincomycyn and Espectynomycin Solubleucm061812laurz95No ratings yet
- PRICE LIST 21 22 HBM - 150822 No MRP 1Document10 pagesPRICE LIST 21 22 HBM - 150822 No MRP 1Mayur MulyeNo ratings yet
- A Detailed Lesson Plan in MAPEH Sample 2010Document3 pagesA Detailed Lesson Plan in MAPEH Sample 2010Estrella P. Agot0% (1)
- DulcolaxDocument1 pageDulcolaxKatie McPeekNo ratings yet
- DX StdieDocument22 pagesDX Stdietimie_reyesNo ratings yet
- New 2008Document33 pagesNew 2008Kathryn MitchellNo ratings yet
- New Materi Pretest Skill Blok 10Document3 pagesNew Materi Pretest Skill Blok 10asabri yunisNo ratings yet
- Antibacerials PharmacolgyDocument53 pagesAntibacerials PharmacolgyHamid AryanNo ratings yet
- MasterDataObat 27072020Document300 pagesMasterDataObat 27072020Bogi Aditya PermanaNo ratings yet
- Local Anaesthetics: Dr. R. Jamuna Rani MD, Professor & HOD, Department of PharmacologyDocument25 pagesLocal Anaesthetics: Dr. R. Jamuna Rani MD, Professor & HOD, Department of PharmacologyAimee Ann MacaraegNo ratings yet
- M.I. (Losartan) Drug Study)Document2 pagesM.I. (Losartan) Drug Study)Angelica Marie MacaslingNo ratings yet
- Videsh PrintingDocument22 pagesVidesh PrintingAbroadnayak KumarNo ratings yet
- Antiepilepsy Drugs: Pharmacodynamics and Principles of Drug SelectionDocument22 pagesAntiepilepsy Drugs: Pharmacodynamics and Principles of Drug SelectionNaela RizqiNo ratings yet
- Michael Jackson: Death by Drugs Project Created By: Elizabeth Lux Period 4/5Document7 pagesMichael Jackson: Death by Drugs Project Created By: Elizabeth Lux Period 4/5Elizabeth LuxNo ratings yet
- Pharmaceutics Is The Discipline of Pharmacy That Deals With The Process of Turning ADocument6 pagesPharmaceutics Is The Discipline of Pharmacy That Deals With The Process of Turning ANGMC Clinical TrialNo ratings yet
- Antibiotics 11.05.19Document18 pagesAntibiotics 11.05.19dahiphale1No ratings yet
- Prescription 2: Ingredient Physical Description Solubility Dose Comparison Given UsualDocument4 pagesPrescription 2: Ingredient Physical Description Solubility Dose Comparison Given UsualRhonabelle DadulaNo ratings yet
- WHO Guide For Rabies Pre and Post Exposure Prophylaxis in HumansDocument29 pagesWHO Guide For Rabies Pre and Post Exposure Prophylaxis in HumansMacky YongcoNo ratings yet
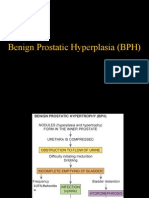
- BPH and TreatmentDocument36 pagesBPH and TreatmentSyokoyolanting Dondon0% (1)
- Day1.5 - Shaw - Drug Master File (DMF) BasicsDocument48 pagesDay1.5 - Shaw - Drug Master File (DMF) BasicsMarkbot1999No ratings yet
- Early Efficacy and Safety of Bedaquiline and Delamanid Given Together in A "Salvage Regimen" For Treatment of Drug-Resistant TuberculosisDocument5 pagesEarly Efficacy and Safety of Bedaquiline and Delamanid Given Together in A "Salvage Regimen" For Treatment of Drug-Resistant Tuberculosisadila awaludinNo ratings yet
- Dosage Lec - Unit 2 Drug DiscoveryDocument8 pagesDosage Lec - Unit 2 Drug DiscoveryJohn Lorenz BordadorNo ratings yet
- UMUMDocument166 pagesUMUMakun rsiNo ratings yet
- Recalls Kaps Dec 2017Document7 pagesRecalls Kaps Dec 2017BincyBenjaminNo ratings yet
- Absorption and Half-Life: Nick Holford Dept Pharmacology & Clinical Pharmacology University of Auckland, New ZealandDocument7 pagesAbsorption and Half-Life: Nick Holford Dept Pharmacology & Clinical Pharmacology University of Auckland, New ZealandkbnarkhedeNo ratings yet
- Cannabis Oil: Chemical Evaluation of An Upcoming Cannabis-Based MedicineDocument3 pagesCannabis Oil: Chemical Evaluation of An Upcoming Cannabis-Based MedicineAllyson CarlosNo ratings yet
- Solomon 2006Document5 pagesSolomon 2006Ottofianus Hewick KalangiNo ratings yet
- MenopauseDocument15 pagesMenopauseTomiNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsK1K5KNo ratings yet
- Drugs Acting On The Autonomic Nervous SystemDocument68 pagesDrugs Acting On The Autonomic Nervous SystemjisooNo ratings yet