
Form-039-Hydrostatic Testing Work Permit
Form-039-Hydrostatic Testing Work Permit
You might also like
- July 23, 2009 Through August 24, 2009 JPMorgan Chase BankDocument4 pagesJuly 23, 2009 Through August 24, 2009 JPMorgan Chase BankMaria Blackburn33% (3)
- Case Study #4 The Case of Joe and BlakeDocument3 pagesCase Study #4 The Case of Joe and BlakeJacques TuckerNo ratings yet
- Reborn Apocalypse (A LitRPGWuxia Story) (Volume 1) (Kerr L.M.)Document515 pagesReborn Apocalypse (A LitRPGWuxia Story) (Volume 1) (Kerr L.M.)julian vegaNo ratings yet
- General Work PermitDocument1 pageGeneral Work PermitJohn Shane100% (5)
- E I P / E P: Project/LocationDocument2 pagesE I P / E P: Project/LocationAsad Maher100% (3)
- Well Testing Project Management: Onshore and Offshore OperationsFrom EverandWell Testing Project Management: Onshore and Offshore OperationsNo ratings yet
- FB EK Holden NASCO Windshield Washer Enthusiasts GuideDocument53 pagesFB EK Holden NASCO Windshield Washer Enthusiasts Guideandrewbower2100% (3)
- Industrial Applications of Infrared Thermography: How Infrared Analysis Can be Used to Improve Equipment InspectionFrom EverandIndustrial Applications of Infrared Thermography: How Infrared Analysis Can be Used to Improve Equipment InspectionRating: 4.5 out of 5 stars4.5/5 (3)
- IDI-FRM-HSE-32-01 Permit To Work - Electrical WorkDocument1 pageIDI-FRM-HSE-32-01 Permit To Work - Electrical Workaulia chaniaNo ratings yet
- 47.HDEC-HSE-F0047 Pressure Test PermitDocument1 page47.HDEC-HSE-F0047 Pressure Test PermitRonn CaiNo ratings yet
- Form 33 Electrical Isolation Testing PermitDocument1 pageForm 33 Electrical Isolation Testing PermitRoshan ZameerNo ratings yet
- General Electric Work Permit - Attachment XXIIDocument2 pagesGeneral Electric Work Permit - Attachment XXIIFaiqah Azmir100% (1)
- Hot Work PermitDocument1 pageHot Work PermitManesh MNo ratings yet
- Cold WP PWIE 27 - 10 - 20 Access ControlDocument2 pagesCold WP PWIE 27 - 10 - 20 Access ControlHBHJBMNNo ratings yet
- Electrical Isolation Work PermitDocument2 pagesElectrical Isolation Work PermitRobby TriNo ratings yet
- Excavaten Work PermitDocument1 pageExcavaten Work Permitasem sawalmehNo ratings yet
- CP 01-2 Hot Work Permit STTGDCDocument2 pagesCP 01-2 Hot Work Permit STTGDCsttkolkataNo ratings yet
- Live Testing - Take 5 Rev EDocument2 pagesLive Testing - Take 5 Rev EVicky JiNo ratings yet
- Pressure Testing Permit: (M) Mandatory RequirementDocument2 pagesPressure Testing Permit: (M) Mandatory RequirementRajesh KumarNo ratings yet
- General Permit To WorkDocument2 pagesGeneral Permit To WorkMuhammad Mas'abNo ratings yet
- Lifting Activity Permit To WorkDocument1 pageLifting Activity Permit To WorkBig ZaddyNo ratings yet
- 001 - Safe Work Permit Form - R2Document2 pages001 - Safe Work Permit Form - R2John Renz Caling RetiroNo ratings yet
- Victoria Health Centre - Fire Curtain - TestsheetsDocument3 pagesVictoria Health Centre - Fire Curtain - TestsheetsYlenia BonelloNo ratings yet
- Cme Iraq CF Oi 5 1 Cold Work PermitDocument1 pageCme Iraq CF Oi 5 1 Cold Work Permitmurtadanajem1999No ratings yet
- EBENCO FACILITY Hot Work PermitDocument2 pagesEBENCO FACILITY Hot Work PermitLateef RaifuNo ratings yet
- Energisation PermitDocument1 pageEnergisation Permitamenmohamm3dNo ratings yet
- HSE 14 Lockout and TagoutDocument1 pageHSE 14 Lockout and TagoutBa N Nhim100% (1)
- Form 0004: Confined Space Permit: Section - I Details of The Permit Issuer & ReciverDocument1 pageForm 0004: Confined Space Permit: Section - I Details of The Permit Issuer & Reciverasem sawalmehNo ratings yet
- Ho 96Document1 pageHo 96Shanmugam AnnamalaiNo ratings yet
- Night Work PermitDocument2 pagesNight Work PermitsttkolkataNo ratings yet
- Work at HeightDocument2 pagesWork at Heightmassmoudi58No ratings yet
- Form 0005: Hot Work Permit: Section - I Details of The Permit ReciverDocument1 pageForm 0005: Hot Work Permit: Section - I Details of The Permit Reciverasem sawalmehNo ratings yet
- SA-S-107-01-01 Electrical Permit To Work - PTW (B.1) 14 - 26 OCT 2022Document2 pagesSA-S-107-01-01 Electrical Permit To Work - PTW (B.1) 14 - 26 OCT 2022karla.adamesNo ratings yet
- Bhate & Raje Construction Co. Pvt. LTD: Electrical Work PermitDocument1 pageBhate & Raje Construction Co. Pvt. LTD: Electrical Work Permitvinayak salve100% (1)
- 17 - Pressure Testing Permit (A4)Document1 page17 - Pressure Testing Permit (A4)Jianping KeNo ratings yet
- HSE 10 Excavation PermitDocument1 pageHSE 10 Excavation PermitBa N Nhim100% (1)
- Hot Work PermitDocument2 pagesHot Work PermitMusadiq HussainNo ratings yet
- HSE 09 Hotwork PermitDocument1 pageHSE 09 Hotwork PermitBa N Nhim100% (1)
- Masa Permit To Work CertificateDocument2 pagesMasa Permit To Work CertificateUsman ManiNo ratings yet
- PTW - Restricted AreaDocument2 pagesPTW - Restricted Areasarath SNo ratings yet
- V012 SCT CO000 0071 02 Crane Operation PermitDocument2 pagesV012 SCT CO000 0071 02 Crane Operation PermitshamsuddinNo ratings yet
- 10-TEC-BFM-F24 - Access Permit - R7 Dec 5 2020Document1 page10-TEC-BFM-F24 - Access Permit - R7 Dec 5 2020Design Xess EventsNo ratings yet
- Hot Work - Permit To WorkDocument1 pageHot Work - Permit To WorkBig ZaddyNo ratings yet
- Work at Height - Permit To WorkDocument1 pageWork at Height - Permit To WorkBig ZaddyNo ratings yet
- Work Permit - Ionizing Radiation: Work Should Not Commence Until Stages 1 To 5 Are CompletedDocument2 pagesWork Permit - Ionizing Radiation: Work Should Not Commence Until Stages 1 To 5 Are CompletedIonian TribeNo ratings yet
- Ptw-Kec - Final v3 - SparkDocument1 pagePtw-Kec - Final v3 - SparkXiang JintaoNo ratings yet
- Isolation Work PermitDocument2 pagesIsolation Work PermitVijayakumar KarunanidhiNo ratings yet
- Ho 87Document1 pageHo 87Shanmugam AnnamalaiNo ratings yet
- AM-HSE-MP-07-F15-Access PermitDocument1 pageAM-HSE-MP-07-F15-Access PermitNajmal AmanNo ratings yet
- PTW Associated Certificates KEC - Final v3-MECHANICALDocument3 pagesPTW Associated Certificates KEC - Final v3-MECHANICALXiang JintaoNo ratings yet
- PTW Associated Certificates KEC - Final V3-TotalDocument9 pagesPTW Associated Certificates KEC - Final V3-TotalXiang JintaoNo ratings yet
- PCD-OSH-SF-35 PTW For Confine SpaceDocument2 pagesPCD-OSH-SF-35 PTW For Confine Spacerizal azizanNo ratings yet
- General Work PermitDocument2 pagesGeneral Work PermitJareem PeesNo ratings yet
- Ho 91Document1 pageHo 91Shanmugam AnnamalaiNo ratings yet
- Mobile Crane Work PermitDocument2 pagesMobile Crane Work PermitprabhuNo ratings yet
- Electrical Permit To WorkDocument2 pagesElectrical Permit To Workimranul haqNo ratings yet
- Adobe Scan Dec 29, 2022Document3 pagesAdobe Scan Dec 29, 2022SelvamNo ratings yet
- Hot Work Permit (Supplementary Permit)Document1 pageHot Work Permit (Supplementary Permit)skskNo ratings yet
- AM-HSE-MP-07-F15-Access PermitDocument1 pageAM-HSE-MP-07-F15-Access PermitNajmal AmanNo ratings yet
- PTW-02 Hot Work PermitDocument4 pagesPTW-02 Hot Work PermitjayNo ratings yet
- PTW - Electrical PermitDocument2 pagesPTW - Electrical PermitJahanzaib KhanNo ratings yet
- Hotworks PermitDocument1 pageHotworks PermitGlorieNo ratings yet
- The Sarbanes-Oxley Section 404 Implementation Toolkit: Practice Aids for Managers and AuditorsFrom EverandThe Sarbanes-Oxley Section 404 Implementation Toolkit: Practice Aids for Managers and AuditorsNo ratings yet
- 121 HSE Alert - Electrical Cable DamagesDocument1 page121 HSE Alert - Electrical Cable DamagesJohn Vincent Macatangay CleofeNo ratings yet
- Form-133-Specific Job Site TrainingDocument1 pageForm-133-Specific Job Site TrainingJohn Vincent Macatangay CleofeNo ratings yet
- Form-132-Safety Induction Attendance SheetDocument1 pageForm-132-Safety Induction Attendance SheetJohn Vincent Macatangay CleofeNo ratings yet
- Form-131-Tool Box Talk Attendance SheetDocument1 pageForm-131-Tool Box Talk Attendance SheetJohn Vincent Macatangay CleofeNo ratings yet
- KPI Form - ConstructionDocument1 pageKPI Form - ConstructionJohn Vincent Macatangay CleofeNo ratings yet
- Imrovement Action Plan - Utility Strike - 16 Feb 2020Document38 pagesImrovement Action Plan - Utility Strike - 16 Feb 2020John Vincent Macatangay CleofeNo ratings yet
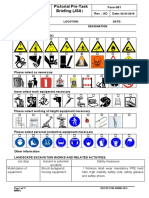
- Landscape Form-051-Pictorial Pre-Task Briefing (JSA) 19 Oct 2019 - FinalDocument17 pagesLandscape Form-051-Pictorial Pre-Task Briefing (JSA) 19 Oct 2019 - FinalJohn Vincent Macatangay Cleofe100% (1)
- Utilities Department Utility Strikes Improvement Action 1Document7 pagesUtilities Department Utility Strikes Improvement Action 1John Vincent Macatangay CleofeNo ratings yet
- Corrective Action Report (Car) : Hse Line 6 Fast Metro ProjectDocument5 pagesCorrective Action Report (Car) : Hse Line 6 Fast Metro ProjectJohn Vincent Macatangay CleofeNo ratings yet
- 2014pe Part IDocument12 pages2014pe Part IJohn Vincent Macatangay CleofeNo ratings yet
- 14-08-2020 - 2200 Hrs - LS 4G1 - DO - Fire Fighting PVC Pipe - DraftDocument12 pages14-08-2020 - 2200 Hrs - LS 4G1 - DO - Fire Fighting PVC Pipe - DraftJohn Vincent Macatangay CleofeNo ratings yet
- Corrective Action Report (Car) : Hse Line 6 Fast Metro ProjectDocument2 pagesCorrective Action Report (Car) : Hse Line 6 Fast Metro ProjectJohn Vincent Macatangay CleofeNo ratings yet
- Engineer & Supervisors List - LANDSCAPEDocument2 pagesEngineer & Supervisors List - LANDSCAPEJohn Vincent Macatangay CleofeNo ratings yet
- CONTROLDocument194 pagesCONTROLJohn Vincent Macatangay CleofeNo ratings yet
- Ser Line Exact Location Serial Number SupplierDocument8 pagesSer Line Exact Location Serial Number SupplierJohn Vincent Macatangay CleofeNo ratings yet
- Flood INDEXDocument171 pagesFlood INDEXJohn Vincent Macatangay CleofeNo ratings yet
- Protection in PlatDocument88 pagesProtection in PlatJohn Vincent Macatangay CleofeNo ratings yet
- Corrective Action Report (Car) : Hse Line 6 Fast Metro ProjectDocument3 pagesCorrective Action Report (Car) : Hse Line 6 Fast Metro ProjectJohn Vincent Macatangay CleofeNo ratings yet
- Line 04-LS/SS Schedule Section Finish Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov DecDocument5 pagesLine 04-LS/SS Schedule Section Finish Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov DecJohn Vincent Macatangay CleofeNo ratings yet
- Eyad-Swareb@sauditumpane, Com Andres - Deharo@fcc - Es No Work As of NowDocument1 pageEyad-Swareb@sauditumpane, Com Andres - Deharo@fcc - Es No Work As of NowJohn Vincent Macatangay CleofeNo ratings yet
- Note 4B1 Storm Water TrenchDocument2 pagesNote 4B1 Storm Water TrenchJohn Vincent Macatangay CleofeNo ratings yet
- Electrical Installation Inspection CARDocument3 pagesElectrical Installation Inspection CARJohn Vincent Macatangay CleofeNo ratings yet
- Corrective Action Report (Car) : Hse Line 6 Fast Metro ProjectDocument2 pagesCorrective Action Report (Car) : Hse Line 6 Fast Metro ProjectJohn Vincent Macatangay CleofeNo ratings yet
- Welcome To The LTE CPE!: Online HelpDocument44 pagesWelcome To The LTE CPE!: Online HelpJohn Vincent Macatangay CleofeNo ratings yet
- Updated Emergency Contact - Docx2 (2) 4b1 A3Document1 pageUpdated Emergency Contact - Docx2 (2) 4b1 A3John Vincent Macatangay CleofeNo ratings yet
- List of Short-Term Courses (TR) No. of Hours Fee Down PaymentDocument1 pageList of Short-Term Courses (TR) No. of Hours Fee Down PaymentJohn Vincent Macatangay CleofeNo ratings yet
- The Mechanical Properties of Polypropylene - Polylactic Acid (PP-PLA) Polymer Blends - 24 PagesDocument24 pagesThe Mechanical Properties of Polypropylene - Polylactic Acid (PP-PLA) Polymer Blends - 24 PagesSiddharthBhasneyNo ratings yet
- 1 Management Theories and PracticesDocument96 pages1 Management Theories and PracticesAsegid H/meskelNo ratings yet
- Case StudyDocument2 pagesCase StudyJoshua LaxamanaNo ratings yet
- Surajs Nair Resume 5Document4 pagesSurajs Nair Resume 5suraj.sNo ratings yet
- Sub District Sub Divisional HospitalDocument102 pagesSub District Sub Divisional HospitalGanesh SoniNo ratings yet
- QuadEquations PPT Alg2Document16 pagesQuadEquations PPT Alg2Kenny Ann Grace BatiancilaNo ratings yet
- Combustion Products From Ventilation Controlled Fires - Thesis PDFDocument321 pagesCombustion Products From Ventilation Controlled Fires - Thesis PDFYuri SanchezNo ratings yet
- Vendor Security Due Diligence ChecklistDocument9 pagesVendor Security Due Diligence ChecklistSukhveer SinghNo ratings yet
- Historical Change and Ceramic Tradition: The Case of Macedonia - Zoi KotitsaDocument15 pagesHistorical Change and Ceramic Tradition: The Case of Macedonia - Zoi KotitsaSonjce Marceva100% (2)
- DIY GREENHOUSE by KMS - ChangelogDocument4 pagesDIY GREENHOUSE by KMS - Changeloglm pronNo ratings yet
- De Thi Thu TN THPT 2024 Tieng Anh So GD Ha NoiDocument23 pagesDe Thi Thu TN THPT 2024 Tieng Anh So GD Ha NoiQuang Lê Hồ DuyNo ratings yet
- Crochetpatternturttle BenjaminDocument10 pagesCrochetpatternturttle BenjaminTere VValle100% (2)
- Research Compilation FinalDocument23 pagesResearch Compilation FinalJessa Mae LoredoNo ratings yet
- Driver Licence & Learner Permit FeesDocument9 pagesDriver Licence & Learner Permit FeesAnatoly IvanovNo ratings yet
- Technical CAPS Technical ScienceDocument84 pagesTechnical CAPS Technical ScienceqanaqNo ratings yet
- EDFD 211: Psychological Foundations in Education First Semester SY 2016-17 Course DescriptionDocument4 pagesEDFD 211: Psychological Foundations in Education First Semester SY 2016-17 Course DescriptionLeezl Campoamor OlegarioNo ratings yet
- IoT - Internet of Things Based Energy Management For Smart HomeDocument4 pagesIoT - Internet of Things Based Energy Management For Smart HomeEditor IJTSRDNo ratings yet
- Breach of ContractDocument26 pagesBreach of ContractSandeep100% (1)
- Aiga 097-17 Ref Guide On Medical Gases Cylinder ValvesDocument7 pagesAiga 097-17 Ref Guide On Medical Gases Cylinder ValvesDeepakNo ratings yet
- Surbir Singh Negi: Surbir99 - Negi@yahoo - Co.in, Surbir - Negi1@yahoo - Co.inDocument3 pagesSurbir Singh Negi: Surbir99 - Negi@yahoo - Co.in, Surbir - Negi1@yahoo - Co.insurbir_negi1100% (2)
- Fanuc 0ieDocument12 pagesFanuc 0ieangelNo ratings yet
- Siliporite Opx Pellets Revision 11 - 2017Document2 pagesSiliporite Opx Pellets Revision 11 - 2017Juan Victor Sulvaran Arellano100% (2)
- Ques Risk and Return & CAPM (S-17Revised)Document6 pagesQues Risk and Return & CAPM (S-17Revised)Najia SiddiquiNo ratings yet
- Guide To Supply Chain Management RemediationV2Document26 pagesGuide To Supply Chain Management RemediationV2Andrada-DianaFilipciucNo ratings yet
- PSI Framework Components - EnglishDocument20 pagesPSI Framework Components - Englishalejandrosag0% (1)
- Trophy Urban Core Property: Houston, TexasDocument25 pagesTrophy Urban Core Property: Houston, Texasbella grandeNo ratings yet













































































































Download as doc, pdf, or txt
You might also like
- July 23, 2009 Through August 24, 2009 JPMorgan Chase BankDocument4 pagesJuly 23, 2009 Through August 24, 2009 JPMorgan Chase BankMaria Blackburn33% (3)
- Case Study #4 The Case of Joe and BlakeDocument3 pagesCase Study #4 The Case of Joe and BlakeJacques TuckerNo ratings yet
- Reborn Apocalypse (A LitRPGWuxia Story) (Volume 1) (Kerr L.M.)Document515 pagesReborn Apocalypse (A LitRPGWuxia Story) (Volume 1) (Kerr L.M.)julian vegaNo ratings yet
- General Work PermitDocument1 pageGeneral Work PermitJohn Shane100% (5)
- E I P / E P: Project/LocationDocument2 pagesE I P / E P: Project/LocationAsad Maher100% (3)
- Well Testing Project Management: Onshore and Offshore OperationsFrom EverandWell Testing Project Management: Onshore and Offshore OperationsNo ratings yet
- FB EK Holden NASCO Windshield Washer Enthusiasts GuideDocument53 pagesFB EK Holden NASCO Windshield Washer Enthusiasts Guideandrewbower2100% (3)
- Industrial Applications of Infrared Thermography: How Infrared Analysis Can be Used to Improve Equipment InspectionFrom EverandIndustrial Applications of Infrared Thermography: How Infrared Analysis Can be Used to Improve Equipment InspectionRating: 4.5 out of 5 stars4.5/5 (3)
- IDI-FRM-HSE-32-01 Permit To Work - Electrical WorkDocument1 pageIDI-FRM-HSE-32-01 Permit To Work - Electrical Workaulia chaniaNo ratings yet
- 47.HDEC-HSE-F0047 Pressure Test PermitDocument1 page47.HDEC-HSE-F0047 Pressure Test PermitRonn CaiNo ratings yet
- Form 33 Electrical Isolation Testing PermitDocument1 pageForm 33 Electrical Isolation Testing PermitRoshan ZameerNo ratings yet
- General Electric Work Permit - Attachment XXIIDocument2 pagesGeneral Electric Work Permit - Attachment XXIIFaiqah Azmir100% (1)
- Hot Work PermitDocument1 pageHot Work PermitManesh MNo ratings yet
- Cold WP PWIE 27 - 10 - 20 Access ControlDocument2 pagesCold WP PWIE 27 - 10 - 20 Access ControlHBHJBMNNo ratings yet
- Electrical Isolation Work PermitDocument2 pagesElectrical Isolation Work PermitRobby TriNo ratings yet
- Excavaten Work PermitDocument1 pageExcavaten Work Permitasem sawalmehNo ratings yet
- CP 01-2 Hot Work Permit STTGDCDocument2 pagesCP 01-2 Hot Work Permit STTGDCsttkolkataNo ratings yet
- Live Testing - Take 5 Rev EDocument2 pagesLive Testing - Take 5 Rev EVicky JiNo ratings yet
- Pressure Testing Permit: (M) Mandatory RequirementDocument2 pagesPressure Testing Permit: (M) Mandatory RequirementRajesh KumarNo ratings yet
- General Permit To WorkDocument2 pagesGeneral Permit To WorkMuhammad Mas'abNo ratings yet
- Lifting Activity Permit To WorkDocument1 pageLifting Activity Permit To WorkBig ZaddyNo ratings yet
- 001 - Safe Work Permit Form - R2Document2 pages001 - Safe Work Permit Form - R2John Renz Caling RetiroNo ratings yet
- Victoria Health Centre - Fire Curtain - TestsheetsDocument3 pagesVictoria Health Centre - Fire Curtain - TestsheetsYlenia BonelloNo ratings yet
- Cme Iraq CF Oi 5 1 Cold Work PermitDocument1 pageCme Iraq CF Oi 5 1 Cold Work Permitmurtadanajem1999No ratings yet
- EBENCO FACILITY Hot Work PermitDocument2 pagesEBENCO FACILITY Hot Work PermitLateef RaifuNo ratings yet
- Energisation PermitDocument1 pageEnergisation Permitamenmohamm3dNo ratings yet
- HSE 14 Lockout and TagoutDocument1 pageHSE 14 Lockout and TagoutBa N Nhim100% (1)
- Form 0004: Confined Space Permit: Section - I Details of The Permit Issuer & ReciverDocument1 pageForm 0004: Confined Space Permit: Section - I Details of The Permit Issuer & Reciverasem sawalmehNo ratings yet
- Ho 96Document1 pageHo 96Shanmugam AnnamalaiNo ratings yet
- Night Work PermitDocument2 pagesNight Work PermitsttkolkataNo ratings yet
- Work at HeightDocument2 pagesWork at Heightmassmoudi58No ratings yet
- Form 0005: Hot Work Permit: Section - I Details of The Permit ReciverDocument1 pageForm 0005: Hot Work Permit: Section - I Details of The Permit Reciverasem sawalmehNo ratings yet
- SA-S-107-01-01 Electrical Permit To Work - PTW (B.1) 14 - 26 OCT 2022Document2 pagesSA-S-107-01-01 Electrical Permit To Work - PTW (B.1) 14 - 26 OCT 2022karla.adamesNo ratings yet
- Bhate & Raje Construction Co. Pvt. LTD: Electrical Work PermitDocument1 pageBhate & Raje Construction Co. Pvt. LTD: Electrical Work Permitvinayak salve100% (1)
- 17 - Pressure Testing Permit (A4)Document1 page17 - Pressure Testing Permit (A4)Jianping KeNo ratings yet
- HSE 10 Excavation PermitDocument1 pageHSE 10 Excavation PermitBa N Nhim100% (1)
- Hot Work PermitDocument2 pagesHot Work PermitMusadiq HussainNo ratings yet
- HSE 09 Hotwork PermitDocument1 pageHSE 09 Hotwork PermitBa N Nhim100% (1)
- Masa Permit To Work CertificateDocument2 pagesMasa Permit To Work CertificateUsman ManiNo ratings yet
- PTW - Restricted AreaDocument2 pagesPTW - Restricted Areasarath SNo ratings yet
- V012 SCT CO000 0071 02 Crane Operation PermitDocument2 pagesV012 SCT CO000 0071 02 Crane Operation PermitshamsuddinNo ratings yet
- 10-TEC-BFM-F24 - Access Permit - R7 Dec 5 2020Document1 page10-TEC-BFM-F24 - Access Permit - R7 Dec 5 2020Design Xess EventsNo ratings yet
- Hot Work - Permit To WorkDocument1 pageHot Work - Permit To WorkBig ZaddyNo ratings yet
- Work at Height - Permit To WorkDocument1 pageWork at Height - Permit To WorkBig ZaddyNo ratings yet
- Work Permit - Ionizing Radiation: Work Should Not Commence Until Stages 1 To 5 Are CompletedDocument2 pagesWork Permit - Ionizing Radiation: Work Should Not Commence Until Stages 1 To 5 Are CompletedIonian TribeNo ratings yet
- Ptw-Kec - Final v3 - SparkDocument1 pagePtw-Kec - Final v3 - SparkXiang JintaoNo ratings yet
- Isolation Work PermitDocument2 pagesIsolation Work PermitVijayakumar KarunanidhiNo ratings yet
- Ho 87Document1 pageHo 87Shanmugam AnnamalaiNo ratings yet
- AM-HSE-MP-07-F15-Access PermitDocument1 pageAM-HSE-MP-07-F15-Access PermitNajmal AmanNo ratings yet
- PTW Associated Certificates KEC - Final v3-MECHANICALDocument3 pagesPTW Associated Certificates KEC - Final v3-MECHANICALXiang JintaoNo ratings yet
- PTW Associated Certificates KEC - Final V3-TotalDocument9 pagesPTW Associated Certificates KEC - Final V3-TotalXiang JintaoNo ratings yet
- PCD-OSH-SF-35 PTW For Confine SpaceDocument2 pagesPCD-OSH-SF-35 PTW For Confine Spacerizal azizanNo ratings yet
- General Work PermitDocument2 pagesGeneral Work PermitJareem PeesNo ratings yet
- Ho 91Document1 pageHo 91Shanmugam AnnamalaiNo ratings yet
- Mobile Crane Work PermitDocument2 pagesMobile Crane Work PermitprabhuNo ratings yet
- Electrical Permit To WorkDocument2 pagesElectrical Permit To Workimranul haqNo ratings yet
- Adobe Scan Dec 29, 2022Document3 pagesAdobe Scan Dec 29, 2022SelvamNo ratings yet
- Hot Work Permit (Supplementary Permit)Document1 pageHot Work Permit (Supplementary Permit)skskNo ratings yet
- AM-HSE-MP-07-F15-Access PermitDocument1 pageAM-HSE-MP-07-F15-Access PermitNajmal AmanNo ratings yet
- PTW-02 Hot Work PermitDocument4 pagesPTW-02 Hot Work PermitjayNo ratings yet
- PTW - Electrical PermitDocument2 pagesPTW - Electrical PermitJahanzaib KhanNo ratings yet
- Hotworks PermitDocument1 pageHotworks PermitGlorieNo ratings yet
- The Sarbanes-Oxley Section 404 Implementation Toolkit: Practice Aids for Managers and AuditorsFrom EverandThe Sarbanes-Oxley Section 404 Implementation Toolkit: Practice Aids for Managers and AuditorsNo ratings yet
- 121 HSE Alert - Electrical Cable DamagesDocument1 page121 HSE Alert - Electrical Cable DamagesJohn Vincent Macatangay CleofeNo ratings yet
- Form-133-Specific Job Site TrainingDocument1 pageForm-133-Specific Job Site TrainingJohn Vincent Macatangay CleofeNo ratings yet
- Form-132-Safety Induction Attendance SheetDocument1 pageForm-132-Safety Induction Attendance SheetJohn Vincent Macatangay CleofeNo ratings yet
- Form-131-Tool Box Talk Attendance SheetDocument1 pageForm-131-Tool Box Talk Attendance SheetJohn Vincent Macatangay CleofeNo ratings yet
- KPI Form - ConstructionDocument1 pageKPI Form - ConstructionJohn Vincent Macatangay CleofeNo ratings yet
- Imrovement Action Plan - Utility Strike - 16 Feb 2020Document38 pagesImrovement Action Plan - Utility Strike - 16 Feb 2020John Vincent Macatangay CleofeNo ratings yet
- Landscape Form-051-Pictorial Pre-Task Briefing (JSA) 19 Oct 2019 - FinalDocument17 pagesLandscape Form-051-Pictorial Pre-Task Briefing (JSA) 19 Oct 2019 - FinalJohn Vincent Macatangay Cleofe100% (1)
- Utilities Department Utility Strikes Improvement Action 1Document7 pagesUtilities Department Utility Strikes Improvement Action 1John Vincent Macatangay CleofeNo ratings yet
- Corrective Action Report (Car) : Hse Line 6 Fast Metro ProjectDocument5 pagesCorrective Action Report (Car) : Hse Line 6 Fast Metro ProjectJohn Vincent Macatangay CleofeNo ratings yet
- 2014pe Part IDocument12 pages2014pe Part IJohn Vincent Macatangay CleofeNo ratings yet
- 14-08-2020 - 2200 Hrs - LS 4G1 - DO - Fire Fighting PVC Pipe - DraftDocument12 pages14-08-2020 - 2200 Hrs - LS 4G1 - DO - Fire Fighting PVC Pipe - DraftJohn Vincent Macatangay CleofeNo ratings yet
- Corrective Action Report (Car) : Hse Line 6 Fast Metro ProjectDocument2 pagesCorrective Action Report (Car) : Hse Line 6 Fast Metro ProjectJohn Vincent Macatangay CleofeNo ratings yet
- Engineer & Supervisors List - LANDSCAPEDocument2 pagesEngineer & Supervisors List - LANDSCAPEJohn Vincent Macatangay CleofeNo ratings yet
- CONTROLDocument194 pagesCONTROLJohn Vincent Macatangay CleofeNo ratings yet
- Ser Line Exact Location Serial Number SupplierDocument8 pagesSer Line Exact Location Serial Number SupplierJohn Vincent Macatangay CleofeNo ratings yet
- Flood INDEXDocument171 pagesFlood INDEXJohn Vincent Macatangay CleofeNo ratings yet
- Protection in PlatDocument88 pagesProtection in PlatJohn Vincent Macatangay CleofeNo ratings yet
- Corrective Action Report (Car) : Hse Line 6 Fast Metro ProjectDocument3 pagesCorrective Action Report (Car) : Hse Line 6 Fast Metro ProjectJohn Vincent Macatangay CleofeNo ratings yet
- Line 04-LS/SS Schedule Section Finish Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov DecDocument5 pagesLine 04-LS/SS Schedule Section Finish Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov DecJohn Vincent Macatangay CleofeNo ratings yet
- Eyad-Swareb@sauditumpane, Com Andres - Deharo@fcc - Es No Work As of NowDocument1 pageEyad-Swareb@sauditumpane, Com Andres - Deharo@fcc - Es No Work As of NowJohn Vincent Macatangay CleofeNo ratings yet
- Note 4B1 Storm Water TrenchDocument2 pagesNote 4B1 Storm Water TrenchJohn Vincent Macatangay CleofeNo ratings yet
- Electrical Installation Inspection CARDocument3 pagesElectrical Installation Inspection CARJohn Vincent Macatangay CleofeNo ratings yet
- Corrective Action Report (Car) : Hse Line 6 Fast Metro ProjectDocument2 pagesCorrective Action Report (Car) : Hse Line 6 Fast Metro ProjectJohn Vincent Macatangay CleofeNo ratings yet
- Welcome To The LTE CPE!: Online HelpDocument44 pagesWelcome To The LTE CPE!: Online HelpJohn Vincent Macatangay CleofeNo ratings yet
- Updated Emergency Contact - Docx2 (2) 4b1 A3Document1 pageUpdated Emergency Contact - Docx2 (2) 4b1 A3John Vincent Macatangay CleofeNo ratings yet
- List of Short-Term Courses (TR) No. of Hours Fee Down PaymentDocument1 pageList of Short-Term Courses (TR) No. of Hours Fee Down PaymentJohn Vincent Macatangay CleofeNo ratings yet
- The Mechanical Properties of Polypropylene - Polylactic Acid (PP-PLA) Polymer Blends - 24 PagesDocument24 pagesThe Mechanical Properties of Polypropylene - Polylactic Acid (PP-PLA) Polymer Blends - 24 PagesSiddharthBhasneyNo ratings yet
- 1 Management Theories and PracticesDocument96 pages1 Management Theories and PracticesAsegid H/meskelNo ratings yet
- Case StudyDocument2 pagesCase StudyJoshua LaxamanaNo ratings yet
- Surajs Nair Resume 5Document4 pagesSurajs Nair Resume 5suraj.sNo ratings yet
- Sub District Sub Divisional HospitalDocument102 pagesSub District Sub Divisional HospitalGanesh SoniNo ratings yet
- QuadEquations PPT Alg2Document16 pagesQuadEquations PPT Alg2Kenny Ann Grace BatiancilaNo ratings yet
- Combustion Products From Ventilation Controlled Fires - Thesis PDFDocument321 pagesCombustion Products From Ventilation Controlled Fires - Thesis PDFYuri SanchezNo ratings yet
- Vendor Security Due Diligence ChecklistDocument9 pagesVendor Security Due Diligence ChecklistSukhveer SinghNo ratings yet
- Historical Change and Ceramic Tradition: The Case of Macedonia - Zoi KotitsaDocument15 pagesHistorical Change and Ceramic Tradition: The Case of Macedonia - Zoi KotitsaSonjce Marceva100% (2)
- DIY GREENHOUSE by KMS - ChangelogDocument4 pagesDIY GREENHOUSE by KMS - Changeloglm pronNo ratings yet
- De Thi Thu TN THPT 2024 Tieng Anh So GD Ha NoiDocument23 pagesDe Thi Thu TN THPT 2024 Tieng Anh So GD Ha NoiQuang Lê Hồ DuyNo ratings yet
- Crochetpatternturttle BenjaminDocument10 pagesCrochetpatternturttle BenjaminTere VValle100% (2)
- Research Compilation FinalDocument23 pagesResearch Compilation FinalJessa Mae LoredoNo ratings yet
- Driver Licence & Learner Permit FeesDocument9 pagesDriver Licence & Learner Permit FeesAnatoly IvanovNo ratings yet
- Technical CAPS Technical ScienceDocument84 pagesTechnical CAPS Technical ScienceqanaqNo ratings yet
- EDFD 211: Psychological Foundations in Education First Semester SY 2016-17 Course DescriptionDocument4 pagesEDFD 211: Psychological Foundations in Education First Semester SY 2016-17 Course DescriptionLeezl Campoamor OlegarioNo ratings yet
- IoT - Internet of Things Based Energy Management For Smart HomeDocument4 pagesIoT - Internet of Things Based Energy Management For Smart HomeEditor IJTSRDNo ratings yet
- Breach of ContractDocument26 pagesBreach of ContractSandeep100% (1)
- Aiga 097-17 Ref Guide On Medical Gases Cylinder ValvesDocument7 pagesAiga 097-17 Ref Guide On Medical Gases Cylinder ValvesDeepakNo ratings yet
- Surbir Singh Negi: Surbir99 - Negi@yahoo - Co.in, Surbir - Negi1@yahoo - Co.inDocument3 pagesSurbir Singh Negi: Surbir99 - Negi@yahoo - Co.in, Surbir - Negi1@yahoo - Co.insurbir_negi1100% (2)
- Fanuc 0ieDocument12 pagesFanuc 0ieangelNo ratings yet
- Siliporite Opx Pellets Revision 11 - 2017Document2 pagesSiliporite Opx Pellets Revision 11 - 2017Juan Victor Sulvaran Arellano100% (2)
- Ques Risk and Return & CAPM (S-17Revised)Document6 pagesQues Risk and Return & CAPM (S-17Revised)Najia SiddiquiNo ratings yet
- Guide To Supply Chain Management RemediationV2Document26 pagesGuide To Supply Chain Management RemediationV2Andrada-DianaFilipciucNo ratings yet
- PSI Framework Components - EnglishDocument20 pagesPSI Framework Components - Englishalejandrosag0% (1)
- Trophy Urban Core Property: Houston, TexasDocument25 pagesTrophy Urban Core Property: Houston, Texasbella grandeNo ratings yet